
Abstract
Purpose
Several genomic loci have been previously found to be associated with intervertebral disc degeneration, so far. Data are mostly derived from northern European countries whereas data derived from Southern European Ancestor are limited. This study aimed to evaluate the association between radiological disease severity of lumbar disc degeneration and certain genetic loci in a sample of participants from Southern Europe.
Methods
Seventy-five patients with mild to severe lumbar disc degeneration and 25 healthy controls were enrolled into the study. In each subject, each lumbar intervertebral disc was separately examined to obtain a total radiological score for disease severity. In addition, single-nucleotide polymorphisms of predefined genetic samples were analyzed in all participants: COL1A1 Sp1, COL9a2 Trp2, COL9a3 Trp3, and VDR TaqI.
Results
Degeneration scores were significantly worse in cases with COL1A1 Sp1, COL9a3 Trp3, and VDR TaqI mutations; however, COL9a2 Trp2 mutation was not associated with a difference in the severity of disc degeneration. In addition, subjects with mutation in more than one gene sample (n = 20) had significantly worse degeneration scores than the remaining study participants (n = 80) (17.70 ± 2.72 vs. 21.81 ± 1.81, p < 0.001).
Conclusion
Single-nucleotide polymorphisms occurring in COL1A1, COL9a3 and VDR genes seem to be associated with the development of lumbar disc degeneration in this cohort, possibly with even more pronounced association when multiple mutations are present in the same individual. By further prospective twin studies in associated genes and analyses of their relationship with environmental factors in an internationally sampled large cohort will make a more clear-minded conclusion about their association with disc degeneration, which would yield better appreciation and clinical planning of some predisposed people for these pathologies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intervertebral disc degeneration and lumbar disc herniation are the two most common spinal conditions in adults. Low back pain represents the most important cause of work-related disability in people less than 45 years of age [1, 2].
Degeneration in intervertebral discs begins after the first decade of life [3]. In conjunction with degeneration, the equilibrium between the breakdown and buildup within the disc is disturbed, resulting in alteration in its biomechanical properties. Also influenced by biomechanical forces, a degenerated disc is more prone to herniation associated with severe low back and extremity pain. The most common concern related with disc degeneration was based on repetitive mechanical forces on intervertebral disc material, which was found to be less likely than genetic influences [4–7]. The association between intervertebral disc degeneration and genetic mutations has originally been proposed by Videman et al. [7] and Jones et al. [8] in 1998. The genomic structures that have been found to be associated with disc degeneration in subsequent studies include the vitamin D receptor (VDR), aggrecan gene, type I and type IX collagen mutations, and the matrix metalloproteinase enzyme gene [7, 9–13].
This study aimed to evaluate the association between disease severity and certain genetic mutations implicated in the occurrence of lumbar disc degeneration in a cohort from Turkey, Southern part of Europe. For this purpose, a gene analysis was performed in different subsets of the study population including subjects with symptoms of disc degeneration and healthy controls to assess the correlation between the genetic disorder and the severity of the radiological degeneration.
Materials and methods
Patients
Seventy-five patients with mild to severe lumbar disc degeneration and 25 healthy controls were included in this study. Exclusion criteria included current smoking, a profession requiring heavy physical work, history of spinal trauma, inflammatory or infectious disorders of spinal column, and congenital conditions. To rule out confounding factors related to gender or age differences, all patients were selected among male subjects between 35 and 45 years of age.
The study was conducted conjointly at Departments of Neurosurgery at Marmara University, and Marmara University Institute of Neurological Sciences. All patients provided written informed consent before participation in the study. The study protocol was approved by the Ethics Committee of the Medical Faculty of Marmara University (Approval code: MAR-YC-2008-0199).
Neuroradiological assessments
Magnetic resonance imaging (MRI) was performed in all participants for neuroradiological assessment. For this purpose, T2-weighted sagittal cross-sections were obtained to score intervertebral disc degeneration based on the classification system proposed by Pfirrmann et al. [14]. Pfirrmann’s classification differentiates intervertebral disc degeneration into 5 grades. While grade 1 corresponds to healthy intervertebral disc (homogenous bright white structure), grade 5 means advanced degeneration of intervertebral disc, accordingly. A point was given for every grade in a reverse manner (5 points to grade 1 intervertebral disc, 1 point to grade 5 intervertebral disc). Each lumbar intervertebral disc was separately scored from L1 to S1 to obtain a total score (max 25, min 5). Examples of scoring are given in Fig. 1. Kappa coefficients for intra- (0.84–0.90) and interobserver (0.69–0.81) reliability were reported high for Pfirrmann’s classification [14].

Three examples of lumbar intervertebral disc degeneration assessment for each intervertebral space using Pfirrmann’s classification [14]
Genetic analyses
For all study participants, the following single-nucleotide polymorphisms described previously for Collagen 1A1 (COL1A1), Collagen 9 alpha-2 (COL9a2), Collagen 9 alpha-3 (COL9a3), and Vitamin D receptor (VDR) genes were analyzed: COL1A1 Sp1, COL9a2 Trp2, COL9a3 Trp3, and VDR TaqI. DNA samples were extracted from venous blood samples (9 cc from each patient) in ethylenediamine tetraacetic acid (EDTA) tubes stored in cold chain. Refgen Biotechnology and Gene Research Institute (METU, Ankara, Turkey) performed all stages of the genetic analysis.
DNA isolation
After blood samples in EDTA tubes were transferred to another tube, 35 ml of double-purified ddH2O at +4 °C was added and stirred together for 5 min. Then, the samples were centrifuged at 2000 rpm for 10 min, and the supernatant was discarded from the tubes. A total of 25 ml of water at +4 °C was added into the precipitate, stirred for 5 min with a vortex, and centrifuged at 2000 rpm for 10 min again. Supernatant was discarded, and 3 ml of nucleolysis buffer, 200 microliter 10 % SDS, and 150 microliter proteinase K (10 mg/ml) were added and the mixture was dissolved with vortex stirring. After completion of this stage, the mixture was maintained at 37 °C for one night. Then, 2 ml of ammonium acetate (9, 6 M) was added. The mixture was kept at room temperature for 10 min, centrifuged at 3000 rpm for 20 min. On that occasion, the supernatant was transferred to another tube and absolute ethanol approximately two times the volume of the supernatant was added into it. The tube was slowly stirred to allow accumulation of genomic DNA. The DNA was transferred to a tube containing 1 ml of distilled water with the tip of a pipette. The purity and concentration of the resultant DNA samples were ascertained using a RNA/DNA meter (Pharmacia Biotech, New Jersey, USA).
Polymerase chain reaction
Polymerase chain reaction (PCR) was used to amplify the genomic DNA obtained through the abovementioned procedures. For this purpose, 50 μl of reaction volume was used that contained 100 ng of DNA, 1.25 units (U) Taq polymerase enzyme, 5 μl of 10X PZR buffer (the concentration in reaction is 1X), 5 μl of 2 mM dNTP, 25 pmol/μl of appropriate primers, and 1 mM of MgCl2. The 50 μl of reaction volume was obtained by the addition of ddH2O. DNA was allowed to accumulate, transferred to a tube containing 1 ml of distilled water using the tip of a pipette, and dissolved. The purity and concentration of the DNA samples obtained were ascertained using a RNA/DNA meter (Pharmacia Biotech, New Jersey, USA). In all five reactions that were allowed to occur within the context of the study procedures, an initial denaturation temperature of 95 °C for 5 min, and final temperature of 72 °C for 7 min were used.
Agarose gel electrophoresis and DNA sequence analysis
Agarose gel electrophoresis was used to observe the products of the PCR reactions. Agarose gel (1 %) was used for col1A1, Col9a2, Col9a3 and VDR regions. To obtain 1 % agarose gel, 0.25 g of agarose was weighed in a sensitive weighing scale and dissolved with the use of heat after addition of 25 ml of 0.5X TBE. After addition of ethidium bromide, the solution was poured into a gel tank. PCR products were loaded while being mixed with gel loading buffer. The products proceeded for 15–30 min depending on the length of the band at 100 V within the gel. DNA sequence analysis was performed on PCR products. The sequence analysis was performed in accordance with the method described in the instruction manual of the “Big Dye Terminator v3.1 Cycle Sequencing” kit (Applied Biosystems, Massachusetts, USA). Following the sequence PCR, a sequence cleansing was performed and the sequence was loaded into the device (ABI 3100 genetic analyzer, Applied Biosystems, Massachusetts, USA). The sequences read were compared with the reference sequences of the genome bank.
Statistical analyses
Statistical analyses were performed using SPSS Statistics for Windows, version 17.0. (Chicago: SPSS Inc, USA) statistics software package. Chi-square test was used to analyze significance level. The cut-off value for statistical significance was set at an alpha level of <0.05.
Results
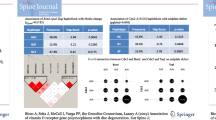
All participants were males at an age of between 35 and 45 years (mean age = 40.99 years). Overall Pfirrmann scores were between 10 and 25 (mean: 20.99 ± 2.59). The observed associations between radiological scores and genetic variations are as follows (Table 1).
There were 32 participants with heterozygote allele and 8 participants with homozygote allele of COL1A1 Sp1. There was a significant difference in Pfirrmann scores between neutral and heterozygous cases (21.88 ± 1.91 vs. 20.16 ± 2.81, p = 0.003). Significant difference was present between neutral and homozygous cases (21.88 ± 1.91 vs. 17.63 ± 2.62, p < 0.001). Hence, there was also statistically significant difference between heterozygous and homozygous cases for COL1A1 Sp1 mutations (20.16 ± 2.81 vs. 17.63 ± 2.62, p = 0.013).
A total number of three participants were found to harbor heterozygote allele of COL9a2 Trp2 gene locus. COL9a2 Trp2 polymorphism did not differ significantly in terms of Pfirrmann scores between neutral and heterozygous cases, even though scores were lower in the heterozygous group (21.12 ± 2.36 vs. 16.67 ± 6.11, p = 0.119). Of the three heterozygous participants, two had had previous lumbar spinal surgeries and recurrent diseases. No homozygous cases were detected for this mutation.
There were five participants with heterozygote allele of COL9a3 Trp3. Cases neutral for COL9a3 Trp3 had significantly higher Pfirrmann scores as compared to heterozygous cases (21.07 ± 2.63 vs. 19.40 ± 1.14, p = 0.044). All of the five heterozygous cases had had previous lumbar disc surgery with recurrence in three. No homozygous mutations were observed.
There were 39 and 11 participants with heterozygote and homozygote allele of VDR TaqI, respectively. A significant difference in Pfirrmann scores was found between those with neutral, heterozygous or homozygous VDR TaqI. Scores in neutral cases were significantly higher compared to both heterozygous cases (22.15 ± 1.83 vs. 20.61 ± 2.68, p = 0.004) and homozygous cases (22.15 ± 1.83 vs. 18.45 ± 2.51, p < 0.001). In addition, heterozygous cases had significantly higher scores than homozygous cases (20.61 ± 2.68 vs. 18.45 ± 2.51, p = 0.008).
Subjects with mutations in more than one gene location (n = 20) had significantly lower Pfirrmann scores than the remaining study participants (17.70 ± 2.72 vs. 21.81 ± 1.81, p < 0.001). Only one out of 25 healthy controls had multiple mutations (4 %). On the other hand, 19 out of 75 symptomatic patients had multiple mutations (25.3 %). The difference was significant (p = 0.021).
Discussion
Previous genetic studies on different populations have pointed out a propensity for intervertebral disc degeneration in individuals with SNP at certain genetic loci, which has also been the subject of the current study (Table 2) [7–11, 13, 15–48]. Genomic structures that have been associated with disc degeneration include the vitamin D receptor, aggrecan gene, type I and type IX collagen genes, and matrix metalloproteinase enzyme gene [7, 9–13]. A good knowledge of genetic factors associated with increased risk of disc degeneration bears some clinical significance, particularly in terms of predicting and preventing prevalent diseases such as lumbar disc herniation and low back pain.
In a recent and comprehensive review, approximately 20 gene locations have been detected that play a role in disc degeneration, those 20 locations were categorized into five functional groups: structural, catabolic, anticatabolic, inflammatory, other [49]. In this study, we analyzed 3 of the 20 gene locations, accordingly: Collagen I, collagen IX (a2 and a3 subtypes), and VDR.
Collagen I is the major building collagen unit of osseous tissues, annulus fibrosis, and the vertebral end-plates. In this regard, it is interesting to note that Grant et al. [50] described a polymorphism in the first intron of COL1A1 gene resulting as substitution of guanine (G) with thymidine (T) that is associated with decreased binding of a transcription factor referred to as Sp1. In that study, TT (homozygous) and GT (heterozygous) alleles have been found to represent a significant risk factor for osteoporosis. In recent years, COL1A1 Sp1 polymorphism has been frequently implicated in the development of osteoporosis and spinal degeneration [51]. The association between the genetic polymorphism of collagen I and disc degeneration was originally shown by Pluijm et al. [15]. On the other hand, Tilkeridis et al. [16] found an increased frequency of homozygote genotype in patients with lumbar disc disease. In the present study, the assessment of the association between COL1A1 Sp1 and intervertebral disc degeneration showed an increased predisposition to disc degeneration in subjects with mutations, which might be related to a change in the composition of collagen in the disc. Sp1 allele is resultant of an intronic polymorphism with potential adverse effects on transcription of collagen I.
Collagen IX, which is thought to play a bridging role between non-collagenous and collagenous tissues [10], is a heterotrimeric protein and contains three chains referred to as α1(IX), α2(IX), and α3(IX) that are separately coded by COL9a1, COL9a2 and COL9a3 genes, respectively [52, 53]. Collagen 9a2 is an SNP region that has been the subject of several studies in terms of its association with the risk of intervertebral disc degeneration [10, 11, 17–22]. For example, the sequence variations of the COL9a2 coding the α2 chain of collagen IX in the intervertebral disc have been studied in a Finnish population [10]. In that study, the rare Trp2 allele, which is located at codon 326 of COL9a2 and substitutes the natural amino acid arginine with tryptophan, was found to be present in 6 of 157 patients (allele frequency 1.9 %), while none of the healthy controls (n = 174) had this allele. Although this represents an important finding, the false negativity could not be ruled out since the study did not involve non-operated symptomatic patients. Our study is similar to that study in terms of the rare occurrence of Trp2 allele. In a study from China, 20 % of the study population has been found to have Trp2 allele, associated with a fourfold increased risk of annular rupture and 2.4-fold increased risk of disc degeneration [20]. In a Japanese study by Seki et al. [21], a specific haplotype COL9a2 has been found to be related with disc degeneration. Trp2 allele existed in 21.4 % of the patients undergoing lumbar discectomy. In a recent study, Zhu et al. examined collagen IX SNP mutations and used immunohistochemical methods to check the presence of collagen IX in the intervertebral disc space. These authors have proposed that collagen IX, which almost never exists in the normal adult disc, is produced in the context of a response to mechanical disc injury [54].
Trp3 polymorphism previously described in COL9a3 was present in five of the 100 cases in this study, who had also increased radiological severity scores compared to the remaining participants. In a Greek population, which may be considered to bear genetic similarities to Turkish population due to geographical neighborhood, Trp3 allele (COL9a3) was present in 8.6 % of those who underwent disc surgery, as compared to 4.9 % in healthy controls, with the difference being unable to reach statistical significance [26]. Solovieva et al. [24, 25] found a positive correlation between Trp3 allele and disc degeneration in 135 middle-aged men in their 2002 study, and proposed in another report published in 2006, that interleukin 1 beta gene polymorphism could modify this association. All of the patients with heterozygote allele of Trp3 in the presented study were bearing degenerated disc and had intervertebral disc disease-related problems. Three of the patients had already developed recurrent disc disease.
A study from India showed higher frequency of collagen 9a2 heterozygosity in those individuals with disc pathology, despite the absence of a similar association for collagen 9a3 [23] which is in contrast with our findings. This difference may be due to an unidentified genomic factor or another biological pathway, which was not addressed in our study; or this may be related geographical variance of the genomic material and influences of different environmental factors over genes.
Vitamin D receptor (VDR) is known to play a role in normal bone mineralization and bone remodeling. Genomic mutations of VDR have been associated with several conditions including osteoporosis, osteoarthritis, and degenerative disc disease [27, 55, 56]. A TaqI polymorphism on this gene has previously been described, and the resultant homozygous or heterozygous genotypes have been linked with degenerative intervertebral disc conditions [28]. In an Australian cohort study involving 172 female and 110 male patients, the frequency of VDR alleles was 63 % for “T” and 37 % for “t” [8], and the “tt” allele” was found to be significantly associated with osteophyte formation and radiologically documented disc degeneration. Radiologically lower signal intensity was present in 12.9 and 4.5 % of the subjects with TaqI “tt” and “Tt” genotypes, respectively, as compared to controls. Another retrospective study suggested a higher rate of annular rupture in those patients with the “tt” genotype [27]. In a Japanese population between 20 and 29 years of age, allele variations of the VDR gene have been found to be linked with severe disc degeneration at multiple levels [9]. In another study with providing more solid statistical evidence in terms of its larger sample size (804 participants), the odds ratio for disc degeneration was quite high, i.e., 2.61, for those subjects having the t allele of the VDR gene [28]. Further analyses in the same subjects showed even a more marked association for those less than 40 years of age (odds ratio 5.97). Similarly, in our study a significantly lower score for lumber disc degeneration was observed in those subjects carrying the VDR TaqI polymorphism.
Many genetic studies, which looked for possible gene loci that may be in association with disc degeneration, have been conducted in ancestors of Northern Europe or Far East Asia. There are two previous studies conducted in Greece, two in Italy and one in Turkey. Although these five studies have already looked for all these four gene loci, they did not analyze them all together. To our knowledge, this is the first study of looking for possible association of these four genes with disc degeneration in a southern Europe country, in separate and in combination [16, 26, 37, 40, 48]. One other important point to mention is that possible associations with disc degeneration have been depicted for collagen I and vitamin D receptor, but not for Collagen IX in those previous studies. Eser et al. [37] reported significant associations of VDR and aggrecan genes with intervertebral disc degeneration and disc herniation in a 300-participant Turkish cohort. They specifically studied both TaqI and FokI polymorphisms of VDR. Our study is concordant with their study in respect of TaqI polymorphism. Even though we did not look for any effect of aggrecan genes, we studied the role of collagen I and collagen IX in intervertebral disc degeneration. Not only the aggrecan and VDR genes, but also collagen 1A1 and collagen 9a3 were found to be significantly associated with disc degeneration. In further, this study also made us to realize a possible additive effect of multiple gene polymorphisms on disc degeneration grade and presence of multiple polymorphisms more commonly in diseased intervertebral discs (25.3 vs. 4 %). This might be through gene–gene interactions or simply breakdown of all structures in the intervertebral disc translated by representative gene loci (VDR, collagen I and IX). Further studies are in need to test this hypothesis.
All SNP studies of collagen I, collagen IX and vitamin D receptor in association with intervertebral disc degeneration are summarized in Table 2. Significant associations have been depicted for COL1A1, COL9a2, VDR, and less for COL9a3. Results are heterogenous across the studies and this can be due to differences in study designs, geographical areas and study participants (twins vs. non-twins).
One of the major limitations of our study is its sample size (i.e., 75 patients with lumbar disc degeneration and 25 controls), which is resultant of prospective nature of the study. Even though, the difference between neutral and heterozygote participants for COL9a2 was not significant, the heterozygote ones had lower Pfirrmann scores. The sample size could be the most relevant factor for this result. However, the number of participants in this study is considerably enough to make comparisons with literature and to give new insights for planning future studies. In addition, the scoring method used for assessing the severity of the disc degeneration may be criticized since Pfirrmann scoring system is not sensitive to the etiology of the disc degeneration and is qualitative in nature. Alternative scoring methods share the same disadvantage of not being sensitive to etiological factors. Despite its qualitative assessment nature, it has been shown that intra- and inter-reliability of Pfirrmann classification is high [14].
Twin studies are the most appropriate model for evaluation of genetic and environmental effects on disc degeneration. It has been demonstrated that environmental factors including smoking have tiny statistically significant effect on disc degeneration process. The most striking fact was not only the degeneration itself but also degenerative events were similar in twin brothers. However, the twin studies were limited to Northern Europe and Northern America [4, 57]. Such a twin study generalized to more other populations will enhance the knowledge about the relation of gene–gene, gene–environment in respect of intervertebral disc degeneration.
Conclusions
Our results suggest that single-nucleotide polymorphisms occurring in COL1A1, COL9a3 and VDR genes seem to be associated with the development of lumbar disc degeneration, with even more pronounced association when multiple mutations in same individuals are present. By further prospective twin studies in associated genes and analyses of their relationship with environmental factors in an internationally sampled large cohort will make a more clear-minded conclusion about their association with disc degeneration, which would yield better appreciation and clinical planning of some predisposed people for these pathologies.
Abbreviations
- SNP:
-
Single-nucleotide polymorphism
- M:
-
Male
- F:
-
Female
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
References
Kelsey JL (1978) Epidemiology of radiculopathies. Adv Neurol 19:385–398
McCowin PR, Borenstein D, Wiesel SW (1991) The current approach to the medical diagnosis of low back pain. Orthop Clin N Am 22:315–325
Buckwalter JA (1995) Aging and degeneration of the human intervertebral disc. Spine (Phila Pa 1976) 20:1307–1314
Battie MC, Videman T, Kaprio J, Gibbons LE, Gill K, Manninen H, Saarela J, Peltonen L (2009) The Twin Spine Study: contributions to a changing view of disc degeneration. Spine J 9:47–59. doi:10.1016/j.spinee.2008.11.011
Battie MC, Videman T, Gibbons LE, Fisher LD, Manninen H, Gill K (1995) 1995 volvo award in clinical sciences. Determinants of lumbar disc degeneration. A study relating lifetime exposures and magnetic resonance imaging findings in identical twins. Spine (Phila Pa 1976) 20:2601–2612
Sambrook PN, MacGregor AJ, Spector TD (1999) Genetic influences on cervical and lumbar disc degeneration: a magnetic resonance imaging study in twins. Arthritis Rheum 42:366–372. doi:10.1002/1529-0131(199902)42:2<366:AID-ANR20>3.0.CO;2-6
Videman T, Leppavuori J, Kaprio J, Battie MC, Gibbons LE, Peltonen L, Koskenvuo M (1998) Intragenic polymorphisms of the vitamin D receptor gene associated with intervertebral disc degeneration. Spine (Phila Pa 1976) 23:2477–2485
Jones G, White C, Sambrook P, Eisman J (1998) Allelic variation in the vitamin D receptor, lifestyle factors and lumbar spinal degenerative disease. Ann Rheum Dis 57:94–99
Kawaguchi Y, Kanamori M, Ishihara H, Ohmori K, Matsui H, Kimura T (2002) The association of lumbar disc disease with vitamin-D receptor gene polymorphism. J Bone Joint Surg Am 84-A:2022–2028
Annunen S, Paassilta P, Lohiniva J, Perala M, Pihlajamaa T, Karppinen J, Tervonen O, Kroger H, Lahde S, Vanharanta H, Ryhanen L, Goring HH, Ott J, Prockop DJ, Ala-Kokko L (1999) An allele of COL9A2 associated with intervertebral disc disease. Science 285:409–412
Paassilta P, Lohiniva J, Goring HH, Perala M, Raina SS, Karppinen J, Hakala M, Palm T, Kroger H, Kaitila I, Vanharanta H, Ott J, Ala-Kokko L (2001) Identification of a novel common genetic risk factor for lumbar disk disease. Jama 285:1843–1849
Takahashi M, Haro H, Wakabayashi Y, Kawa-uchi T, Komori H, Shinomiya K (2001) The association of degeneration of the intervertebral disc with 5a/6a polymorphism in the promoter of the human matrix metalloproteinase-3 gene. J Bone Joint Surg Br 83:491–495
Valdes AM, Hassett G, Hart DJ, Spector TD (2005) Radiographic progression of lumbar spine disc degeneration is influenced by variation at inflammatory genes: a candidate SNP association study in the Chingford cohort. Spine (Phila Pa 1976) 30:2445–2451
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N (2001) Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 26:1873–1878
Pluijm SM, van Essen HW, Bravenboer N, Uitterlinden AG, Smit JH, Pols HA, Lips P (2004) Collagen type I alpha1 Sp1 polymorphism, osteoporosis, and intervertebral disc degeneration in older men and women. Ann Rheum Dis 63:71–77
Tilkeridis C, Bei T, Garantziotis S, Stratakis CA (2005) Association of a COL1A1 polymorphism with lumbar disc disease in young military recruits. J Med Genet 42:e44. doi:10.1136/jmg.2005.033225
Wrocklage C, Wassmann H, Paulus W (2000) COL9A2 allelotypes in intervertebral disc disease. Biochem Biophys Res Commun 279:398–400. doi:10.1006/bbrc.2000.3967
Karppinen J, Paakko E, Raina S, Tervonen O, Kurunlahti M, Nieminen P, Ala-Kokko L, Malmivaara A, Vanharanta H (2002) Magnetic resonance imaging findings in relation to the COL9A2 tryptophan allele among patients with sciatica. Spine (Phila Pa 1976) 27:78–83
Noponen-Hietala N, Kyllonen E, Mannikko M, Ilkko E, Karppinen J, Ott J, Ala-Kokko L (2003) Sequence variations in the collagen IX and XI genes are associated with degenerative lumbar spinal stenosis. Ann Rheum Dis 62:1208–1214
Jim JJ, Noponen-Hietala N, Cheung KM, Ott J, Karppinen J, Sahraravand A, Luk KD, Yip SP, Sham PC, Song YQ, Leong JC, Cheah KS, Ala-Kokko L, Chan D (2005) The TRP2 allele of COL9A2 is an age-dependent risk factor for the development and severity of intervertebral disc degeneration. Spine (Phila Pa 1976) 30:2735–2742
Seki S, Kawaguchi Y, Mori M, Mio F, Chiba K, Mikami Y, Tsunoda T, Kubo T, Toyama Y, Kimura T, Ikegawa S (2006) Association study of COL9A2 with lumbar disc disease in the Japanese population. J Hum Genet 51:1063–1067. doi:10.1007/s10038-006-0062-9
Higashino K, Matsui Y, Yagi S, Takata Y, Goto T, Sakai T, Katoh S, Yasui N (2007) The alpha2 type IX collagen tryptophan polymorphism is associated with the severity of disc degeneration in younger patients with herniated nucleus pulposus of the lumbar spine. Int Orthop 31:107–111. doi:10.1007/s00264-006-0117-8
Rathod TN, Chandanwale AS, Gujrathi S, Patil V, Chavan SA, Shah MN (2012) Association between single nucleotide polymorphism in collagen IX and intervertebral disc disease in the Indian population. Indian J Orthop 46:420–426. doi:10.4103/0019-5413.97261
Solovieva S, Lohiniva J, Leino-Arjas P, Raininko R, Luoma K, Ala-Kokko L, Riihimaki H (2002) COL9A3 gene polymorphism and obesity in intervertebral disc degeneration of the lumbar spine: evidence of gene-environment interaction. Spine (Phila Pa 1976) 27:2691–2696. doi:10.1097/01.BRS.0000035266.44292.FA
Solovieva S, Lohiniva J, Leino-Arjas P, Raininko R, Luoma K, Ala-Kokko L, Riihimaki H (2006) Intervertebral disc degeneration in relation to the COL9A3 and the IL-1ss gene polymorphisms. Eur Spine J 15:613–619. doi:10.1007/s00586-005-0988-1
Kales SN, Linos A, Chatzis C, Sai Y, Halla M, Nasioulas G, Christiani DC (2004) The role of collagen IX tryptophan polymorphisms in symptomatic intervertebral disc disease in Southern European patients. Spine (Phila Pa 1976) 29:1266–1270
Videman T, Gibbons LE, Battie MC, Maravilla K, Vanninen E, Leppavuori J, Kaprio J, Peltonen L (2001) The relative roles of intragenic polymorphisms of the vitamin d receptor gene in lumbar spine degeneration and bone density. Spine (Phila Pa 1976) 26:E7–E12
Cheung KM, Chan D, Karppinen J, Chen Y, Jim JJ, Yip SP, Ott J, Wong KK, Sham P, Luk KD, Cheah KS, Leong JC, Song YQ (2006) Association of the Taq I allele in vitamin D receptor with degenerative disc disease and disc bulge in a Chinese population. Spine (Phila Pa 1976) 31:1143–1148. doi:10.1097/01.brs.0000216530.41838.d3
Videman T, Saarela J, Kaprio J, Nakki A, Levalahti E, Gill K, Peltonen L, Battie MC (2009) Associations of 25 structural, degradative, and inflammatory candidate genes with lumbar disc desiccation, bulging, and height narrowing. Arthritis Rheum 60:470–481. doi:10.1002/art.24268
Kelempisioti A, Eskola PJ, Okuloff A, Karjalainen U, Takatalo J, Daavittila I, Niinimaki J, Sequeiros RB, Tervonen O, Solovieva S, Kao PY, Song YQ, Cheung KM, Chan D, Ala-Kokko L, Jarvelin MR, Karppinen J, Mannikko M (2011) Genetic susceptibility of intervertebral disc degeneration among young Finnish adults. BMC Med Genet 12:153. doi:10.1186/1471-2350-12-153
Eskola PJ, Kjaer P, Daavittila IM, Solovieva S, Okuloff A, Sorensen JS, Wedderkopp N, Ala-Kokko L, Mannikko M, Karppinen JI (2010) Genetic risk factors of disc degeneration among 12-14-year-old Danish children: a population study. Int J Mol Epidemiol Genet 1:158–165
Oishi Y, Shimizu K, Katoh T, Nakao H, Yamaura M, Furuko T, Narusawa K, Nakamura T (2003) Lack of association between lumbar disc degeneration and osteophyte formation in elderly japanese women with back pain. Bone 32:405–411
Sakai Y, Matsuyama Y, Hasegawa Y, Yoshihara H, Nakamura H, Katayama Y, Imagama S, Ito Z, Ishiguro N, Hamajima N (2007) Association of gene polymorphisms with intervertebral disc degeneration and vertebral osteophyte formation. Spine (Phila Pa 1976) 32:1279–1286. doi:10.1097/BRS.0b013e318059af8a
Virtanen IM, Karppinen J, Taimela S, Ott J, Barral S, Kaikkonen K, Heikkila O, Mutanen P, Noponen N, Mannikko M, Tervonen O, Natri A, Ala-Kokko L (2007) Occupational and genetic risk factors associated with intervertebral disc disease. Spine (Phila Pa 1976) 32:1129–1134. doi:10.1097/01.brs.0000261473.03274.5c
Nunes FTB, Conforti-Froes NDT, Negrelli WF, Souza DRS (2007) Genetic and environmental factors involved on intervertebral disc degeneration. Acta Ortop Bras 15:09–13
Yuan HY, Tang Y, Lei L, Xiao GB, Liang YX, Wang S, Xia ZL (2010) Synergistic interaction between MMP-3, VDR gene polymorphisms and occupational risk factors on lumbar disc degeneration. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 28:334–338
Eser B, Cora T, Eser O, Kalkan E, Haktanir A, Erdogan MO, Solak M (2010) Association of the polymorphisms of vitamin D receptor and aggrecan genes with degenerative disc disease. Genet Test Mol Biomarkers 14:313–317. doi:10.1089/gtmb.2009.0202
Omair A, Lie BA, Reikeras O, Brox JI (2012) An association study of interleukin 18 receptor genes (IL18R1 and IL18RAP) in lumbar disc degeneration. Open Orthop J 6:164–171. doi:10.2174/1874325001206010164
Cervin Serrano S, Gonzalez Villareal D, Aguilar-Medina M, Romero-Navarro JG, Romero Quintana JG, Arambula Meraz E, Osuna Ramirez I, Picos-Cardenas V, Granados J, Estrada-Garcia I, Sanchez-Schmitz G, Ramos-Payan R (2014) Genetic polymorphisms of interleukin-1 alpha and the vitamin d receptor in mexican mestizo patients with intervertebral disc degeneration. Int J Genom 2014:302568. doi:10.1155/2014/302568
Colombini A, Brayda-Bruno M, Lombardi G, Croiset SJ, Vrech V, Maione V, Banfi G, Cauci S (2014) FokI polymorphism in the vitamin D receptor gene (VDR) and its association with lumbar spine pathologies in the italian population: a case-control study. Plos One 9:e97027. doi:10.1371/journal.pone.0097027
Vieira LA, De Marchi PL, dos Santos AA, Christofolini DM, Barbosa CP, Fonseca FL, Bianco B, Rodrigues LM (2014) Analysis of FokI polymorphism of vitamin D receptor gene in intervertebral disc degeneration. Genet Test Mol Biomarkers 18:625–629. doi:10.1089/gtmb.2014.0030
Zawilla NH, Darweesh H, Mansour N, Helal S, Taha FM, Awadallah M, El Shazly R (2014) Matrix metalloproteinase-3, vitamin D receptor gene polymorphisms, and occupational risk factors in lumbar disc degeneration. J Occup Rehabil 24:370–381. doi:10.1007/s10926-013-9472-7
Chen W, Li G, Sun H, Ye W, Huang D, Su P, Zhang Z (2012) Association of vitamin D receptor gene polymorphism in Han people with lumbar degenerative disc disease. Afr J Pharm Pharmacol 6:1211–1215
Jordan KM, Syddall H, Dennison EM, Cooper C, Arden NK (2005) Birthweight, vitamin D receptor gene polymorphism, and risk of lumbar spine osteoarthritis. J Rheumatol 32:678–683
Karppinen J, Paakko E, Paassilta P, Lohiniva J, Kurunlahti M, Tervonen O, Nieminen P, Goring HH, Malmivaara A, Vanharanta H, Ala-Kokko L (2003) Radiologic phenotypes in lumbar MR imaging for a gene defect in the COL9A3 gene of type IX collagen. Radiology 227:143–148. doi:10.1148/radiol.2271011821
Matsui Y, Mirza SK, Wu JJ, Carter B, Bellabarba C, Shaffrey CI, Chapman JR, Eyre DR (2004) The association of lumbar spondylolisthesis with collagen IX tryptophan alleles. J Bone Joint Surg Br 86:1021–1026
Koshizuka Y, Ogata N, Shiraki M, Hosoi T, Seichi A, Takeshita K, Nakamura K, Kawaguchi H (2006) Distinct association of gene polymorphisms of estrogen receptor and vitamin D receptor with lumbar spondylosis in post-menopausal women. Eur Spine J 15:1521–1528. doi:10.1007/s00586-005-0005-8
Colombini A, Brayda-Bruno M, Ferino L, Lombardi G, Maione V, Banfi G, Cauci S (2015) Gender differences in the VDR-FokI polymorphism and conventional non-genetic risk factors in association with lumbar spine pathologies in an Italian case-control study. Int J Mol Sci 16:3722–3739. doi:10.3390/ijms16023722
Mayer JE, Iatridis JC, Chan D, Qureshi SA, Gottesman O, Hecht AC (2013) Genetic polymorphisms associated with intervertebral disc degeneration. Spine J 13:299–317. doi:10.1016/j.spinee.2013.01.041
Grant SF, Reid DM, Blake G, Herd R, Fogelman I, Ralston SH (1996) Reduced bone density and osteoporosis associated with a polymorphic Sp1 binding site in the collagen type I alpha 1 gene. Nat Genet 14:203–205. doi:10.1038/ng1096-203
Williams FM, Spector TD (2007) The genetics of osteoporosis. Acta Reumatol Port 32:231–240
Paassilta P, Pihlajamaa T, Annunen S, Brewton RG, Wood BM, Johnson CC, Liu J, Gong Y, Warman ML, Prockop DJ, Mayne R, Ala-Kokko L (1999) Complete sequence of the 23-kilobase human COL9A3 gene. Detection of Gly-X-Y triplet deletions that represent neutral variants. J Biol Chem 274:22469–22475
Pihlajamaa T, Vuoristo MM, Annunen S, Perala M, Prockop DJ, Ala-Kokko L (1998) Human COL9A1 and COL9A2 genes. Two genes of 90 and 15 kb code for similar polypeptides of the same collagen molecule. Matrix Biol 17:237–241
Zhu Y, Wu JJ, Weis MA, Mirza SK, Eyre DR (2011) Type IX collagen neo-deposition in degenerative discs of surgical patients whether genotyped plus or minus for COL9 risk alleles. Spine (Phila Pa 1976) 36:2031–2038. doi:10.1097/BRS.0b013e3181ffdd61
Christakos S, Barletta F, Huening M, Dhawan P, Liu Y, Porta A, Peng X (2003) Vitamin D target proteins: function and regulation. J Cell Biochem 88:238–244. doi:10.1002/jcb.10349
Morrison NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV, Sambrook PN, Eisman JA (1994) Prediction of bone density from vitamin D receptor alleles. Nature 367:284–287. doi:10.1038/367284a0
Battie MC, Haynor DR, Fisher LD, Gill K, Gibbons LE, Videman T (1995) Similarities in degenerative findings on magnetic resonance images of the lumbar spines of identical twins. J Bone Jt Surg Am 77:1662–1670
Acknowledgments
Murat Şakir Ekşi, M.D. was supported by a grant from Tubitak, The Scientific and Technological Research Council of Turkey (Grant Number: 1059B191400255).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Toktaş, Z.O., Ekşi, M.Ş., Yılmaz, B. et al. Association of collagen I, IX and vitamin D receptor gene polymorphisms with radiological severity of intervertebral disc degeneration in Southern European Ancestor. Eur Spine J 24, 2432–2441 (2015). https://doi.org/10.1007/s00586-015-4206-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4206-5