
Abstract
Purpose
To analyze the sagittal thoracic parameters of different types of progressive thoracic adolescent idiopathic scoliosis (AIS) patients and compare them with healthy adolescents.
Methods
115 AIS patients with main thoracic curves (Cobb: 59.4 ± 12.7) were prospectively compared with 116 healthy adolescents. The AIS and control (C) groups were homogeneous in terms of age and gender. Standing sagittal radiographs were analyzed for differences in T5–T12 kyphosis, T5–T8 and T9–T12 segmental kyphosis, the change between these two angles, and the double rib contour sign. Statistical analyses were performed using the χ 2, one-way ANOVA, Mann–Whitney U and Student’s t tests.
Results
The sagittal parameters of Lenke 1 curves did not differ from healthy adolescents (T5–T8: 17.1 ± 10 vs C: 16 ± 7; T9–T12: 6.3 ± 7 vs C: 7.9 ± 5; T5–T12: 23.9 ± 14 vs C: 23.9 ± 8). Compared with the controls, Lenke type 3 curves were globally more hypokyphotic (T5–T12: 18.9 ± 12 vs C: 23.9 ± 8, P = 0.027) due to a “lordosis” of the lower thoracic segment (T9–T12: 0.9 ± 10 vs C: 7.9 ± 5, P = 0.001). Type 2 curves tended to exhibit more pronounced upper thoracic kyphosis (T5–T8: 20.7 ± 12 vs C: 16 ± 7). Both types 2 and 3 require a marked TK changes in the transition between the upper and lower thoracic segments to compensate for global (T5–T12) kyphosis.
Conclusions
In this 2D analysis of moderate AIS, Lenke 1 curves exhibited normal thoracic sagittal parameters, which brings into question the effect of lordosis on the development of single thoracic curves. Lenke 3 curves exhibited lower thoracic segmental hypokyphosis, and the type 2 showed upper segmental hyperkyphosis. These results should be considered when planning a surgical strategy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Historically, we have considered that the thoracic kyphosis is smaller for thoracic adolescent idiopathic scoliosis (AIS) curves when compared with those of asymptomatic controls [1–6]. Idiopathic thoracic curves are believed to be induced by this thoracic hypokyphosis [7–9]. The apical vertebral bodies are wedged shaped, with an increased anterior vertebral height, which results in a longer anterior column and a shorter posterior column [1, 10]. This anterior spinal overgrowth is thought to be due to disproportionate endochondral and intramembranous bone formation [11]. With the further flexion of a pre-existing coronal plane asymmetry, this lordosis creates a spinning moment that causes the spine to rotate and create three-dimensional scoliosis [1]. Recently, 3D image reconstructions have confirmed the presence of this local hypokyphosis [12] in thoracic scoliosis, reaffirming this theory and enhancing the importance of restoring the appropriate kyphosis when correcting these curves [4, 13].
However, these concepts are still opened to debate. Some authors have found no significant difference in thoracic kyphosis between patients with scoliosis and controls [14–16]. Based on the 3D reconstruction analyses, it has been reported that thoracic curves are not always hypokyphotic [17]. Indeed, half of Lenke 1 (main thoracic deformity) curves have been found to be normokyphotic when the global kyphosis is considered [18, 19]. Furthermore, local apical hypokyphosis has recently been considered to be more strongly related to curve progression than an initiating factor in the pathogenesis of idiopathic scoliosis [3, 15, 20].
Thoracic kyphosis in normal children is considerably reduced in early adolescence and reaches a minimum at approximately age 12 [9, 21, 22]. Consequently following this principle, all children of this age, whether asymptomatic or not, should have a straighter thoracic spine. Thus, our hypothesis is that the sagittal thoracic planes of patients with moderate thoracic idiopathic curves in the adolescent period are straight but similar to those of healthy patients of the same age.
The purpose of the current study was to analyze in 2D the sagittal parameters of different types of progressive thoracic AIS and compare them with the same parameters in healthy adolescents.
Materials and methods
We retrospectively registered the preoperative data of a consecutive series of patients with AIS and main thoracic deformity (Lenke type 1–4) who were scheduled for surgery at a single institution. Non-idiopathic deformities and main lumbar curves were excluded. Next, a prospective consecutive cohort of healthy adolescents who were being examined with standing AP and lateral thoracic radiographs due to respiratory benign concerns (asthma, bronchitis, etc.) were registered and used as controls (C group). The cohorts were found homogeneous in terms of age and gender.
Radiographic analyses were performed on digitalized coronal and lateral radiographs of the spines taken with patients in standing positions to determine the different measures. In the coronal plane, the coronal Cobb angle and the Lenke curve type (for the AIS group) were recorded. Two experienced attending spine surgeons measured all the radiographic data.
The standing sagittal radiographs of both groups were analyzed to identify differences in the following measures: T5–T12 kyphosis (measured from the upper endplate of T5 to the lower endplate of T12); T5–T8 segmental kyphosis (measured from the upper endplate of T5 to the lower endplate of T8); T9–T12 segmental kyphosis (measured from the upper endplate of T9 to the lower endplate of T12); and the change between these two angles (TK Change), which was calculated by the subtraction of the two former angles. As reported in the literature, thoracic kyphosis in AIS is divided in a caudal hypokyphosis and a cranial hyperkyphosis and the turning point between these two zones corresponded to the plane of maximal rotation, which has been determined in T9. Following these reports, thoracic segmental kyphosis was measured with a cut-off at T9 [19, 23].
Rib cage deformity was also assessed by measuring the rib index or the double rib contour sign (DRCS) at the apex of the thoracic curve. The rib index was defined as the ratio of the distance of the posterior margin of the vertebral body to the most extended point of the most projecting rib contour, divided by the distance between the posterior margin of the same vertebral body and the most protruding point of the least projecting rib contour as described by Grivas [24]. In healthy adolescents, this index was always measured at T9 because this location was found to be the prevalent level at which the thoracic coronal apex was located in the AIS group, and therefore the most rotated.
The statistical analysis was performed with SPSS software (version 20, SAS Institute Inc., Cary, NC, USA). The distributions of the variables are given as the means and standard deviations. For the quantitative analyses, the Mann–Whitney U test was used for non-parametric variables, and Student’s t test was used for parametric variables. The qualitative data were compared with the χ 2 test. The sagittal alignments for all curve types and healthy adolescents were compared using analysis of variance (ANOVA) to determine the statistical significance. The level of significance was set at 0.05.
Results
Two hundred and thirty-one patients were included in the study. One hundred and fifteen AIS patients with main thoracic curves (coronal Cobb angle: 59.4° ± 12.7) were compared with 116 healthy adolescents (coronal Cobb angle: 1.7° ± 3.8). The mean ages (AIS: 14.9 ± 1.9 years vs. C: 14.8 ± 0.9 years) and gender distributions (AIS female: 80 % vs. C female: 70 %) were homogeneous (P > 0.05) between the groups. All patients were white caucasians (Table 1). No Lenke type 4 curves were encountered; thus, Lenke types 1, 2 and 3 curves were further analyzed and compared with controls. The rib index was found to be significantly different between the AIS patients (2.7 ± 1.3) and controls (1.4 ± 0.3; P = 0.000).
In general, the thoracic AIS curves exhibited global T5–T12 thoracic kyphosis that was similar to that of the controls. The AIS patients were more hypokyphotic than the healthy adolescents in the lower thoracic segment (T9–T12: 4.9° ± 8.2 vs. 7.9° ± 5.1, P = 0.000) and exhibited a greater TK change (12.8° ± 12.7 vs. 8.7° ± 8.4, P = 0.001), which ultimately resulted in the same global kyphosis, T5–T12 of 23° (Table 2).
The sagittal parameters (T5–T12, T5–T8, T9–T12, and TK Change) of the Lenke type 1 curves did not differ significantly from those of the healthy adolescents (Table 3).
The type 2 curves tended to be slightly more hyperkyphotic than the other curves (TK T5–T12: 26.6° ± 13.3) and exhibited more kyphotic upper thoracic segments (T5–T8: 20.7° ± 12.1 vs. 16° ± 7) than those of the control group; however, these differences did not reach significance (P > 0.05). Because the Lenke type 2 patients were slightly more hypokyphotic in the lower thoracic segment than the control group (T9–T12: 5.6° ± 4.3 vs. 7.9° ± 5.1; P = 0.028), they required a greater TK change (15.1° ± 12.5 vs. 8.7° ± 8.4; P = 0.019) to finally achieve global thoracic balance (Table 4).
Compared with the controls, the Lenke type 3 curves were globally more hypokyphotic (T5–T12: 18.9° ± 12 vs. C: 23.9° ± 8, P = 0.027) due to a “lordosis” of the lower thoracic segment (T9–T12: 0.9° ± 10 vs C: 7.9° ± 5, P = 0.001). This lower segment hypokyphosis required a marked TK change in the transition between the upper and lower thoracic segments (16.1° ± 15.5 vs. 8.7° ± 8, P = 0.013) to compensate for the global (T5–T12) kyphosis (Tables 5, 6).
Discussion
There is controversy in the literature (Table 7), as whether AIS patients present normal values of thoracic kyphosis, because reported values on normal adolescents show disparity between authors. Before and at the peak of the growth spurt, healthy children have smaller thoracic kyphosis and more posterior inclination of individual vertebrae as compared to after the peak of the growth spurt [21, 25]. So thoracic kyphosis in normal children is believed to be considerably reduced in early adolescence, reach a minimum at approximately the age of 12, and later grow and establish normal values at the end of growth [9, 21]. Normal thoracic kyphosis has commonly been described to range from 20° to 40° [2, 4, 26], although reference values ranging from 10° to 50° have also been suggested [27, 28], with no difference between males and females [29]. Upasani and Mac-Thiong estimate thoracic kyphosis in healthy adolescents to be 27° and 44°, respectively [3, 30], and Lenke’s classification only considers curves as hypokyphotic if the sagittal Cobb is less than 10° [31].
The majority of reports have found very similar values of thoracic kyphosis among thoracic AIS curves, ranging from 18° to 33°, with a pooled mean of 23.8° [16] (Table 7). Our figures (23°) are similar to those published [2–6, 32, 33]. And with these figures in hand, many authors have reported that thoracic kyphosis is smaller in thoracic AIS curves than in controls.
In contrast, some authors have found no significant differences in thoracic kyphosis between patients with scoliosis and controls [14, 15]. Based on the 3D reconstruction analyses, some authors have demonstrated that thoracic curves are not always hypokyphotic and can be divided into different groups based on the location of the plane of the maximum deformity, whether the curves are in a lordotic or kyphotic area [17, 23]. Indeed these authors have proved that half of Lenke type 1 curves are normokyphotic with an average T4–T12 kyphosis of 33°, which could explain why normokyphosis values in the range of 10° to 40° (N) are the most common sagittal thoracic modifiers observed in AIS based on the Lenke classification (75 % of the patients), while hypokyphosis (−) represents only the 14 % [31]. Recently Ries has demonstrated with plain radiographs, that adolescents with Lenke I or II curves have comparable sagittal profiles with those of healthy controls of the same age, suggesting that Lenke I and II curves may not be hypokyphotic as previously thought [16].
Considering only the global kyphosis, we can say based on our results that thoracic AIS patients exhibit a low T5–T12 thoracic kyphosis similar to that of healthy peers of the same age. This thoracic kyphosis is straight, with values falling in the lower range of normality. Thus, the theory that a straighter spine is present during the growth spurt of adolescence (in both AIS and asymptomatic patients) seems reasonable [9, 21, 22, 25].
One well-consolidated theory supports that progressive AIS is attributable to relative anterior spinal overgrowth that leads to thoracic hypokyphosis primarily in the two or three most apical segments of the spine, which is followed by increasing axial rotational instability [7, 8, 34]. Recent 3D reconstructions of thoracic scoliosis spines have reaffirmed a consistent loss of kyphosis within the five thoracic apical vertebrae [12].
However, some controversy has recently arisen. Some authors have observed that thoracic hypokyphosis is strongly related to curve progression [3, 15, 20] and to Roussouly’s sagittal type 3 and 4 profiles, showing greater pelvic incidence and lumbar lordosis in patients compared with healthy controls [2, 3, 6]. Together, these findings suggest that by facilitating axial rotation, this reduced kyphosis could be viewed as being permissive to progression rather than an initiating factor, in the pathogenesis of idiopathic scoliosis [3, 15, 20].
In the current study, we have seen that thoracic AIS curves exhibited a slightly more hypokyphotic lower thoracic T9–T12 segment compared with those of controls (5° vs 8°), in addition to a marked change in the proximal T5–T8 kyphosis (12° vs 8°). Thus, even if we consider the scoliosis patients to be globally slightly more hypokyphotic, not all of the segments of the thoracic spine are more hypokyphotic. This lower segment hypokyphosis in AIS, makes that segment more prone to rotational instability. Analyzing the different curve types, we find that different thoracic curve patterns describe different sagittal thoracic profiles.
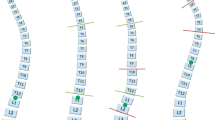
None of the studied sagittal parameters of the Lenke type 1 curves (single thoracic curves), differed significantly from those of the healthy adolescents (Fig. 1). This finding brings into question the influence of apical lordosis on the development of single thoracic curves.

Comparison between a healthy girl and a Lenke 1AN girl. Healthy patient: MT Cobb 7.8°; T5–T12: 20.2°, T5–T8: 16.5°, T9–T12: 3.3°. Lenke 1AN patient: MT Cobb: 53°, T5–T12: 21°, T5–T8: 18°, T9–T12: 2.7°
The Lenke type 2 curves (double thoracic curves) were slightly more hyperkyphotic (T5–T12 of 26°), and most of the kyphosis originated in the upper thoracic segments T5–T8 (20°), (Fig. 2). This finding can be seen during surgery, when the cranial segment of the thoracic spine falls into kyphosis, which makes it difficult to set the anchor points at the thoracic proximal levels. A way to correct this hyperkyphosis would be to use Ponte osteotomies along with convex rod compression. However, surgeons should be aware of this circumstance and develop a tendency to over-bend the rod in the upper thoracic segment to prevent proximal junctional kyphosis from excessive correction.

Comparison between a healthy girl and a Lenke 2AN girl. Healthy patient: MT Cobb 0.9°, T5–T12: 20.6°, T5–T8: 15.8°, T9–T12: 4.6°. Lenke 2AN patient: PT Cobb: 56°, MT Cobb: 60°, T5–T12: 26°, T5–T8: 25°, T9–T12: 1°
The most hypokyphotic curves were the Lenke type 3, double major curves, which exhibited a T5–T12 thoracic kyphosis of 19°. In the transition to the lumbar coronal curve (the change between curves), the lower thoracic segment acted in the sagittal plane as an abnormal upward continuation of the lumbar lordosis [1, 19, 23], and showed a T9–T12 kyphosis of nearly 1° (Fig. 3). To enable appropriate sagittal balance, the upper segment consequently developed hyperkyphosis and divided the thoracic kyphosis at the apical T8–T9 levels into a cranial hyperkyphosis and a caudal hypokyphosis. The most cranial vertebra of the hypokyphotic segment in the sagittal plane corresponded to the most rotated vertebra in the transversal plane, and to the apical vertebra in the frontal plane [19, 23], which continues 4–5 levels down into the lumbar spine [1, 3, 19]. Vertebral rotation is maximal at the cranial levels of this zone, and these vertebrae are located around the sagittal and coronal apices. This issue is important when selecting the corrective maneuver to use during surgery, because rod derotation or apical screw-derotation may increase this lordosis and flatten the spine. The use of all pedicle screw constructs has a significant hypokyphotic effect on thoracic sagittal plane alignment and if post-operative thoracic kyphosis is excessively decreased, the cervical spine may decompensate into significant kyphosis [6]. In such cases, medial translational maneuvers with extended screws, bands or wires following Asher’s principles of bringing the deformity into a concave rod molded with the desired kyphosis; the use of posterior Ponte osteotomies in distraction; different contouring of the concave (over contoured) and convex (under bended) rods to facilitate rotation; rigid rods; or anterior approaches can better restore thoracic kyphosis [4, 13, 35].

Comparison between a healthy girl and a Lenke 3CN girl. Healthy patient: MT Cobb: 0°, T5–T12: 17.3°, T5–T8: 17.4°, T9–12: 2.8°. Lenke 3CN patient MT Cobb: 54°, L Cobb: 53°, T5–T12: 18°, T5–T8: 15°, T9–T12: 1.5°
One limitation of our study is that lateral views were taken with standard lateral radiographic projections. The measurement of thoracic kyphosis with the Cobb method on lateral radiographs tends to underestimate the loss of thoracic kyphosis in patients with thoracic scoliotic curves due to the rotational component [10]. To perceive the true apical sagittal profile of thoracic scoliosis, the beam should be rotated by approximately 10° to eliminate the effect of vertebral rotation, or a 3D reconstruction tool should be used to obtain a “true lateral” view of the deformity [10, 12, 36]. However, the Cobb technique describes the lateral appearance of the patient well [26], and currently remains the most commonly available system. Another limitation is that matching between cohorts depended only on chronological age and gender. We cannot assure a perfect matching as other demographic variables such as (BMI, height, weight, or skeletal age) were not available. And finally, only patients with surgical magnitude curves were included in the analyses; it is unknown whether these sagittal parameters have the same characteristics and similar relations to those of healthy among subjects with small curve sizes.
In conclusion, AIS patients have a reduced thoracic kyphosis but very similar to that of healthy adolescents and within the range of normality. Global T5–T12 kyphosis is then within the normal values for this age. The apex acts as the inflexion point. Below the apex, there is a hypokyphosis extending 4–5 segments down to finally end up in the lumbar lordosis. Above the apex, there is a change into hyperkyphosis to finally obtain a global normokyphosis of the global thoracic spine. This has variations depending on the Lenke type. Patients with Lenke type 1 curves exhibited normal thoracic sagittal parameters, which bring into question the influence of lordosis on the development of single thoracic curves. Lenke type 3 curves exhibited lower thoracic segmental hypokyphosis, and type 2 curves exhibited upper segmental hyperkyphosis. These results should be considered when planning surgical strategies.
References
Dickson RA, Lawton JO, Archer IA, Butt WP (1984) The pathogenesis of idiopathic scoliosis. Biplanar spinal asymmetry. J Bone Joint Surg Br 66(1):8–15
Mac-Thiong J-M, Labelle H, Charlebois M, Huot M-P, de Guise JA (2003) Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine (Phila Pa 1976) 28(13):1404–1409
Upasani VV, Tis J, Bastrom T, Pawelek J, Marks M, Lonner B, Crawford A, Newton PO (2007) Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: how do these two curve types differ? Spine (Phila Pa 1976) 32(12):1355–1359
Sucato DJ, Agrawal S, O’Brien MF, Lowe TG, Richards SB, Lenke L (2008) Restoration of thoracic kyphosis after operative treatment of adolescent idiopathic scoliosis: a multicenter comparison of three surgical approaches. Spine (Phila Pa 1976) 33(24):2630–2636
Lonner BS, Lazar-Antman MA, Sponseller PD, Shah SA, Newton PO, Betz R, Shufflebarger HS (2012) Multivariate Analysis of Factors Associated With Kyphosis Maintenance in Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 37(15):1297–1302
Roussouly P, Labelle H, Rouissi J, Bodin A (2013) Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults. Eur Spine J 22(Suppl 2):S203–S215
Somerville EW (1952) Rotational lordosis: the development of the single curve. J Bone Joint Surg Br 34-B(3):421–427
Roaf R (1960) Vertebral growth and its mechanical control. J Bone Joint Surg Br 42-B(1):40–59
Dickson RA (1985) Aetiology of idiopathic spinal deformities. Arch Dis Child 60(6):508–511
Deacon P, Flood BM, Dickson RA (1984) Idiopathic scoliosis in three dimensions. A radiographic and morphometric analysis. J Bone Joint Surg Br 66(4):509–512
Guo X, Chau WW, Chan YL, Cheng JC (2003) Relative anterior spinal overgrowth in adolescent idiopathic scoliosis. Results of disproportionate endochondral membranous bone growth. J Bone Joint Surg Br 85(7):1026–1031
Hayashi K, Upasani VV, Pawelek JB, Aubin CE, Labelle H, Lenke LG, Jackson R, Newton PO (2009) Three-dimensional analysis of thoracic apical sagittal alignment in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 34(8):792–797
Cidambi KR, Glaser DA, Bastrom TP, Nunn TN, Ono T, Newton PO (2012) Postoperative Changes in Spinal Rod Contour in Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 37(18):1566–1572
Propst-Proctor SL, Bleck EE (1983) Radiographic determination of lordosis and kyphosis in normal and scoliotic children. J Pediatr Orthop 3(3):344–346
Rigo M, Quera-Salvá G, Villagrasa M (2006) Sagittal configuration of the spine in girls with idiopathic scoliosis: progressing rather than initiating factor. Stud Health Technol Inform 123:90–94
Ries Z, Harpole B, Graves C, Gnanapragasam G, Larson N, Weintstein S, Mendoza-Lattes SA (2015) Selective Thoracic Fusion of Lenke I and II Curves Affects Sagittal Profiles But Not Sagittal or Spinopelvic Alignment: A Case-Control Study. Spine (Phila Pa 1976) 40(12):926–934
Stokes IA, Sangole AP, Aubin CE (2009) Classification of scoliosis deformity three-dimensional spinal shape by cluster analysis. Spine (Phila Pa 1976) 34(6):584–590
Sangole AP, Aubin CE, Labelle H, Stokes IA, Lenke LG, Jackson R, Newton P (2009) Three-dimensional classification of thoracic scoliotic curves. Spine (Phila Pa 1976) 34(1):91–99
Charles YP, Bouchaïb J, Walter A, Schuller S, Sauleau EA, Steib J-P (2012) Sagittal balance correction of idiopathic scoliosis using the in situ contouring technique. Eur Spine J 21(10):1950–1956. doi:10.1007/s00586-012-2356-2
Grivas TB, Dangas S, Samelis P, Maziotou C, Kandris K (2002) Lateral spinal profile in school-screening referrals with and without late onset idiopathic scoliosis 10 degrees-2 degrees. Stud Health Technol Inform 91:25–31
Willner S (1981) Spinal pantograph. A non-invasive technique for describing kyphosis and lordosis in the thoracolumbar spine. Acta Orthop Scand 52:525–529
Schlösser TP, Vincken KL, Rogers K, Castelein RM, Shah SA (2015) Natural sagittal spino-pelvic alignment in boys and girls before, at and after the adolescent growth spurt. Eur Spine J 24(6):1158–1167. doi:10.1007/s00586-014-3536-z
Kotwicki T (2002) Sagittal and transversal plane deformity in thoracic scoliosis. Stud Health Technol Inform 91:251–256
Grivas TB, Dangas S, Polyzois BD, Samelis P (2002) The Double Rib Contour Sign (DRCS) in lateral spinal radiographs: aetiologic implications for scoliosis. Stud Health Technol Inform 88:38–43
Janssen MM, Drevelle X, Humbert L, Skalli W, Castelein RM (2009) Differences in male and female spino-pelvic alignment in asymptomatic young adults: a three-dimensional analysis using upright low-dose digital biplanar X-rays. Spine (Phila Pa 1976) 34(23):E826–E832. doi:10.1097/BRS.0b013e3181a9fd85
de Jonge T, Dubousset J, Illés T (2002) Sagittal plane correction in idiopathic scoliosis. Spine (Phila Pa 1976) 27(7):754–760
Vedantam R, Lenke LG, Keeney JA, Bridwell KH (1998) Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine (Phila Pa 1976) 23(2):211–215
Bernhardt M, Bridwell KH (1989) Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine (Phila Pa 1976) 14(7):717–721
Lee CS, Chung SS, Kang KC, Park SJ, Shin SK (2011) Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population. Spine (Phila Pa 1976) 36(25):E1648–E1654
Mac-Thiong JM, Labelle H, Berthonnaud E, Betz RR, Roussouly P (2007) Sagittal spinopelvic balance in normal children and adolescents. Eur Spine J 16(2):227–234
Lenke LG, Betz RR, Clements D, Merola A, Haher T, Lowe T, Newton P, Bridwell KH, Blanke K (2002) Curve prevalence of a new classification of operative adolescent idiopathic scoliosis: does classification correlate with treatment? Spine (Phila Pa 1976) 27(6):604–611
Archer IA, Dickson RA (1985) Stature and idiopathic scoliosis: a prospective study. J Bone Joint Surg Br 67(2):185–188
Janssen MM, Vincken KL, van Raak SM, Vrtovec T, Kemp B, Viergever MA, Bartels LW, Castelein RM (2013) Sagittal spinal profile and spinopelvic balance in parents of scoliotic children. Spine J 13(12):1789–1800
Dickson RA (1992) The etiology and pathogenesis of idiopathic scoliosis. Acta Orthop Belg 58(Suppl 1):21–25
Monazzam S, Newton PO, Bastrom TP, Yaszay B, Harms Study Group (2013) Multicenter comparison of the factors important in restoring thoracic kyphosis during posterior instrumentation for adolescent idiopathic scoliosis. Spine Deform 1(5):359–364. doi:10.1016/j.jspd.2013.06.002
du Peloux J, Fauchet R, Faucon B, Stagnara P (1965) The plan of choice for the radiologic examination of kyphoscolioses. Rev Chir Orthop Reparatrice Appar Mot 51(6):517–524
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript
Ethical standards
This study has IRB approval/Research Ethics Committee.
Rights and permissions
About this article

Cite this article
Pizones, J., Núñez-Medina, A., Sánchez-Mariscal, F. et al. Thoracic sagittal plane variations between patients with thoracic adolescent idiopathic scoliosis and healthy adolescents. Eur Spine J 25, 3095–3103 (2016). https://doi.org/10.1007/s00586-016-4400-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4400-0