
Abstract
Degenerative changes have the potential to greatly disrupt the normal curvature of the spine, leading to sagittal malalignment. This phenomenon is often treated with operative modalities, such as osteotomies, though even with surgery, only one-third of patients may reach neutral alignment. Improvement in surgical outcomes may be achieved through better understanding of radiographic spino-pelvic parameters and their association with deformity. Methodical surgical planning, including selection of levels of instrumentation and site of the osteotomy, is crucial in determining the optimal plan for a patient’s specific pathology and may minimize risk of developing postoperative proximal junctional kyphosis/failure. While sagittal alignment is essential in operative strategy, the coronal plane should not be overlooked, as it may affect the osteotomy technique. The concepts of sagittal balance and alignment are further complicated in patients with neuromuscular diseases such as Parkinson’s disease, and appreciation of the interplay between anatomic and postural deformities is necessary to properly treat these patients. Finally, given the importance of sagittal alignment and the role of osteotomies in treatment for deformity, the need for future research becomes apparent. Novel intraoperative measurement techniques and three-dimensional analysis of the spine may allow for vastly improved operative correction. Furthermore, awareness of the relationship between alignment and balance, the soft tissue envelope, and compensatory mechanisms will provide a more comprehensive conception of the nature of spinal deformity and the modalities with which it is treated.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Many healthy individuals are fortunate enough to either age without developing significant degenerative changes [1] or developing ankylosis of the spine. If no other pathologies are involved, these subjects age in a favorable pathway, maintaining an acceptable sagittal alignment and remaining asymptomatic. However, the combination of aging and a cascade of degenerative events lead to an unfavorable and irreversible scenario. The degenerative process primarily affects the lumbar spine and involves intervertebral discs, facet joints, ligaments and bone. The lumbar curve and spinal alignment is an anatomical feature unique to the hominidae species and allows maintenance of neutral upright posture with minimum energy expenditure. However, when degenerative changes affect the lordotic component of the normal spinal curvatures, the harmony of the sagittal plane is disrupted, leading to the well-described phenomenon of sagittal malalignment.
While malalignment itself is not an indication for surgery, the subsequent pain and decline in functional status constitute a concerning clinical picture. The previously described loss of lumbar lordosis (LL) leads to anterior (positive) sagittal alignment. As a response, the body progressively recruits compensatory mechanisms to counteract the anterior truncal shift. A chain of compensation is initiated from the flexible parts of the spine, and extends to the hips, lower extremities, and cervical spine to preserve an erect posture and horizontal gaze [2, 3]. The interaction between deformity and compensatory mechanisms depicts the final presentation of patients with adult spinal deformity (ASD).
Several studies have described the debilitating course of sagittal deformity, which requires enormous energy expenditure and severely impairs quality of life [4–7]. Patients usually seek treatment because of pain and disability, which are the main characteristics of the ASD clinical presentation [5]. While non-operative treatment in ASD can do little to impact pathological anatomy or curve progression [6], it may have benefit in a specific subset of patients with mild or moderate disease [7]. However, in cases of severe deformity, non-operative treatment modalities may not suffice [8]. For complex sagittal deformities, surgical intervention has been shown to offer superior clinical and radiographic outcomes compared to non-operative approaches [9, 10]. Careful consideration of the risks, complications, and all possible outcomes of surgery must occur when patients consider transitioning from non-operative to operative care. Recent studies on outcomes following ASD surgeries have shown high rates of complications (8.4–42 %) [11, 12] and revisions (9–17.6 %) [13, 14]. On the other hand, as improvements in the medical area continue to advance, patients’ expectations for surgery have reached unprecedented levels, even including full recovery to daily activities [15, 16].
Why do we fail?
Adequate alignment following surgical treatment is not consistently achieved. Recent studies revealed that only 32 % of patients reach neutral alignment, while 42 % remain with some positive sagittal malalignment; 26 % are overcorrected [17]. In addition, the rate of revision surgery following realignment procedures has been shown to increase progressively with longer follow-up: 12.3 % for 3-month follow-up and 17.6 % for 1-year follow-up. Given that revision rates may approach 30 % in some cases [18], it is possible that these revisions are driven by failure to achieve and/or maintain realignment.
Multi-center and inter-site variability studies revealed wide variability in reported complication and revision rates among different sites in the same study group, and even among different surgeons at the same institution [18, 19]. These studies unmasked manageable failures and demonstrated opportunities for improvement. This review will specifically address several of these matters: understanding of the sagittal plane, surgical planning, common complications such as proximal junctional failure, and the often overlooked topics of coronal plane and balance.
Opportunity 1: sagittal plane understanding
The importance of the pelvis
The pelvis is a key factor in conceptualizing the ideal spinal alignment in the sagittal plane. To realign the spine, it is crucial to identify the magnitude of the sagittal deformity, as well as the pelvic compensation that can mislead the surgeon in the assessment of postural alignment. Spinal sagittal malalignment (SSD) represents not only the deviation of lumbar lordosis from the ideal curve, but also the discordance of the lumbar curve from its seat, the pelvis.
Over the past few decades, numerous authors’ contributions to the literature have alerted the scientific community to the importance of the pelvis in SSD [4, 20–22]. This research led to four important facts:
-
1.
The pelvis is another caudal spinal vertebra.
-
2.
The pelvic morphology can be assessed using the pelvic incidence angle (PI, Fig. 1).
Fig. 1 
Pelvic incidence
-
3.
The pelvic retro version masks the true spinal alignment (Fig. 2), and should be measured using the pelvic tilt angle (PT).
Fig. 2 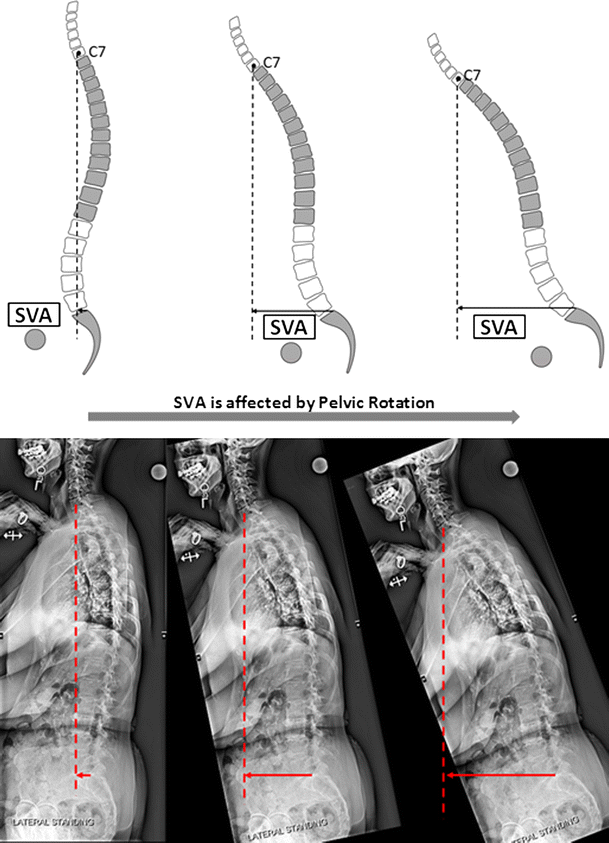
Impact of pelvic rotation (left to right, decrease in pelvic tilt) on global alignment
-
4.
The mismatch between lumbar lordosis and pelvic morphology angles allows for the quantification of sagittal deformity (Fig. 3).
Fig. 3 
Pelvic incidence minus lumbar lordosis (PI-LL) mismatch



What to correct?
Full analysis of the pelvis is highly recommended. This is accomplished by quantifying the pelvic morphological parameters and the sagittal orientation of the sacral plate (sacral slope, “SS”), which governs the lumbar curve. From studies of asymptomatic subjects, we know that individuals with a small pelvic incidence (PI) tend to have a vertical sacrum and relatively small and short lumbar lordosis. Conversely, individuals with large PI tend to have a horizontal sacrum and a relatively large and long lumbar lordosis [21, 23]. Schwab et al. simplified this complex spino-pelvic relationship with the concept of “Pelvic Incidence minus Lumbar Lordosis”. PI-LL is the difference between the PI angle and the lumbar lordosis (LL) angle, and quantifies the mismatch between pelvic morphology and the lumbar curve. The authors suggested that the ideal PI-LL target should be ≤10° if satisfactory spino-pelvic alignment is to be achieved [4].
As previously mentioned, the PI-LL relationship is valuable when planning deformity surgical correction in the sagittal plane. It allows a surgeon to estimate the required amount of LL to match PI, thus answering the question of what and how much to correct. A more recent study on surgical patients confirmed that use of the PI-LL relationship to determine the amount of correction when planning the operation is an excellent predictor of postoperative standing alignment. Moreover, in this study, adherence to a stricter threshold of lumbo-pelvic mismatch (correction aimed for PI-LL ≤ 0°) was an even stronger predictor of good sagittal alignment [24]. Of note, the authors found that patients with thoracic hyperkyphosis or significant kyphosis in the thoracolumbar junction required greater lordotic correction (PI-LL < −10°) [24].
Limitations
Studies on “PI-LL” demonstrated the validity and reliability of this formula in a wide range of realignment challenges [4, 25, 26]. However, this simple approach has limitations when applied to individuals with extreme values of PI and/or severe thoracic kyphosis (TK). The same team investigated these limitations in recent communications and proposed the following solutions [27]:
-
1.
Low PI patients require LL in excess of PI (LL = PI + 10°), while large PI patients require LL smaller than their PI (LL = PI − 10°).
-
2.
High TK patients also require LL greater than the theoretical LL to compensate for the thoracic hyperkyphosis.
-
3.
These two findings are summarized by the formula LL = (PI + TK)/2 + 10. This formula was developed using multi-linear regression analysis and validated on a separate group of subjects.
In summary, the correction should target the driver of the deformity. Loss of lumbar lordosis is the driver of the vast majority of sagittal deformities. Therefore, the PI-LL parameter provides an easy, pragmatic, and established solution. The site of deformity and correction is also a crucial step in SSD operative planning. On average, 65 % of the LL occurs in the extreme caudal lumbar segments [28], and perhaps unsurprisingly, the degenerative changes that lead to loss of LL also occur in the caudal lumbar spine [29]. Of course, the individual history, circumstances, and goals of each patient should be considered along with quantitative targets in surgical decision-making. Thus, the determination of where in the lumbar curve should the correction take a place is multifactorial and depends upon individual curve characteristics, existing fusion masses or pseudarthrosis, and surgical team preference [30, 31].
Correction of LL to match the pelvic morphology indirectly impacts the anterior truncal inclination, as assessed by the sagittal vertical axis (SVA), and the pelvic compensation, assessed by PT. Along with PI-LL, correction of these modifiers through surgery can greatly improve the clinical outcomes measured by health-related quality of life (HRQOL) scores. A 2013 study by Smith et al. [32] compared patients who improved in the sagittal modifiers (PT, SVA, or PI-LL) versus those whose sagittal modifiers deteriorated in. Patients who improved in spino-pelvic modifiers after surgical correction were more likely to reach a clinically noticeable difference in HRQOL [such as oswestry disability index (ODI), general health questionnaire (SF-36), scoliosis research society (SRS) activity and pain scores] than those whose modifiers deteriorated or remained the same.
There is no clear consensus in the literature regarding the ideal PT. Some authors are proponents of a fixed threshold of 20°. Others, such as Vialle et al. [33] derived patient-specific pelvic tilt values from the pelvic morphology, using the equation PT = 0.37 × PI − 7. From multiple studies of asymptomatic individuals, we have learned that PI values range from 30° to 90° [34–36]. Using Vialle’s equation, the ideal PT values for PI 30° and PI 90° are 4.1° and 26°, respectively. Therefore, even for the extreme values of PI, PT of 20° is a reasonable simplified threshold, and more clinically feasible than the alternative of memorizing and calculating equations.
Opportunity 2: surgical planning beyond sagittal alignment
In addition to the surgical planning pertaining to sagittal spino-pelvic alignment, numerous aspects of the surgery need to be carefully planned.
Upper- and lower-instrumented vertebra (UIV, LIV)
The choice of the UIV is crucial and is based on several principles to avoid mechanical complications due to biomechanical overload or reciprocal changes of the unfused segment after correction-stabilization surgery [37–41]:
Avoidance of the apex of kyphosis
The instrumentation must end at a sagittally neutral vertebra in terms of alignment [42]. This rule is simple to apply regarding the LIV. However, it should be acknowledged that determination of a stable sagittal vertebra may be difficult in cases of extreme deformity. In ASD patients with positive sagittal alignment, commonly accepted levels for the UIV are T2-3, T10, or L2 [43]. As a generally accepted rule, fusion should not stop at the apex of a regional or focal kyphosis to avoid proximal junctional failure [38]. When compensatory hypokyphosis of the thoracic spine is present, the surgeon should avoid an UIV between T5 and T9, as postoperatively, this region will become the apex of the thoracic kyphosis.
Quality of adjacent discs
Assessment of the cephalad intervertebral mobile segment is crucial in the choice of UIV. Signs of degenerative disc disease and/or stenosis alert to a segment that would serve as a poor site for instrumentation termination [41, 44]. Magnetic resonance imaging (MRI) is useful in the evaluation of stenosis as well as the quality and the hydration of the disc and the zygapophyseal joints of the segments adjacent to the planned fusion.
Avoidance of the thoracolumbar transition zone
The thoracolumbar junction (TLJ) is a transition zone between the relatively rigid “barrel” of the thoracic spine and the more mobile lumbar region. Most authors prefer to instrument across the TLJ, placing the UIV either below it (frequently L2) or above it (frequently T10). However, there is no definitive evidence to support this algorithm. Stopping at T10 can be a viable option in the setting of limited realignment procedures, especially when the thoracic spine compensates for imbalance with active extension [45].
Avoidance of the upper lumbar spine (L1, L2) as UIV
Ending the construct at the upper lumbar spine in severe sagittal deformity provides poor clinical results and high risk of proximal junctional kyphosis (PJK). Moreover, it limits the amount of possible correction and has been reported to be associated to a suboptimal rate of fusion [41, 46]. Kim et al. [46] observed that 73 % of patients with lumbar UIVs had suboptimal sagittal alignment postoperatively, compared to only 29 % of patients with T9–T10 UIVs; this difference was attributed to greater kyphosis of vertebral segments over the UIV when a lumbar site was chosen.
Choice of lower-instrumented vertebra (LIV)
The choice of LIV is still debated in the literature. While some surgeons preferred to fuse to L5 to avoid extensive dissection and risk of pseudarthrosis [47], studies by Edwards et al. [48] and Kuhns et al. [49] demonstrated a high risk of adjacent segment disease (61 and 68 %, respectively) if the construct stops at L5, versus a 25 % revision rate associated with extension to S1. In 2004, Bridwell [44] proposed criteria necessitating fusion to S1: L5–S1 spondylolisthesis; previous L5–S1 laminectomy; central or foraminal stenosis at L5–S1; oblique coronal take-off of L5 (>15°), and severe degenerative changes described by the radiographic scoring system for osteoarthritis of the lumbosacral spine intervertebral disc by Weiner et al. [50] and modified by Edwards et al. [48] (Table 1). In addition, the adjunction of sacro-iliac fixation is supported by many authors to decrease the risk of distal junctional kyphosis or pseudarthrosis [51–55].
Short versus long fusion
In 2014, Kim et al. [56] investigated the radiographic and clinical outcome between patients who underwent short fusions (UIV T9–L1) versus long fusions (UIV T1–T6). In the perioperative period, patients who underwent long fusions sustained longer operating room time and length of stay in the hospital. Nevertheless, the complication rates (including PJK) as well as the radiographic and clinical outcomes at the 2-year follow-up were similar between the groups. Scheer et al. similarly investigated maintenance of radiographic alignment at 2-year follow-up following pedicle subtraction osteotomy (PSO). The authors found that long fusion to T1–T6 was protective against PJK, and associated with lower revision rates as well as increased likelihood of maintaining sagittal alignment [57]. However, the difficulty of treating severe PJK in the cervicothoracic junction may still cause some surgeons to choose a lower thoracic vertebra for the UIV. Moreover, in uncertain cases (for example, if a large correction is indicated but active extension of the thoracic spine is to be preserved), an UIV in the lower thoracic spine may be preferred.
Osteotomy level
Spinal osteotomies are effective techniques that allow for significant correction of alignment in patients with severe sagittal plane deterioration. The optimum level for the osteotomy continues to be debated in the literature. Traditionally, it was thought that if the osteotomy was performed at a caudal spinal level, a smaller angle of resection was needed [31, 58–62]. More recently, Lafage et al. [63] found no relationship between the vertebral level of the osteotomy and the correction in SVA; they concluded that a more caudal osteotomy correlated only with greater correction of PT. Though no studies have demonstrated a difference in outcomes between higher and lower levels of osteotomy, caudal osteotomies may be superior in the ability to restore a more physiological shape of the spine. This distributes most of the LL between L4 and S1, and it could have consequences for both esthetics and distribution of body weight.
In line with the Lafage’s findings, a recent work by the same team investigated the distribution of three-column osteotomy (3CO) correction between the trunk and the pelvis [64]. The authors identified two factors influencing the effects of 3CO on the spino-pelvic complex:
-
1.
Patients who undergo 3CO and achieve significantly greater improvement in truncal inclination are more likely to have larger preoperative SVA and less preoperative pelvic compensation. Conversely, patients with greater preoperative pelvic retroversion are more likely to have improvement in PT after 3CO.
-
2.
Level of lumbar osteotomy: more cephalad osteotomy correlates with greater correction in SVA than PT, while more caudal osteotomy correlates with significantly larger PT correction.
This study demonstrated that to determine the amount of correction obtained from a certain osteotomy level, the patient’s specific deformity must be taken into account. The authors concluded that patients with proportionally high pelvic compensation in relation to truncal inclination may sustain pelvic correction if they undergo caudal osteotomies [64].
Proximal junctional kyphosis (PJK)
Proximal junctional kyphosis is a known complication of deformity surgeries, with reported rates approaching 61 % [65–69]. PJK is a radiographic complication believed to have little or no impact on patient-reported outcomes. The primary exception is esthetic; PJK >20° has been linked to poor scores in the appearance domain of the SRS HRQOL [65–68]. In 2011, a classification of PJK has been proposed by Yagi et al. [67]. The classification aimed to guide treatment decisions, and helps to distinguish less relevant forms of PJK from severe ones. The literature reports a broad spectrum of risk factors for PJK, including short fusion, reciprocal changes in the unfused segments, age, fatty degeneration of the muscle envelope, bone health, and the amount of sagittal correction [66, 70–73]. While numerous preventive measures have been reported in the literature [74, 75], the efficacy of these solutions is still questionable and long follow-up is required to prove their reliability.
Coronal plane
As previously mentioned, the clinical status and HRQOL measures are highly affected by the deterioration of the sagittal plane. Conversely, studies on the relationship between the coronal plane and quality of life revealed that coronal malalignment may be better tolerated than sagittal malalignment in an adult population [76, 77]. Nevertheless, deformity in the coronal plane should not be neglected. Gupta et al. addressed the coronal plane status following sagittal deformity procedures [78]. The authors revealed that 10 % of patients who underwent sagittal realignment procedures were iatrogenically malaligned in the coronal plane. Moal et al. [79] further investigated the ability of sagittal realignment to radiographically restore spino-pelvic alignment in both planes and concluded that the number of patients that was corrected in the coronal plane was similar to the number of patients that deteriorated in their global coronal alignment.
Thus, it is of high importance to surgeons to address the deformity in both sagittal and coronal planes and to differentiate between the patients experiencing exclusively sagittal malalignment and the patients experiencing malalignment in both planes. The SRS-Schwab classification provides an opportunity to do so by classifying patients using the coronal and sagittal modifiers. As a result, this will facilitate communication among treatment providers and provides a standardized language and system to describe their awareness of multiplanar deformities [26]. The direction of coronal imbalance can alter the choice of level of the osteotomy in the lumbar spine: when the coronal imbalance presents towards the concave side of the lumbar scoliosis, an asymmetrical PSO at the base of the lumbar scoliosis is more effective in the restoration of sagittal and coronal balance. In the case of a coronal imbalance towards the convex side, an osteotomy performed at or near the apex of the lumbar curve is more efficacious to correct both deformities.
Selection of the LIV at L5 can result in new coronal imbalance when a rigid coronal tilt of L5 is present preoperatively [80]. Also, the presence of a more rigid segment in a lumbar coronal deformity can result in different degree of correction of two parts of the scoliotic deformity with consequent postoperative coronal imbalance.
Parkinson’s disease
Parkinson disease (PD) is a degenerative neurological condition characterized by tremor, rigidity, bradykinesia, loss of postural reflexes, and alteration of standing balance. [81]. PD patients present with a broad spectrum of alignment abnormalities, such as altered posture and/or deformity. In some patients, PD manifests with an abnormal muscle recruitment pattern in which flexion of the spine, hips, and knees predominates. Camptocormia is the term used to describe this severe alteration in an otherwise flexible spine, and is classically characterized by a forward flexion deformity that spontaneously corrects when the patient is supine. PD patients may also present with a variety of deformities that likely reflect different modalities of dystonia [82]. One of these deformities, antecollis, is a forward flexion posture of the neck. Pisa syndrome is another such deformity, and is typified by coronal deviation of the spine that can be combined with forward flexion. All of these deformities are reversible in supine position.
The treatment of PD postural deformities may overlap with the same medical therapies used for generalized PD symptoms. In some cases, however, antecollis and Pisa syndrome are actually side effects of PD drugs and would thus necessitate treatment with anticholinergic drugs or related modalities. Though the postural changes of PD are in nature reversible and flexible, over time they can lead to rigid deformity. In those cases, the recommended treatment combines drug therapy and, eventually, corrective surgery.
Finally, some PD patients present with genuine deformity of the spine, whether rigid or flexible. These cases may even resemble cases of non-PD collapsing spine, in which the degenerated discs cannot maintain their shape under load and subsequently collapse, resulting in positive sagittal alignment when the patient is standing. In these cases, surgery can be proposed as the main solution. But unlike the typical ASD patient, the PD patient will have a greater tendency of the patient to bend forward as a result of the abnormal neuromuscular activation pattern, and this should be taken into account in surgical correction. Some surgeons, for example, may elect to extend the fusion area to the upper thoracic spine in PD patients with deformity [83].
Previous reports have suggested that the outcomes of spinal surgery in patients with PD may be poorer than in patients without this disease, especially for cases in which instrumented arthrodesis is necessary [84]. Generally, PD patients with primarily structural deformities and low-grade PD tend to respond more predictably to surgery. More severe forms of PD in which malalignment is predominantly postural are less predictable and carry a higher risk of failure.
Kuen et al. evaluated the incidence of sagittal malalignment in a consecutive series of PD patients. Forty-two percent of PD patients had positive sagittal malalignment significantly exceeding the commonly used threshold of SVA >50 mm. Moreover, 51 % of PD patients had spino-pelvic mismatch (PI-LL) >10°, and it was noted that the severity of PD affected the ability to compensate using pelvic retroversion. The authors’ findings suggested that sagittal malalignment in PD is multifactorial; accordingly, thresholds of the sagittal modifiers should be carefully implemented if PD patients are to be realigned [85].
While sagittal alignment reflects how the anatomic shape of the spine permits an economical standing position, sagittal balance is a dynamic parameter and corresponds to the ability of the subject to maintain the stability of the standing position. PD patients have characteristically poor stability, often presenting with greater oscillations in the standing position and a significantly greater likelihood to fall [86]. Long fusions of the spine eliminate some of the mechanisms used to recover the position of the center of mass above the feet, thus reducing the width of the cone of stability of patients. Long fusion in a patient who has intrinsic loss of stability due to PD can result in correct alignment but poor balance and instability, leading to catastrophic, repeated falls. This should be taken into account when treating severe PD patients with sagittal imbalance.
Opportunity 3: what is missing?
Intraoperative control of correction
The literature argues that sagittal alignment measured radiographically is an independent predictor of outcomes. If this is true, every effort should be made to plan surgical procedures with the intention to restore alignment in line with the values that correlate with better clinical outcomes. Geometric and non-geometric methods to calculate the necessary correction have been published and, in some cases, validated. In the hypothetical case of a patient for which a narrow range of possible postoperative alignments provides the best surgical outcomes, preoperative planning should establish an appropriate target of correction and intraoperative control should assure that the target is met at the end of surgery.
Unlike adolescent idiopathic scoliosis, in which the motion segments not included in the fusion are able to compensate, ASD tends to be corrected from the pelvis to the upper spine, leaving little chance for spontaneous realignment. No specific tools currently exist to assess for intraoperative coronal alignment. One possible strategy is obtaining a full-spine radiograph intraoperatively before closure of the wound. When this is not available, an inverted cross made with two rods connected at 90° can be used to check the coronal alignment. In this configuration, the short rod is positioned on the pelvis, and is confirmed with the C-arm to be parallel to the sacral alae. Meanwhile, the long rod is positioned at 90°, extending from the spinous process of S1 to the upper thoracic spine, and the C-arm is used again to verify that it matches with the spinous process of T1.
Sagittal alignment may also be assessed with a similar method. Two parallel shots at S1 and L1 are taken with the C-arm, subsequently followed by images at T2–T3. This allows the surgeon to measure the final lordosis and kyphosis. Furthermore, using the predictive rules described by Lafage [87] the surgeon can estimate the final alignment when the patient stands. If the intraoperative calculations suggest inadequate alignment, additional maneuvers can be performed until correct intraoperative alignment is obtained. Navigation tools may play a role in the future to facilitate the intraoperative calculation and to obtain better matching between the surgical plan and the final result.
Third dimension
The human being is built in three dimensions. The one- or two-dimension solutions of the past are inadequate to analyze of spinal deformities. In 1994, Jean Dubousset raised awareness against the unidimensional thinking [20] and now advocates for a 3D evaluation including the horizontal plane [88] (Fig. 4). While results from 3D analysis in AIS revealed “true” sagittal deformity, little is known on the clinical impact of 3D analysis in the setting of adult spinal deformity [89]. Currently, there is little knowledge on the interpretation and utilization of torsional deformity of the spine in adult deformity.

Three-Dimensional representation of the spine in a patient with adult spinal deformity
Alignment, balance or both?
Efforts to realign the sagittal deformity often overlook the “aging failure of balance” [90]. Alignment and balance are not similar, nor are they opposite; they are, in fact, complementary components of upright posture in humans. Sagittal alignment is a morphological parameter that relates to the relative location of anatomical structures at a given time point. Balance is a dynamic property that depends on numerous factors, including the vestibular, ocular, proprioceptive, and cerebral systems. Bony structures can be surgically realigned, but this may not be sufficient to restore an aged balance. “Balance is the stability within movement” [90], and alignment is just a component of it. As has been discussed in the section dedicated to PD, a better alignment with a rigid spine could paradoxically result in worsened balance and stability. Future research should aim to quantify balance and suggest approaches to improve the accommodation of the neurosensorial system to the new sagittal alignment following surgical intervention.
Muscle envelope
Upright aligned posture is a mission of many components of the musculoskeletal system. The soft tissue envelope is often overlooked in the assessment of patients with spinal deformity. Using MRI, Moal et al. investigated the fatty infiltration in the sets of muscle from the T12 vertebra to the proximal tibia in ASD patients [91]. The authors demonstrated that the lumbar spine extensors had the greatest percentage (32 %) of fat component. Further findings from Moal’s study suggested that the significantly greater degeneration of these muscles is likely not solely attributable to age and BMI [91].
Full body assessment
Full body images allow for lower limb assessment and a comprehensive understanding of the chains of action and counteraction between the components above and below the pelvis. Evaluations of the sagittal plane from head to toe could unmask compensatory mechanisms distant from the spinal deformity driver and help surgical planning (Fig. 5).

Full body sagittal X-ray and potential measurements
Conclusion
While the literature is rich with research on ASD, we identified several opportunities that merited additional consideration and discussion. First, we identified the spinal curvatures and spino-pelvic parameters that are keys to proper alignment, and noted that the correction of these parameters leads to significantly better results in adult deformity surgery. Similarly, the understanding of these sagittal values allows for comprehensive surgical planning that again improves operative outcomes. Several controversies in surgical planning were addressed, with accompanying literature that discusses the ways in which the modalities of surgical execution may prevent radiologic and clinical failures. In addition, the anatomical and biomechanical deformities of PD were discussed as a framework to understand structural and neuromuscular contributions to spinal deformity. Finally, we proposed several suggestions for developing further understanding in the field of sagittal alignment, drawing on the work of our colleagues to explore areas such as the intersection between coronal and sagittal balance, 3D analysis of deformity, and the role of surrounding soft tissues and compensatory mechanisms.
The key points can be summarized as follows:
-
1.
We have greater understanding of the spinal shape and alignment that leads to better results in surgery for ASD.
-
2.
Surgical planning is key to achieving optimum postoperative alignment and improved outcomes.
-
3.
The modalities of surgical execution have a role in the prevention of failures.
-
4.
Neurological conditions such as PD pose unique challenges to the spine surgeon in ASD.
-
5.
Future work in sagittal alignment involves 3D considerations, soft tissue analysis, and better understanding of compensatory mechanisms.
References
Kim YB, Kim YJ, Ahn Y-J et al (2014) A comparative analysis of sagittal spinopelvic alignment between young and old men without localized disc degeneration. Eur Spine J 23:1400–1406. doi:10.1007/s00586-014-3236-8
Barrey C, Roussouly P, Perrin G, Le Huec J-C (2011) Sagittal balance disorders in severe degenerative spine. Can we identify the compensatory mechanisms? Eur Spine J 20(Suppl 5):626–633. doi:10.1007/s00586-011-1930-3
Obeid I, Hauger O, Aunoble S et al (2011) Global analysis of sagittal spinal alignment in major deformities: correlation between lack of lumbar lordosis and flexion of the knee. Eur Spine J 20(Suppl 5):681–685. doi:10.1007/s00586-011-1936-x
Schwab F, Patel A, Ungar B et al (2010) Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine 35:2224–2231. doi:10.1097/BRS.0b013e3181ee6bd4
Schwab F, Lafage V, Farcy J-P et al (2007) Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine 32:2723–2730. doi:10.1097/BRS.0b013e31815a58f2
Youssef JA, Orndorff DO, Patty CA et al (2013) Current status of adult spinal deformity. Global Spine J 3:51–62. doi:10.1055/s-0032-1326950
Liu S, Schwab F, Smith JS et al (2014) Likelihood of reaching minimal clinically important difference in adult spinal deformity: a comparison of operative and nonoperative treatment. Ochsner J 14:67–77
Wang MY, Mummaneni PV, Fu K-MG et al (2014) Less invasive surgery for treating adult spinal deformities: ceiling effects for deformity correction with 3 different techniques. Neurosurg Focus 36:E12. doi:10.3171/2014.3.FOCUS1423
Bridwell KH, Glassman S, Horton W et al (2009) Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: a prospective multicenter evidence-based medicine study. Spine 34:2171–2178. doi:10.1097/BRS.0b013e3181a8fdc8
Smith JS, Shaffrey CI, Berven S et al (2009) Improvement of back pain with operative and nonoperative treatment in adults with scoliosis. Neurosurgery 65:86–93. doi:10.1227/01.NEU.0000347005.35282.6C (discussion 93–94)
Schwab FJ, Hawkinson N, Lafage V et al (2012) Risk factors for major peri-operative complications in adult spinal deformity surgery: a multi-center review of 953 consecutive patients. Eur Spine J 21:2603–2610. doi:10.1007/s00586-012-2370-4
Bianco K, Norton R, Schwab F et al (2014) Complications and intercenter variability of three-column osteotomies for spinal deformity surgery: a retrospective review of 423 patients. Neurosurg Focus 36:E18. doi:10.3171/2014.2.FOCUS1422
Pichelmann MA, Lenke LG, Bridwell KH et al (2010) Revision rates following primary adult spinal deformity surgery: six hundred forty-three consecutive patients followed-up to twenty-two years postoperative. Spine 35:219–226. doi:10.1097/BRS.0b013e3181c91180
Maier SP, Lafage V, Smith JS et al (2013) Revision surgery after three-column osteotomy (3CO) in 335 adult spinal deformity (ASD) patients: intercenter variability and risk factors. Spine J 13:S9–S10. doi:10.1016/j.spinee.2013.07.052
Saban KL, Penckofer SM (2007) Patient expectations of quality of life following lumbar spinal surgery. J Neurosci Nurs 39:180–189
Saban KL, Penckofer SM (2007) Patient expectations of quality of life following lumbar spinal surgery. J Neurosci Nurs 39:180–189
Blondel B, Schwab F, Bess S et al (2013) Posterior global malalignment after osteotomy for sagittal plane deformity: it happens and here is why. Spine 38:E394–E401. doi:10.1097/BRS.0b013e3182872415
Maier S, Smith JS, Schwab F et al (2014) Revision surgery after three-column osteotomy in 335 adult spinal deformity patients: inter-center variability and risk factors. Spine 39:881–885. doi:10.1097/BRS.0000000000000304
Moal B, Lafage VC, Maier SP et al (2014) Discrepancies in preoperative planning and operative execution in the correction of sagittal spinal deformities. North American Spine Society 29th Annual Meeting (San Francisco). Podium Presentation
Dubousset J (1994) Three-dimensional analysis of the scoliotic deformity. In: Weinstein S (ed) The pediatric spine: principles and practices. Raven Press, New York, pp 479–496
Legaye J, Duval-Beaupère G, Hecquet J, Marty C (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7:99–103
Lafage V, Schwab F, Patel A et al (2009) Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine 34:E599–E606. doi:10.1097/BRS.0b013e3181aad219
Vialle R, Levassor N, Rillardon L et al (2005) Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am 87:260–267. doi:10.2106/JBJS.D.02043
Berjano P, Langella F, Ismael M-F et al (2014) Successful correction of sagittal imbalance can be calculated on the basis of pelvic incidence and age. Eur Spine J 23(Suppl 6):587–596. doi:10.1007/s00586-014-3556-8
Schwab FJ, Blondel B, Bess S et al (2013) Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine 38:E803–E812. doi:10.1097/BRS.0b013e318292b7b9
Schwab F, Ungar B, Blondel B et al (2012) Scoliosis research society-Schwab adult spinal deformity classification: a validation study. Spine 37:1077–1082. doi:10.1097/BRS.0b013e31823e15e2
Schwab FJ, Diebo BG, Smith JS et al (2014) Fine-tuned surgical planning in adult spinal deformity: determining the lumbar lordosis necessary by accounting for both thoracic kyphosis and pelvic incidence. North American Spine Society 29th Annual Meeting (San Francisco). Podium Presentation. In: The 21st International meeting on advanced spine techniques (IMAST), Valencia, Spain. Two-Minute Podium Presentation
Been E, Barash A, Marom A, Kramer Pa (2010) Vertebral bodies or discs: which contributes more to human-like lumbar lordosis? Clin Orthop Relat Res 468:1822–1829. doi:10.1007/s11999-009-1153-7
Schultz A, Andersson G, Ortengren R et al (1982) Loads on the lumbar spine. Validation of a biomechanical analysis by measurements of intradiscal pressures and myoelectric signals. J Bone Joint Surg Am 64:713–720
Bergin PF, O’Brien JR, Matteini LE et al (2010) The use of spinal osteotomy in the treatment of spinal deformity. Orthopedics 33:586–594. doi:10.3928/01477447-20100625-22
Ondra SL, Marzouk S, Koski T et al (2006) Mathematical calculation of pedicle subtraction osteotomy size to allow precision correction of fixed sagittal deformity. Spine 31:E973–E979. doi:10.1097/01.brs.0000247950.02886.e5
Smith JS, Klineberg E, Schwab F et al (2013) Change in classification grade by the SRS-Schwab adult spinal deformity classification predicts impact on health-related quality of life measures: prospective analysis of operative and non-operative treatment. Spine 38:1663–1671. doi:10.1097/BRS.0b013e31829ec563
Vialle R, Levassor N, Rillardon L et al (2005) Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am 87:260–267. doi:10.2106/JBJS.D.02043
Vaz G, Roussouly P, Berthonnaud E, Dimnet J (2002) Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J 11:80–87
Vialle R, Levassor N, Rillardon L et al (2005) Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am 87:260–267. doi:10.2106/JBJS.D.02043
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 30:346–353
Margulies JY, Floman Y, Robin GC et al (1998) An algorithm for selection of instrumentation levels in scoliosis. Eur Spine J 7:88–94
Blondel B, Wickman AM, Apazidis A et al (2013) Selection of fusion levels in adults with spinal deformity: an update. Spine J 13:464–474. doi:10.1016/j.spinee.2012.11.046
Kim YJ, Bridwell KH, Lenke LG et al (2007) Is the T9, T11, or L1 the more reliable proximal level after adult lumbar or lumbosacral instrumented fusion to L5 or S1? Spine 32:2653–2661. doi:10.1097/BRS.0b013e31815a5a9d
Cho K-J, Suk S-I, Park S-R et al (2013) Selection of proximal fusion level for adult degenerative lumbar scoliosis. Eur Spine J 22:394–401. doi:10.1007/s00586-012-2527-1
Kuklo TR (2006) Principles for selecting fusion levels in adult spinal deformity with particular attention to lumbar curves and double major curves. Spine 31:S132–S138. doi:10.1097/01.brs.0000236023.08226.90
Lenke LG, Betz RR, Harms J et al (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 8:1169–1181. doi:10.5455/aces.20130422110147
O’Shaughnessy BA, Bridwell KH, Lenke LG et al (2012) Does a long-fusion “T3-sacrum” portend a worse outcome than a short-fusion “T10-sacrum” in primary surgery for adult scoliosis? Spine 37:884–890. doi:10.1097/BRS.0b013e3182376414
Bridwell KH (2004) Selection of instrumentation and fusion levels for scoliosis: where to start and where to stop. Invited submission from the joint section meeting on disorders of the spine and peripheral nerves, March 2004. J Neurosurg Spine 1:1–8. doi:10.3171/spi.2004.1.1.0001
Lamartina C, Berjano P (2014) Classification of sagittal imbalance based on spinal alignment and compensatory mechanisms. Eur Spine J 23:1177–1189. doi:10.1007/s00586-014-3227-9
Kim YJ, Bridwell KH, Lenke LG et al (2006) Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine 31:2359–2366. doi:10.1097/01.brs.0000238969.59928.73
Polly DW, Hamill CL, Bridwell KH (2006) Debate: to fuse or not to fuse to the sacrum, the fate of the L5–S1 disc. Spine 31:S179–S184. doi:10.1097/01.brs.0000234761.87368.ee
Edwards CC, Bridwell KH, Patel A et al (2003) Thoracolumbar deformity arthrodesis to L5 in adults: the fate of the L5-S1 disc. Spine 28:2122–2131. doi:10.1097/01.BRS.0000084266.37210.85
Kuhns CA, Bridwell KH, Lenke LG et al (2007) Thoracolumbar deformity arthrodesis stopping at L5: fate of the L5–S1 disc, minimum 5-year follow-up. Spine 32:2771–2776. doi:10.1097/BRS.0b013e31815a7ece
Weiner DK, Distell B, Studenski S et al (1994) Does radiographic osteoarthritis correlate with flexibility of the lumbar spine? J Am Geriatr Soc 42:257–263
Emami A, Deviren V, Berven S et al (2002) Outcome and complications of long fusions to the sacrum in adult spine deformity. Spine 27:776–786. doi:10.1097/00007632-200204010-00017
Harimaya K, Mishiro T, Lenke LG et al (2011) Etiology and revision surgical strategies in failed lumbosacral fixation of adult spinal deformity constructs. Spine 36:1701–1710. doi:10.1097/BRS.0b013e3182257eaf
Tsuchiya K, Bridwell KH, Kuklo TR et al (2006) Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine 31:303–308. doi:10.1097/01.brs.0000197193.81296.f1
Tumialán LM, Mummaneni PV (2008) Long-segment spinal fixation using pelvic screws. Neurosurgery 63:183–190. doi:10.1227/01.NEU.0000320431.66632.D5
Kebaish KM (2010) Sacropelvic fixation: techniques and complications. Spine 35:2245–2251. doi:10.1097/BRS.0b013e3181f5cfae
Kim HJ, Boachie-Adjei O, Shaffrey CI et al (2014) Upper thoracic versus lower thoracic upper instrumented vertebrae endpoints have similar outcomes and complications in adult scoliosis. Spine 39:E795–E799. doi:10.1097/BRS.0000000000000339
Scheer JK, Lafage V, Smith JS et al (2014) Maintenance of radiographic correction at 2 years following lumbar pedicle subtraction osteotomy is superior with upper thoracic compared with thoracolumbar junction upper instrumented vertebra. Eur Spine J. doi:10.1007/s00586-014-3391-y
Van Royen BJ, De Gast a (1999) Lumbar osteotomy for correction of thoracolumbar kyphotic deformity in ankylosing spondylitis. A structured review of three methods of treatment. Ann Rheum Dis 58:399–406
Cw D (1957) Posterior elementectomy in ankylosing arthritis of the spine. Clin Orthop Relat Res 10:274–281
Van Royen BJ, Gerhard S (1995) Closing-wedge posterior osteotomy for ankylosing spondylitis. Partial corporectomy and transpedicular fixation in 22 cases. J Bone Joint Surg Br 77:117–121
Camargo FP, Cordeiro EN, Napoli MM (1986) Corrective osteotomy of the spine in ankylosing spondylitis. Experience with 66 cases. Clin Orthop Related Res 208:157–167
Van Royen BJ, De Gast a, Smit TH (2000) Deformity planning for sagittal plane corrective osteotomies of the spine in ankylosing spondylitis. Eur Spine J 9:492–498
Lafage V, Schwab F, Vira S et al (2011) Does vertebral level of pedicle subtraction osteotomy correlate with degree of spinopelvic parameter correction? J Neurosurg Spine 14:184–191. doi:10.3171/2010.9.SPINE10129
Lafage V, Diebo B, Schwab F (2014) Spinal alignment formulas and operative planning tools. American Academy of Orthopaedic Surgeons (AAOS) Instructional Course Lectures
Glattes RC, Bridwell KH, Lenke LG et al (2005) Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine 30:1643–1649
Kim Y, Jung J, Bridwell KH, Lenke LG et al (2008) Proximal junctional kyphosis in adult spinal deformity after segmental posterior spinal instrumentation and fusion. Spine 33:2179–2184
Yagi M, Akilah KB, Boachie-Adjei O (2011) Incidence, risk factors and classification of proximal junctional kyphosis: surgical outcomes review of adult idiopathic scoliosis. Spine 36:E60–E68. doi:10.1097/BRS.0b013e3181eeaee2
Hart RA, McCarthy I, Ames CP et al (2013) Proximal junctional kyphosis and proximal junctional failure. Neurosurg Clin N America 24:213–218. doi:10.1016/j.nec.2013.01.001
Cho SK, Shin JI, Kim YJ (2014) Proximal junctional kyphosis following adult spinal deformity surgery. Eur Spine J. doi:10.1007/s00586-014-3531-4
Husson J-L, Mallet J-F, Parent H et al (2010) The lumbar-pelvic-femoral complex: applications in spinal imbalance. Orthop Traumatol Surg Res 96:1–9. doi:10.1016/j.otsr.2010.03.006
Kallman DA, Plato CC, Tobin JD (1990) The role of muscle loss in the age-related decline of grip strength: cross-sectional and longitudinal perspectives. J Gerontol 45:82–88
Balogun JA, Akindele KA, Nihinlola JO, Marzouk DK (1994) Age-related changes in balance performance. Disabil Rehabil 16:58–62
Lafage V, Ames C, Schwab F et al (2012) Changes in thoracic kyphosis negatively impact sagittal alignment after lumbar pedicle subtraction osteotomy: a comprehensive radiographic analysis. Spine 37:E180–E187. doi:10.1097/BRS.0b013e318225b926
Kebaish KM, Martin CT, O’Brien JR et al (2013) Use of vertebroplasty to prevent proximal junctional fractures in adult deformity surgery: a biomechanical cadaveric study. Spine J 13:1897–1903. doi:10.1016/j.spinee.2013.06.039
Cammarata M, Aubin C-É, Wang X, Mac-Thiong J-M (2014) Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine 39:E500–E507. doi:10.1097/BRS.0000000000000222
Glassman SD, Berven S, Bridwell K et al (2005) Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine 30:682–688
Daubs MD, Lenke LG, Bridwell KH et al (2013) Does correction of preoperative coronal imbalance make a difference in outcomes of adult patients with deformity? Spine 38:476–483. doi:10.1097/BRS.0b013e3182846eb3
Gupta MC, Boachie-Adjei O, Cunningham ME et al (2013) Coronal imbalance may be neglected in patients undergoing majority sagittal deformity correction. International Meeting on Advanced Spine Techniques (IMAST)
Moal B, Schwab FJ, Ames CP et al (2014) Radiographic outcomes of adult spinal deformity correction: a critical analysis of variability and failures across deformity patterns. Spine Deformity 2:219–225. doi:10.1016/j.jspd.2014.01.003
Berjano P, Lamartina C (2013) Far lateral approaches (XLIF) in adult scoliosis. Eur Spine J 22(Suppl 2):S242–S253. doi:10.1007/s00586-012-2426-5
Marsden CD, Duvoisin R (1980) Scoliosis and Parkinson’s disease. Arch Neurol 37:253–254
Doherty KM, Van de Warrenburg BP, Peralta MC et al (2011) Postural deformities in Parkinson’s disease. Lancet Neurol 10:538–549. doi:10.1016/S1474-4422(11)70067-9
Bourghli A, Guérin P, Vital J et al (2012) Posterior spinal fusion from T2 to the sacrum for the management of major deformities in patients with Parkinson disease: a retrospective review with analysis of complications. J Spinal Disord Tech 25:E53–E60. doi:10.1097/BSD.0b013e3182496670
Babat LB, McLain RF, Bingaman W et al (2004) Spinal surgery in patients with Parkinson’s disease: construct failure and progressive deformity. Spine 29:2006–2012. doi:10.1097/01.brs.0000138306.02425.21
Oh JK, Smith JS, Shaffrey CI et al (2014) Sagittal spinopelvic malalignment in Parkinson disease: prevalence and associations with disease severity. Spine 39:E833–E841. doi:10.1097/BRS.0000000000000366
Maetzler W, Mancini M, Liepelt-Scarfone I et al (2012) Impaired trunk stability in individuals at high risk for Parkinson’s disease. PLoS ONE 7:e32240. doi:10.1371/journal.pone.0032240
Lafage V, Schwab F, Vira S et al (2011) Spino-pelvic parameters after surgery can be predicted: a preliminary formula and validation of standing alignment. Spine 36:1037–1045
Dubousset J, Charpak G, Dorion I et al (2005) A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: the EOS system. Bulletin de l’Académie nationale de médecine 189:287–297 (discussion 297–300)
Newton PO, Fujimori T, Daan J et al (2014) 3D analysis: the truth about the “Hypokyphosing Effect of Pedicle Screws” in AIS. SRS 49th annual meeting
Dubousset J, Challier V, Farcy J-P et al (2014) Spinal alignment versus spinal balance. Global spinal alignment: principles, pathologies, and procedures book
Moal B, Bronsard N, Raya JG et al (2014) Preliminary results on quantitative volume and fat infiltration of spino-pelvic musculature in adults with spinal deformity (unpublished data)
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Diebo, B.G., Henry, J., Lafage, V. et al. Sagittal deformities of the spine: factors influencing the outcomes and complications. Eur Spine J 24 (Suppl 1), 3–15 (2015). https://doi.org/10.1007/s00586-014-3653-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3653-8