
Abstract
Objective
To investigate and compare blood losses intra and postoperatively between lumbar fusion patients with and without antiplatelet use.
Methods
A total of 106 patients who had undergone at least 2 or more segments of lumbar fusion surgery were selected for the study. They were divided into three groups. Group 1 was not on medication before the surgery. Groups 2 and 3 had taken aspirin prior to the surgery. Group 2 discontinued the medication 1 week before the operation, but group 3 continued the use. In addition, non-steroid anti-inflammatory drug (NSAIDs) use in all patients was questioned. Amount of blood losses and platelet function were evaluated.
Results
When usage of NSAID was not controlled, intraoperative, postoperative, and total blood losses were found to have no statistical significance among the groups. However, when NSAID usage was taken into account, there were significantly higher blood losses in groups 2 and 3 compared with group 1. The use of NSAID resulted in significantly higher blood loss in group 1, but not in groups 2 or 3. The platelet function test results disclosed statistical differences between groups 1 and 2 and groups 1 and 3.
Conclusion
Aspirin significantly increases the risk of bleeding in patients undergoing lumbar fusion at two or more levels. This risk is present even in patients who discontinued aspirin 1 week prior to surgery. In patients with high risk of complications resulting from aspirin discontinuation, the use should be allowed in lumbar fusion surgery. However, strong attention must be paid to avoid excessive bleeding. Because NSAID use also increases surgical blood loss, proper interval from discontinuation to surgery must be granted to minimize the risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In patients who undergo lumbar decompression and posterolateral fusion, one of most serious complications is postoperative bleeding and resultant epidural hematoma that leads to neurologic demise [7]. Excessive bleeding during or after the operation also affects downfall of patients’ general health and postponement of recovery. Surgical method and extent of dissection, number of fusion level, medications, hemodynamic characteristic of a patient and others are considered causes for excessive bleeding [9]. Recently, increased prevalence of cardio- and cerebrovascular diseases proliferated the use of antiplatelet agents for both treatment and prevention. The most commonly used antiplatelet agent is aspirin and the use of non-steroid anti-inflammatory drugs (NSAIDs) for preoperative pain control also shows similar antiplatelet effect. Several studies have shown that patients who had undergone lumbar decompression and posterolateral fusion while taking aspirin had no definite increase in amount of bleeding. Furthermore, no significant difference was shown in frequency of complications between patients with and without aspirin use, and therefore, they reported that patients using single antiplatelet agent does not necessarily require discontinuation of the use to prevent excessive bleeding [2, 5]. As these studies have shown, assertion on increased intra and postoperative bleeding risk with the continued use of antiplatelet agent is under much debate, and studies on increased bleeding due to antiplatelet use in lumbar spinal surgery have been rare in particular. Thus, the authors studied effects of antiplatelet in intra and postoperative bleeding of lumbar fusion operation which has relatively higher blood loss among spine surgeries.
Subjects and methods
Subjects
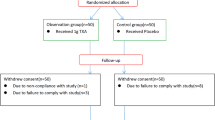
This study was conducted with patients who had undergone decompression and posterolateral fusion on two segments of the lumbar spine at our institution from September 2008 to January 2011. Patients (1) with coagulation disorder, (2) taking an anticoagulant medication preoperatively, (3) taking an antiplatelet agent showing stronger antiplatelet action than aspirin such as clopidogrel, (4) taking a steroid continuously immediately before the surgery, (5) undergoing reoperation, and (6) with dural injury during the operation were excluded. A total of 106 patients meeting these criteria were divided into groups: not taking an antiplatelet agent before the operation (Group 1, 38 patients), taking it before but discontinuing them 1 week prior to the operation (Group 2, 38 ones), and taking it continuously just before the operation (Group 3, 30 ones). Their age, name, underlying diseases, and all medications which were being taken were investigated preoperatively, and the sum of the amount of intraoperative blood loss and postoperatively drained fluid was measured in all three groups to determine the difference in blood loss among the groups.
Administration of aspirin
Out of the 68 patients taking aspirin, 7 took aspirin to prevent cardio- and cerebrovascular diseases without any underlying diseases. Aspirin was given to 46 patients with hypertension as an underlying disease, and they took the medication to prevent the vascular diseases. The rests, 12 and 10 patients, took aspirin to treat or to prevent coronary artery and cerebrovascular diseases without history of stent insertion or balloon angioplasty and due to stent insertion or balloon angioplasty for coronary artery disease, respectively. Through the cooperation with the cardiology department, 22 patients with history of coronary artery and cerebrovascular diseases were educated to take aspirin regardless of the surgery. These patients were classified as group 3. Exception to them, others were asked to discontinue the administration of aspirin 7 days before the surgery by following German guideline for the administration of low dose aspirin in spinal surgery [8], and they were designated as group 2. However, eight took the aspirin continually until the day before the surgery despite of the informing discontinuation, and they were told to keep taking the medication. These patients were included in group 3 also.
Use of NSAID
NSAID was not prescribed for patients who were planned to receive the operation, and they were recommended to discontinue NSAID at a preoperative visit to the outpatient clinic. However, patients, who refused to discontinue the administration, maintained the medication. The administration of NSAID was checked the day before the surgery, and it was designated as a confounding variable to analyze the difference in blood loss by the administration. Out of the 106 patients, 48 took NSAID to the day before the surgery, and groups 1, 2, and 3 had 20, 12, and 16 patients with NSAID use, respectively.
Preoperative platelet function test
This study utilized PFA 100 (Platelet Function Analyzer 100; Dade Behring, Deerfield, IL), and it measured the time to closure (CT) following platelet agglutination between membranes covered with collagen and adenosine diphosphate (ADP) and with collagen and epinephrine. CT can theoretically be measured up to 300 s, and various normal ranges have been proposed. This study used the range from 85 to 165 s as the norm. Because a previous research found that PFA using collagen and ADP cannot detect the abnormality of platelet action caused by aspirin [10], this study checked the level of PFA 100 using collagen and epinephrine a day before the surgery. Considering the finding of Forestier et al. [3] that the postoperative blood loss was related with PFA 100 level, this study analyzed the correlation between PFA 100 level and total blood loss.
Blood loss measurement
All operations were performed by a single surgeon, and intraoperative blood loss was calculated by adding the total suction amount minus the amount of saline used for washing and the weight of gauze used for the surgery minus the weight of dry gauze. Postoperative blood loss was measured with the amount of drained blood through a suction drain inserted during the surgery. The suction drain was maintained until the drained amount was reduced to less than 50 cc per day, and it was removed within seven days after the surgery.
Statistical analysis
All statistical analyses were conducted with PASW statistics 18.0 version. To determine whether statistical differences among the three groups were significant, intra and postoperative blood losses and total blood losses of the three groups were analyzed with ANOVA. If the differences were observed to be significant, significances of the differences between two out of the three groups were checked through post hoc test using the method of Schaffe. The patients from each group were classified into two groups by the administration of NSAID, and their total blood losses were compared with independent T test.
Results
Characteristics of subjects
The mean age of all the subjects was 64.0 ± 9.0 years old. The mean ages of groups 1, 2 and 3 were 61.4 ± 6.7, 66.3 ± 9.4, and 64.3 ± 10.5 years old, respectively, and they showed no significant difference among the three groups (p = 0.787). When diabetes, hypertension, coronary artery disease, and cerebrovascular disease were investigated, the numbers of patients with hypertension were 24, 32, and 20 in groups 1, 2 and 3, respectively, and those with diabetes were 8, 16, and 8 in groups 1, 2, and 3, respectively. The number of patients with history of coronary artery disease was 6 and 10 in groups 2 and 3, respectively, and all patients in group 3 had undergone stent insertion or balloon angioplasty. Cerebrovascular disease was found in four and two patients in groups 2 and 3, respectively. These four underlying diseases among the three groups showed no significance (p > 0.05). The numbers of patients taking NSAID to the surgery were 20, 12, and 16 in groups 1, 2 and 3, respectively. Operation times for each group were 208.4 ± 0.26.3, 199.3 ± 28.7, and 211.3 ± 26.8 min, respectively (p = 0.783) (Table 1).
Blood loss by administration of aspirin
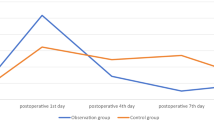
The amounts of intraoperative blood loss were 582.8 ± 259.6, 597.1 ± 336.0, and 668.1 ± 453.7 cc in groups 1, 2 and 3, respectively, and it was not significantly different among the three groups (p = 0.763). The postoperative drained amounts were 603.6 ± 268.5, 684.7 ± 268.6, and 755.6 ± 389.0 cc in groups 1, 2, and 3, respectively, and it also did not show any significant difference (p = 0.175). The total blood losses were 1186.5 ± 383.7, 1281.7 ± 393.6, and 1332.8 ± 464.8 cc in groups 1, 2, and 3, respectively, and it was not significantly different either (p = 0.192) (Table 2).
Blood loss by administration of NSAID
When amount of blood loss was compared after dividing all patients into two groups by the administration of NSAID, the total blood loss of the group taking NSAID continuously before the surgery had 1381.3 ± 345.6 cc, and those not taking it recorded 1074.2 ± 472.8 cc, showing increased blood loss in NSAID administration group (p = 0.017). In group 1, the blood loss of NSAID group (1390.1 ± 370.3 cc) was significantly higher than that of non-NSAID group (960.3 ± 260.1 cc) (p = 0.010). However, statistical difference between NSAID and non-NSAID groups was not observed in groups 2 (1376.8 ± 456.2 vs. 1237.1 ± 205.5 cc) and 3 (1372.0 ± 538.6 vs. 1298.6 ± 425.0 cc) (p = 0.773, p = 0.904) (Table 3).
Comparison of total blood losses in NSAID taking patients in all three groups did not reveal any significance (p = 0.675). Comparisons on patients who had not taken it showed significances between groups 1 and 2 (p = 0.034) and groups 1 and 3 (p = 0.043), but comparison between groups 2 and 3 who had taken aspirin had statistical significance (p = 0.873) (Table 4).
Platelet function test
Results of platelet function test in groups 1, 2, and 3 were 162.7 ± 65.0, 221.1 ± 89.4, and 216.1 ± 92.6 s, respectively. The results revealed no statistical difference between groups 2 and 3 (p = 0.761), but they showed significant differences between groups 1 and 2 (p = 0.029) and groups 1 and 3 (p = 0.011). When platelet function test results of NSAID administered patients were compared in the three groups, no significance was found (p = 0.431). For those who had not taken NSAID, the results were 141.3 ± 32.6, 218.6 ± 40.8, and 225.3 ± 53.5 s in groups 1, 2, and 3, respectively. Groups 2 and 3 did not have any statistical significance (p = 0.870), but between groups 1 and 2 and groups 1 and 3 had significant differences (p = 0.011, p = 0.001) (Tables 5, 6)
Complications
Complications including epidural hematoma and infection were not observed in all three groups, and cardio- or cerebrovascular complications did not occur.
Discussion
The finding that intraoperative blood loss is larger in patients taking aspirin and the increased blood loss raises the risk of complications and surgery has been reported many times not only in cardiac surgery but also in other surgical specialties. Although such studies in spinal surgery have been rare, Merriman et al. [11] reported an antiplatelet administered patient with repeated hematoma after a spinal surgery and insisted that platelet dysfunction caused by aspirin can increase hemorrhage after spinal surgery. In this aspect, surgeons have urged patients to discontinue their use of an antiplatelet agent prior to the surgery to reduce hemorrhage and to prevent its complications. Thus, they should perform operation after the platelet function recovers to the normal level to avoid complications caused by hemorrhage. However, the discontinuation of an antiplatelet agent can provoke other risks in patients with cerebrovascular or cardiovascular disease as an underlying disease and to those with a high risk of the diseases. In fact, Burger et al. [1] said that occurrence of cardiovascular disease after the discontinuation accounted for 10.2 % of all cases, and they recommended that the administration should be discontinued only when the mortality rate and the rate of complications following the increased intraoperative hemorrhage caused by the administration of aspirin were higher than the risk of cardiovascular disease caused by the discontinuation.
In this study, total blood losses did not show any statistically significant difference among the three groups divided by the aspirin administration and the period between the discontinuation and the surgery. Ferraris and Swanson [2] reported that the aspirin use did not increase intraoperative hemorrhage in patients undergoing emergency surgery of obstetrics and gynecology if there was no abnormality in other coagulation factors. Jackics et al. [6] said that the preoperative administration of aspirin did not raise the amount of hemorrhage caused by coronary artery bypass graft (CABG) surgery. However, these results did not consider the confounding action of the preoperative NSAID administration, and most patients undergoing lumbar fusion take NSAID as a part of conservative treatments prior to the surgery. NSAID hinders platelet action by suppressing cyclooxygenase-like aspirin, and it is known to delay clotting and to increase hemorrhage to a similar level as aspirin [13]. Hence, this study considered administration of NSAID as a confounding factor when making the analysis.
Those who had taken NSAID showed no significant differences of total blood loss in three groups. When the total blood losses of patients not taking NSAID were analyzed, it was significantly larger in group 2 who discontinued aspirin 1 week prior to the operation and group 3 who maintained the use than in group 1 who did not take aspirin. This finding implies that after controlling the effect of the confounding factor, NSAID, it became clear on aspirin’s role in platelet dysfunction and larger amount of bleeding in a surgery. However, the difference between groups 2 and 3 revealed no statistical significance. Considering the finding of Patrono et al. [12] that around 50 % of the total platelets recovered to the norm in 5–6 days after the aspirin discontinuation, a week from the discontinuation to the surgery is believed to be insufficient time to recover the normal platelet function.
In this study, the patients in the group 1 who were taking NSAID showed larger amount of blood loss than those not taking NSAID in the same group. NSAID has been currently reported to have antiplatelet action which is equal to that of aspirin [13], and it is considered to discontinue the use during conservative treatments to decrease hemorrhage following surgery. Other treatment options for pain control rather than NSAID are recommended for patients who are scheduled for lumbar fusion surgery. Also, it is imperative to balance the risk or benefit of continued aspirin use in an operation for those who have a history of cerebrovascular or cardiovascular disease, and once a decision was made to continue the use, cautionary measure must be taken to avoid excessive bleeding.
When a patient takes a drug inhibiting the platelet action such as an antiplatelet agent or NSAID, a test to determine whether the platelet function recovers to the normal level and to investigate the extent of the decreased platelet action caused by the administration is necessary. As a test to check the platelet function, platelet level and bleeding times test were used, but platelet function test has been currently found to have better sensitivity and specificity than others and has been recognized as a test to examine preoperative platelet function [4]. However, Thaler et al. [14] also reported that the correlation between results of platelet function test and the amount of blood loss was not significant in hip fracture patients with surgical treatment. This study also investigated whether the platelet function test can be used as a tool to predict the amount of blood loss and found a similar result from the three groups to the result from comparison on blood losses among the same groups. Also, patients (1126.9 ± 740.3 cc) who had platelet function within the normal range (85–165 s) had significant difference when compared with those (1362 ± 613 cc) who had the dysfunction (p = 0.036). Thus, platelet function test is considered a helpful tool in intra and postoperative management of patients by predicting intra and postoperative blood losses.
Some limitations are present in this study. Firstly, the surgeries were conducted by one surgeon in this study without utilizing double blind method, thus the surgeon may have become more careful with intraoperative bleeding control for patients without discontinuation of the antiplatelet agent. Secondly, this study included a relatively small number of patients that had limited control over other factors which may produce an alteration in the amount of blood loss. It only examined the effect of the aspirin administration in a limited manner. Lastly, different types of NSAIDs were taken by the patients. Despite of these limitations, it is meaningful as a study to provide an accurate guideline for patients taking an antiplatelet agent or NSAID in spinal surgery in the future.
References
Burger W, Chemnitius JM, Kneissl GD, Rucker G (2005) Low-dose aspirin for secondary cardiovascular prevention—cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation—review and meta-analysis. J Intern Med 257:399–414. doi:10.1111/j.1365-2796.2005.01477.x
Ferraris VA, Swanson E (1983) Aspirin usage and perioperative blood loss in patients undergoing unexpected operations. Surg Gynecol Obstet 156:439–442
Forestier F, Coiffic A, Mouton C, Ekouevi D, Chene G, Janvier G (2002) Platelet function point-of-care tests in post-bypass cardiac surgery: are they relevant? Br J Anaesth 89:715–721
Franchini M (2005) The platelet function analyzer (PFA-100): an update on its clinical use. Clin Lab 51:367–372
Harder S, Klinkhardt U, Alvarez JM (2004) Avoidance of bleeding during surgery in patients receiving anticoagulant and/or antiplatelet therapy: pharmacokinetic and pharmacodynamic considerations. Clin Pharmacokinet 43:963–981
Jakics J, Lee J, Ikeda S (1999) Preoperative aspirin and heparin therapy does not increase perioperative blood loss and blood product requirements in coronary artery bypass graft surgery. J Anesth 13:8–13. doi:10.1007/s005400050014
Kebaish KM, Awad JN (2004) Spinal epidural hematoma causing acute cauda equina syndrome. Neurosurg Focus 16:e1
Korinth MC, Gilsbach JM, Weinzierl MR (2007) Low-dose aspirin before spinal surgery: results of a survey among neurosurgeons in Germany. Eur Spine J 16:365–372. doi:10.1007/s00586-006-0216-7
Kou J, Fischgrund J, Biddinger A, Herkowitz H (2002) Risk factors for spinal epidural hematoma after spinal surgery. Spine (Phila Pa 1976) 27:1670–1673
Mammen EF, Comp PC, Gosselin R et al (1998) PFA-100 system: a new method for assessment of platelet dysfunction. Semin Thromb Hemost 24:195–202. doi:10.1055/s-2007-995840
Merriman E, Bell W, Long DM (1979) Surgical postoperative bleeding associated with aspirin ingestion. Report of two cases. J Neurosurg 50:682–684. doi:10.3171/jns.1979.50.5.0682
Patrono C, Coller B, FitzGerald GA, Hirsh J, Roth G (2004) Platelet-active drugs: the relationships among dose, effectiveness, and side effects: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 126:234S–264S. doi:10.1378/chest.126.3_suppl.234S
Rothschild BM (2004) Comparative antiplatelet activity of COX1 NSAIDS versus aspirin, encompassing regimen simplification and gastroprotection: a call for a controlled study. Reumatismo 56:89–93
Thaler HW, Frisee F, Korninger C (2010) Platelet aggregation inhibitors, platelet function testing, and blood loss in hip fracture surgery. J Trauma 69:1217–1220. doi:10.1097/TA.0b013e3181f4ab6a (discussion 1221)
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Park, HJ., Kwon, KY. & Woo, JH. Comparison of blood loss according to use of aspirin in lumbar fusion patients. Eur Spine J 23, 1777–1782 (2014). https://doi.org/10.1007/s00586-014-3294-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3294-y