
Abstract
Purpose
Cervical sagittal balance has received increased attention as an important determinant of radiological and clinical outcomes. However, no prospective studies have compared the impact of cervical sagittal balance between anterior and posterior surgeries. We previously conducted a prospective study comparing anterior decompression with fusion (ADF) and laminoplasty (LAMP) for degenerative cervical myelopathy (DCM) and reported; however, analysis of cervical alignment within the concept of sagittal balance has yet to be performed, because that concept has recently been proposed. This study aimed to review this prospective cohort, specifically focusing on cervical sagittal balance.
Methods
We prospectively performed ADF or LAMP for DCM patients based on the year of enrollment: ADF was performed in odd-numbered years and LAMP in even-numbered years. Cervical lateral X-ray images taken in the neutral standing position were evaluated preoperatively and at a 1-year follow-up. The radiographic measurements included the following: (1) CL (cervical lordosis: C2–7 lordotic angle), (2) CGH (center of gravity of the head)-C7 SVA (sagittal vertical axis), and (3) C7 slope. The clinical results were evaluated using the Japanese Orthopedic Association scoring system for cervical myelopathy (C-JOA score).
Results
We analyzed the data for 66 patients (ADF n = 28, LAMP n = 38). While the CL and CGH-C7 SVA in the ADF were unchanged after the operation, those in the LAMP group worsened, especially in patients with preoperative cervical sagittal imbalance. The C7 slopes were not affected by the operation in either group. The postoperative decreases in the CL in the LAMP group correlated with the preoperative CGH-C7 SVA (r = 0.618, P < 0.01), but those in ADF group did not. In patients with preoperative cervical sagittal imbalance (CGH-C7 SVA ≥40 mm), the recovery rate of the C-JOA score in the ADF group was superior to that in the LAMP group (67.3 vs. 39.8 %). In contrast, for patients without cervical sagittal imbalance, the recovery rate of the C-JOA score showed no significant difference between the ADF and LAMP groups (64.5 vs. 58.7 %).
Conclusions
Postoperative cervical sagittal alignment and balance were maintained after ADF but deteriorated following LAMP, especially in patients with preoperative CGH-C7 SVA ≥40 mm. In these patients, neurological recovery after LAMP was unsatisfactory. LAMP is not suitable for degenerative cervical myelopathy patients with preoperative cervical sagittal imbalance.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Anterior decompression with fusion (ADF) and laminoplasty (LAMP) are standard surgical procedures for the treatment of degenerative cervical myelopathy (DCM) [5, 16]. To date, several studies have investigated post-surgical changes in cervical sagittal alignment [7, 8, 9, 17, 23, 27, 33]. Postoperative deterioration of cervical alignment, such as a kyphotic deformity, has occasionally been observed, and studies have indicated that this deterioration has worsened clinical outcomes, especially after LAMP [10, 12, 27].
Recently, cervical sagittal balance has been identified as an important determinant of radiological and clinical outcomes following cervical surgeries as well as thoracolumbar spinal surgeries [19, 22, 34]. However, little is known about the precise impact of cervical sagittal balance. Furthermore, no prospective studies have compared the impact of cervical sagittal balance between anterior and posterior surgeries.
We previously conducted a prospective study comparing ADF and LAMP in the treatment of DCM and reported the radiological and clinical outcomes [7]. However, because the concept of cervical sagittal balance has been recently proposed, detailed analysis of cervical alignment within the concept of sagittal balance has yet to be performed. In this study, we reviewed the changes in cervical sagittal alignment and neurological outcomes, focusing specifically on cervical sagittal balance, in the prospective comparative cohort between the ADF and LAMP.
Materials and methods
Materials
A total of 76 consecutive patients with DCM were included in this prospective study. Each patient underwent a cervical surgery, ADF or LAMP, at our hospital between 1996 and 2003 and provided adequate informed consent. Exclusion criteria included the presence of myelopathy caused by cervical disc herniation or ossification of the posterior longitudinal ligament and any history of a previous cervical spine surgical intervention or injury. In addition, patients who could not maintain an upright position without assistance or who did not receive a standing X-ray preoperatively were excluded.
Choice of surgical procedure
The patients were divided into two groups based on the year of enrollment. A total of 34 patients was enrolled in the ADF group in 1997, 1999, 2001, and 2003, and 42 patients were enrolled in the LAMP group in 1996, 1998, 2000, and 2002.
Operative procedure
Anterior decompression with fusion
Operative segments were selected on the basis of the findings from radiological studies and preoperative spinal cord-evoked potentials recorded from an epidural electrode. Discectomy was performed for 1-level lesion, and corpectomies were performed for 2-level lesion or more. The cervical spine was reconstructed using an autologous bone with plate and screw fixation. The autologous bone was harvested from an iliac crest for less than 2-level and a fibula for 3-level or more. The patient’s neck was immobilized externally using a collar for 2–3 months.
Laminoplasty
The double door LAMP without lamina spacer was performed. The paravertebral muscles were detached from the spinous processes on both sides and the processes at C3–6 were removed. The laminae at C3–6 were split at the midline, and bilateral gutters were fashioned using a high-speed air-burr drill. The bilateral laminae were kept open by sutures to the capsule of the facet joint. Small bone chips made from the removed spinous processes were inserted into the bilateral gutters. For patients who had spinal cord compression at the C2/3 level, the inferior lamina at C2 was fenestrated. For patients who had spinal cord compression at the C6/7 level, the superior lamina at C7 was fenestrated. In all patients, the C2 and C7 spinous processes and the paravertebral muscles that were attached to these spinous processes were preserved. The patient’s neck was immobilized externally using a collar for 3–4 weeks.
Outcome measures
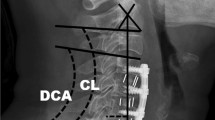
Cervical lateral plane X-ray images obtained in the standing position were measured at the preoperative stage and at a 1-year follow-up visit. The radiographic measurements included the following: (1) CL (cervical lordosis: C2–7 lordotic angle), (2) CGH (center of gravity of the head)-C7 SVA (cervical sagittal vertical axis), which is the distance between the anterior margin of the external auditory canal plumb line and the posterior-cranial corner of the C7 vertebral body [34], and (3) C7 slope (Fig. 1). The clinical results were evaluated using the Japanese Orthopedic Association score system for cervical myelopathy (C-JOA score) at the preoperative stage and at a 1-year follow-up. The recovery rate (RR) of the C-JOA score was calculated using Hirabayashi’s method [6].

Radiographic measurements. a CL (cervical lordosis: C2–7 lordotic angle). b CGH (center of gravity of the head)-C7 SVA (cervical sagittal vertical axis). c C7 slope
Statistics
Statistical analysis was performed using SPSS for Windows version 19.0 (SPSS Institute, Chicago, IL). The Student unpaired t test, the Mann–Whitney U test, and the χ 2 test were used to compare the differences between the ADF group and the LAMP group, and the Student paired t test was used to examine the differences between the preoperative and postoperative data in both groups. The Pearson correlation coefficient was used to evaluate the relationships between a postoperative decrease in CL and the preoperative factors. Furthermore, a single linear regression analysis was used to determine the relationship between the postoperative decrease in CL and the CGH-C7 SVA in the LAMP group. A statistically significant difference was set at P < 0.01 and 0.05.
Results
Patient demographics
Seventy-two of 76 patients completed the 1-year follow-up. The remaining 4 patients could not be followed and so data were missing for these patients. Six patients could not obtain completely data, because the external auditory canal or C7 vertebra could not see clearly in the X-ray images. We analyzed 66 (86.8 %; 50 males, 16 females) of the 76 patients. The patients received ADF in 28 cases (ADF group) and LAMP in 38 cases (LAMP group). The patients’ demographic data are shown in Table 1. There were no significant differences in the age at surgery, gender, the C-JOA score, duration of symptom, the number of cord compression levels on magnetic resonance imaging, the CL, the CGH-C7 SVA, and the C7 slope between the two groups prior to surgery. The number of operative segments in the ADF group was less than that in the LAMP group (P < 0.01).
Postoperative outcomes
While the operation had no effect on the CL and CGH-C7 SVA in the ADF group, they worsened following the operation in the LAMP group (individually, P < 0.01, P < 0.01). The operation had no effect on the C7 slopes in either group. The postoperative CL and CGH-C7 SVA in the ADF group were superior to those in the LAMP group (individually, P < 0.05, P < 0.05) (Table 2).
While the C-JOA scores in both groups improved after surgery, there were no significant differences in the postoperative C-JOA score or the RR of the C-JOA score between the ADF and LAMP groups.
Correlations between postoperative decrease in cervical lordosis and the preoperative or operative factors
We investigated which preoperative or operative factors, including preoperative CL, CGH-C7 SVA, C7 slope, and the number of operative segments influenced the postoperative decrease in the CL (preoperative CL–postoperative CL) by Pearson correlation coefficient analysis (Table 3). The decrease in the CL positively correlated with the preoperative CGH-C7 SVA in the LAMP group (Pearson correlation coefficient value (r) = 0.618, P < 0.01, Fig. 2); however, no such correlation was observed in the ADF group. There were no correlations between the postoperative decrease in CL and either the other preoperative factors or number of operative segments in either group. Therefore, the cervical alignment was influenced by the preoperative cervical sagittal balance in the LAMP group, but not in the ADF group.

Correlations between the postoperative decrease of CL and the preoperative CGH-C7 SVA in the LAMP group
Impact of preoperative cervical sagittal balance for surgical outcomes
In addition, we focused on the preoperative cervical sagittal balance and divided the patients into two subgroups based on the preoperative CGH-C7 SVA: the Imbalance was defined as a CGH-C7 SVA ≥40 mm in accordance with the previous studies [19, 27, 34] (Imbalance subgroup) and the Balance was CGH-C7 SVA <40 mm (Balance subgroup). Nine (13.6 %) of the 66 patients exhibited preoperative cervical sagittal imbalance (4 patients in the ADF group, 5 patients in the LAMP group).
We compared the outcomes between the ADF group and LAMP group for both of the subgroups (Table 4). The preoperative demographics showed no statistically significant differences between the ADF and LAMP groups in either subgroup. For the Imbalance subgroup, while the operation had no effect on the CL in the ADF group, that in the LAMP group worsened following the operation (P < 0.05), and the postoperative CL in the LAMP group was inferior to those in the ADF group (P < 0.05) (Fig. 3). Although all of five patients following LAMP in the Imbalance subgroup had a cervical lordosis alignment preoperatively (CL >0°), all of them occurred the postoperative kyphotic deformity (CL <0°). In the Balance subgroup, the postoperative CL and CGH-C7 SVA were not significantly different between the ADF and LAMP groups. These results indicate that the cervical sagittal alignment of the patients with preoperative cervical sagittal imbalance deteriorates after LAMP, and not after ADF (Fig. 4).

Postoperative changes of the CL in comparison between ADF and LAMP in patients with preoperative cervical sagittal Imbalance and Balance subgroups.  P < 0.05
P < 0.05

Preoperative X-ray image a of a 61-year-old man with cervical sagittal imbalance (CGH-C7 SVA: 58 mm). An X-ray image at a 1-year follow-up after C3–6 ADF b showed that the cervical lordosis was maintained. A preoperative X-ray image c of a 50-year-old man with cervical sagittal imbalance (CGH-C7 SVA: 50 mm). Although he had cervical lordotic alignment, an X-ray image at a 1-year follow-up after LAMP d showed postoperative kyphotic deformity
In the Imbalance subgroup, the RR of the C-JOA score in the ADF group was superior to that in the LAMP group (67.3 vs. 39.8 %, P < 0.05) (Fig. 5). In contrast, in the Balance subgroup, the RR of the C-JOA score showed no significant difference between the ADF and LAMP groups (64.5 vs. 58.7 %).

Recovery rate of the C-JOA score in comparison between ADF and LAMP in patients with preoperative cervical sagittal Imbalance and Balance subgroups.
P < 0.05
Discussion
ADF can achieve a direct anterior decompression and stabilize the spinal column. On the other hand, LAMP generates a direct posterior decompression effect and an indirect anterior decompression effect resulting from the posterior shift of the spinal cord from the anterior compressive lesions. Therefore, postoperative posterior cord shift was needed [2, 31], and it is known that LAMP is not suitable for patients with preoperative cervical kyphosis [18, 28, 32]. However, we sometimes encounter patients who develop postoperative kyphosis, despite normal preoperative cervical alignment. Sakai et al. reported that the kyphotic deformity after LAMP for DCM patients without preoperative kyphotic alignment occurred in 5.2 % [27]. In this study, whereas we did not decide to exclude patients with excessive cervical kyphosis, because it had been unclear whether the cervical kyphosis was, in fact, related to postoperative outcome at the beginning of this study, we included no patient with preoperative excessive kyphosis over 10°: however, postoperative kyphotic deformity over 10° occurred in 7.8 % of the patients following LAMP. It suggests that factors other than preoperative cervical alignment involve occurrence of postoperative kyphotic deformity following LAMP.
In recent years, the concept of sagittal balance based on cervical SVA was proposed in the cervical spine. Cervical sagittal balance has been found to affect the HR-QOL of patients similar to the thoracolumbar spine. Oe et al. examined a sample of healthy volunteers and reported that cervical sagittal imbalance negatively influenced HR-QOL [19]. Protopsaltis et al. showed that improvement in the cervical sagittal balance following corrective surgery for thoracolumbar deformity was related to HR-QOL improvement [22]. Tang et al. found that HR-QOL was associated with postoperative cervical sagittal balance based on cervical SVA [34]. Based on the results of these studies, the cervical sagittal balance appears to closely correlate with patients’ HR-QOL.
Several studies have addressed changes in cervical alignment, focusing on sagittal balance before and after cervical surgeries. Kim et al. reported that cervical sagittal balance was maintained after anterior cervical discectomy with fusion for DCM patients [11]. Chen et al. also demonstrated that cervical sagittal balance was improved following anterior cervical corpectomy with fusion for myelopathy patients due to ossification of the posterior longitudinal ligament (OPLL) [3]. On the other hand, Lin et al. reported that cervical SVA in DCM patients is worsened after LAMP [14]. Lee et al. reported that cervical sagittal balances deteriorated after laminectomy and LAMP in myelopathic patients due to OPLL [13]. Sakai et al. reported that cervical SVA was worse after LAMP for DCM patients; moreover, preoperative sagittal imbalance was a risk factor of kyphotic deformity after LAMP, and neurological recovery in patients with the kyphotic deformity was poor [27]. Although these previous studies implied the superiority of the anterior procedure over the posterior in preventing postoperative cervical imbalance and malalignment, no prospective studies have directly compared anterior and posterior procedures in terms of postoperative changes in the sagittal alignment, balance, and clinical outcomes. We previously conducted prospective studies and reported comparing anterior decompression with fusion (ADF) and laminoplasty (LAMP) for DCM [7] and OPLL [26]. Therefore, we reviewed the influence of surgical procedures (anterior or posterior) on the cervical alignment change and neurological recovery, with a focus on the sagittal balance using the prospective ADF and LAMP cohorts for DCM.
This study yielded important findings: (1) the postoperative CL and cervical sagittal balance after ADF were maintained; however, those after LAMP worsened, especially in the patients with preoperative cervical sagittal imbalance; (2) the postoperative decrease of CL was correlated with preoperative CGH-C7 SVA in the LAMP group, but not in the ADF group; and (3) in the patients with preoperative cervical sagittal imbalance, neurological recovery in the LAMP group was inferior to that in the ADF group.
In cervical sagittal imbalanced patients, it is well known that CL is increased to compensate for the balance adjustment or forward gazing, and thus, CL closely correlates with cervical sagittal balance [1, 21]. In fact, the preoperative cervical alignment type for all of the cervical imbalanced patients was lordosis in this study. In the imbalanced state, the cervical extensor muscles play a critically important role in maintaining the lordosis of the cervical spine. For these conditions, it is speculated that the invasion in the posterior extension mechanism by LAMP causes postoperative cervical malalignment. Furthermore, it may interrupt the posterior cord shift or generate an anterior impingement of the spinal cord, ultimately resulting in impairment of the neurological recovery. On the other hand, ADF does not damage these posterior muscles at all, because of its approach from the anterior-lateral intermuscular planes. Therefore, ADF may maintain the cervical alignment and balance after surgery and lead to good neurological recovery even in such cases. Based on the results of our study, posterior decompression alone should not be applied to patients with preoperative cervical sagittal imbalance.
To determine the surgical procedure, of course, overall judgment should be exercised based on the patient’s general condition, comorbidities, and complications. In cases where to the anterior procedure would be more difficult to perform, alternative posterior procedures may be viable choices. In this study, we performed the conventional LAMP (at least C3–6 even if 1 level lesion) to achieve posterior spinal cord shift certainly. However, recently, various minimally invasive posterior decompression procedures, such as muscle preserving LAMP, skip laminectomy (LAM), or selective LAM, were reported [25, 29, 30, 35]. Shiraishi et al. showed cervical curvature index after skip LAM was superior to the conventional LAMP [29], and selective LAM also could retain postoperative cervical alignment [30]. Lin et al. reported that postoperative cervical alignment and balance after muscle preserving LAMP were superior to those after the conventional LAMP [15]. Posterior decompression with fusion (PDF) may also be another choice [24]. Miyamoto et al. reported that postoperative cervical alignment and neurological recovery following PDF were superior to LAMP in DCM patients with local kyphosis [18]. Lee et al. reported that PDF could maintain cervical sagittal alignment, but not LAM/LAMP, in myelopathic patients due to OPLL [13]. However, we think more studies assessing theses alternative procedures were needed, because it is still unclear the impact of preoperative sagittal balance on these surgical outcomes.
The potential limitations of this study include the relatively small cohort size. In addition, the relationship between the cervical parameters and thoracolumbar or spinopelvic parameters could not be confirmed, because the whole sagittal radiograph was not used. Recently, cervical sagittal alignment or surgical outcomes were recognized to be affected by thoracolumbar alignment and balance. Diebo et al. reported that cervical lordosis was increased to maintain horizontal gaze in patient with C7-SVA >50 mm and greater thoracic kyphosis [4]. Jalai et al. reported thoracolumbar corrective surgery for adult spinal deformity resulted in higher cervical deformity rates [8]. Oshima et al. said that postoperative functional outcome scores following LAMP were significantly lower in patients with C7-SVA > 50 mm [20]. More prospective studies with large populations, including whole spine sagittal radiographs, to assess the postoperative change in cervical alignment or balance are needed. Although further investigations remain necessary, our findings demonstrate that postoperative cervical sagittal alignment and balance were maintained after ADF yet deteriorated following LAMP. ADF is preferred to LAMP especially for patients with cervical sagittal imbalance.
Conclusions
Postoperative cervical sagittal alignment and balance were maintained after ADF, but deteriorated following LAMP, especially in patients with preoperative CGH-C7 SVA ≥40 mm. In these patients, neurological recovery after LAMP was unsatisfactory. LAMP is not suitable for degenerative cervical myelopathy patients with preoperative cervical sagittal imbalance.
References
Ames CP, Blondel B, Scheer JK et al (2013) Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine (Phila Pa 1976) 38(22 Suppl 1):S149–S160. doi:10.1097/BRS.0b013e3182a7f449
Baba H, Uchida K, Maezawa Y et al (1996) Lordotic alignment and posterior migration of the spinal cord following en bloc open-door laminoplasty forcervical myelopathy: a magnetic resonance imaging study. J Neurol 85:626–632
Chen Y, Yang L, Liu Y et al (2014) Surgical results and prognostic factors of anterior cervical corpectomy and fusion for ossification of the posterior longitudinal ligament. PLoS One 9(7):e102008. doi:10.1371/journal.pone.0102008
Diebo BG, Challier V, Henry JK et al (2016) Predicting cervical alignment required to maintain horizontal gaze based on global spinal alignment. Spine (Phila Pa 1976) [Epub ahead of print]
Fehling MG, Ibrahim A, Tetreault L et al (2015) A global perspective on the outcomes of surgical decompression in patients with cervical spondylotic myelopathy: result from the prospective multicenter AOSpine international study on 479 patients. Spine (Phila Pa 1976) 40(17):1322–1328. doi:10.1097/BRS.0000000000000988
Hirabayashi K, Miyakawa J, Satomi K, Maruyama T, Wakano K (1981) Operative results and postoperative progression among patients with ossification of cervical posterior longitudinal ligament. Spine (Phila Pa 1976) 6:354–364
Hirai T, Okawa A, Arai Y et al (2011) Middle-term results of a prospective comparative study of anterior decompression with fusion and posterior decompression with laminoplasty for the treatment of cervical spondylotic myelopathy. Spine (Phila Pa 1976) 36(23):1940–1947. doi:10.1097/BRS.0b013e3181feeeb2
Jalai CM, Passias PG, Lafage V et al (2016) A comparative analysis of the prevalence and characteristics of cervical malalignment in adults presenting with thoracolumbar spine deformity based on variations in treatment approach over 2 years. Eur Spine J [Epub ahead of print]
Jiang L, Tan M, Dong L et al (2015) Comparison of anterior decompression and fusion with posterior laminoplasty for multilevel cervical compressive myelopathy: a systematic review and meta-analysis. J Spinal Disord Tech 28(8):282–290. doi:10.1097/BSD.0000000000000317
Kawaguchi Y, Kanamori M, Ishihara H et al (2013) Minimum 10-year followup after en bloc cervical laminoplasty. Clin Orthop Relat Res 411:129–139
Kim JH, Park JY, Yi S et al (2015) Anterior cervical discectomy and fusion alters whole-spine sagittal alignment. Yonsei Med J 56(4):1060–1070. doi:10.3349/ymj.2015.56.4.1060
Kimura I, Shingu H, Nasu Y (1995) Long term follow-up of cervical spndylotic myelopathy treated by canal-expansive laminoplasty. J Bone Joint Surg Br 77(6):956–961
Lee CH, Jahng TA, Hyun SJ, Kim KJ, Kim HJ (2016) Expansive laminoplasty versus laminectomy alone versus laminectomy and fusion for cervical ossification of the posterior longitudinal ligament: is there a difference in the clinical outcome and sagittal alignment? Clin Spine Surg 29(19):E9–E15. doi:10.1097/BSD.0000000000000058
Lin S, Zhou F, Sun Y et al (2014) Changes of sagittal balance of cervical spine after open-door expansive laminoplasty. Zhonghua Yi Xue Za Zhi 94(35):2726–2730
Lin S, Zhou F, Sun Y et al (2015) The severity of operative invasion to the posterior muscular-ligament complex influences cervicalsagittal balance after open-door laminoplasty. Eur Spine J 24(1):127–135. doi:10.1007/s00586-014-3605-3
Liu X, Min S, Zhang H et al (2014) Anterior corpectomy versus posterior laminoplasty for multilevel cervical myelopathy: a systematic review and meta-analysis. Eur Spine J 23(2):362–372. doi:10.1007/s00586-013-3043-7
Matsunaga S, Sakou T, Nakanisi K (1999) Analysis of the cervical spine alignment following laminoplasty and laminectomy. Spinal Cord 37(1):20–24
Miyamoto H, Maeno K, Uno K et al (2014) Outcomes of surgical intervention for cervical spondylotic myelopathy accompanying local kyphosis (comparison between laminoplasty alone and posterior reconstruction surgery using the screw-rod system). Eur Spine J 23(2):341–346. doi:10.1007/s00586-013-2923-1
Oe S, Togawa D, Nakai K et al (2015) The influence of age and sex on cervical spinal alignment among volunteers aged over 50. Spine (Phila Pa 1976) 40(19):1487–1494. doi:10.1097/BRS.0000000000001071
Oshima Y, Takeshita K, Taniguchi Y et al (2016) Effect of preoperative sagittal balance on cervical laminoplasty outcomes. Spine (Phila Pa 1976) [Epub ahead of print]
Patwardhan AG, Havey RM, Khayatzadeh S et al (2015) Posture consequences of cervical sagittal imbalance: a novel laboratory model. Spine (Phila Pa 1976) 40(11):783–792. doi:10.1097/BRS.0000000000000877
Protopsaltis TS, Scheer JK, Terran JS et al (2015) How the neck affects the back: changes in regional cervical sagittal alignment correlate to HRQOL improvement in adult thoracolumbar deformity patients at 2-year follow-up. J Nuerosurg Spine 23(2):153–158. doi:10.3171/2014.11.SPINE1441
Qian L, Shao J, Liu Z et al (2014) Comparison of the safety and efficacy of anterior ‘skip’ corpectomy versus posterior decompression in the treatment of cervical spondylotic myelopathy. J Orthop Surg Res 9:63. doi:10.1186/s13018-014-0063-x
Ratliff JK, Cooper PR (2003) Cervical laminoplasty: a critical review. J Neurosug 98(3 Suppl):230–238
Roselli R, Pompucci A, Formica F et al (2000) Open-door laminoplasty for cervical stenotic myelopathy: surgical technique and neurophysiological monitoring. J Neurosurg 92(1 Suppl):38–43
Sakai K, Okawa A, Takahashi M et al (2012) Five-year follow-up of surgical treatment caused by ossification of the posterior longitudinal ligament: a prospective comparative study of anterior decompression and fusion with floating method versus laminoplasty. Spine (Phila Pa 1976) 37(5):367–376. doi:10.1097/BRS.0b013e31821f4a51
Sakai K, Yoshii T, Hirai T et al (2016) Cervical sagittal imbalance is a predictor of kyphotic deformity after laminoplasty in cervical spondylotic myelopathy patients without preoperative kyphotic alignment. Spine (Phila Pa 1976) 41(4):299–305. doi:10.1097/BRS.0000000000001206
Shamji MF, Mohanty C, Massicotte EM, Fehlings MG (2016) The association of cervical spine alignment with neurologic recovery in a prospective cohort of patients with surgical myelopathy: analysis of a series of 124 cases. World Neurosurg 86:112–119. doi:10.1016/j.wneu.2015.09.044
Shiraishi T, Fukuda K, Yato Y, Nakamura M, Ikegami T (2003) Results of skip laminectomy-minimum 2-year follow-up study compared with open-door laminoplasty. Spine (Phila Pa 1976) 28(24):2667–2672
Shiraishi T, Kato M, Yato Y et al (2012) New techniques for exposure of posterior cervical spine through intermuscular planes and their surgical application. Spine (Phila Pa 1976) 37(5):E286–E296. doi:10.1097/BRS.0b013e318239cc7e
Sodeyama T, Goto S, Mochizuki M, Takahashi J, Moriya H (1999) Effect of decompression enlargement laminoplasty for posterior shifting of the spinal cord. Spine (Phila Pa 1976) 24(15):1527–1531
Suda K, Abumi K, Ito M et al (2003) Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine (Phila Pa 1976) 28(12):1258–1262
Suk KS, Kim KT, Lee JH et al (2007) Sagittal alignment of the cervical spine after the laminoplasty. Spine (Phila Pa 1976 32(23):E656–E660
Tang JA, Scheer JK, Smith JS et al (2012) The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery 71(3):662–669. doi:10.1227/01.neu.0000462074.66077.2b
Traynelis VC, Arnold PM, Fourney DR et al (2013) Alternative procedures for the treatment of cervical spondylotic myelopathy: arthroplasty, oblique corpectomy, skip laminectomy: evaluation of comparative effectiveness and safety. Spine (Phila Pa 1976) 38(22 Suppl 1):S210–S231. doi:10.1097/BRS.0000000000000009
Acknowledgments
We gratefully acknowledge Dr. Satoru Egawa to help our work. This work was supported by Japanese Health Labour Sciences Research Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Sakai, K., Yoshii, T., Hirai, T. et al. Impact of the surgical treatment for degenerative cervical myelopathy on the preoperative cervical sagittal balance: a review of prospective comparative cohort between anterior decompression with fusion and laminoplasty. Eur Spine J 26, 104–112 (2017). https://doi.org/10.1007/s00586-016-4717-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4717-8