
Abstract
Background/purpose
Measurement and classification of standing posture in the sagittal plane has important clinical implications for adolescent spinal disorders. Previous work using cluster analysis on three gross body segment orientation parameters (lower limbs, trunk, and entire body inclination) has identified three distinct postural groups of healthy subjects before pubertal peak growth: “neutral”, “sway-back”, and “leaning-forward”. Although accurate postural subgrouping may be proposed to be crucial in understanding biomechanical challenges posed by usual standing, there is currently no objective method available for class assignment. Hence, this paper introduces a novel approach to subclassify new cases objectively according to their overall sagittal balance.
Methods
Postural data previously acquired from 1,196 pre-peak height velocity (pre-PHV) subjects were used in this study. To derive a classification rule for assigning a class label (“neutral”, “sway-back”, or “leaning-forward”) to any new pre-PHV subjects, linear discriminant analysis was applied. Predictor variables were pelvic displacement, trunk lean and body lean angle. The performance of the newly developed classification algorithm was verified by adopting a cross-validation procedure.
Results
The statistical model correctly classified over 96.2 % of original grouped subjects. In the cross-validation procedure used, over 95.9 % of subjects were correctly assigned.
Conclusions
Based on three angular measures describing gross body segment orientation, our triage method is capable of reliably classifying pre-PHV subjects as either “neutral”, “sway-back”, or “leaning-forward”. The discriminant prediction equations presented here enable a highly accurate posture class allocation of new cases with a prediction capability higher than 95.9 %, thereby removing subjectivity from sagittal plane posture classification.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Variations in sagittal alignment can be theorized to produce alterations in biomechanical environment in the spinopelvic region, either at the passive tissue, muscular, or motor control level [1–8]. Furthermore, small systematic differences early in life may be hypothesized to result in a considerable increase in accumulated load and/or a gradual process of failure of certain properties, thereby rendering the human spinopelvic complex vulnerable to pain, (progressive) deformity and/or early degenerative changes [1, 2, 4, 8–11]. The adolescent growth spurt, in particular, is considered a critical period for musculoskeletal development [4, 8, 9, 12]. Hence, a paradigm shift in research on sagittal plane posture and its clinical relevance has been proposed concentrating on young adolescent populations, thereby taking biological—rather than chronological—age as a baseline for recruitment and comparisons [13–17]. In this regard, it is important to realize that both age at takeoff (i.e., the onset of growth acceleration) and peak height velocity (PHV) are sex-dependent with these parameters occurring, on average, about 2 years earlier in girls than boys [18].
From a clinical perspective, research involving postural subgroups may exceed the relatively limited view provided by single postural feature approaches. Whereas posture classification is widely being used in clinical practice, relatively few attempts have been made to develop quantitative classification schemes for sagittal alignment in the standing position [15, 16, 19, 20]. With regard to non-adult populations, in particular, the comprehension of sagittal standing balance and the identification of different postural subgroups may imply early treatment possibilities or possibly prevention measures for specific situations according to each postural type, since various morphotypes may contribute to the aggregate risk profile of (progressive) spinal deformity (e.g., adolescent idiopathic scoliosis, Scheuermann’s kyphosis, ankylosing spondylitis, spondylolisthesis) or spinal-pelvic pain states. If postural classification in non-adults is pursued, one should be aware that gender, maturity state and/or age may be potential confounders [14, 21, 22]. Accordingly, a scientifically sound and clinically meaningful classification scheme has recently been developed for healthy boys and girls at pre-peak height velocity (pre-PHV) age [15, 16]. This scheme involved a fresh and systematic approach to posture type recognition and considered the interactions between three gross body segment orientation parameters (legs, trunk, and entire body) as the primary features discriminating between posture classes. As such, three postural categories could be distinguished: “neutral”, “sway-back” and “leaning-forward”. In support for its clinical relevance, a differential association of spinal pain prevalence rates to “non-neutral” versus “neutral” alignment was found, in that sway-back boys were ~2 to 3 times more likely to report low back or neck pain when compared to boys categorized as neutral [15]. Furthermore, with respect to those boys who had a thoracic spine pain history, a tendency towards a low prevalence for care seeking because of their pain was noted in the neutral group when compared to the sway-back and leaning-forward groups (8, 25 and 20 %, respectively). Nonetheless, this latter finding did not reach statistical significance [15]. Further support for the categorizing system proposed by Dolphens et al. [15, 16] was derived from the finding that—for the first time—clinically relevant sex differences in sagittal standing posture features were established at pre-PHV age [16, 17]. Generally, these differences in spinopelvic, lower limb and entire body alignment between genders were concealed by examining an aggregate pre-PHV population [13, 14], and turned up only when the classification was applied. Since these exciting results probably represent sex variation in the antero-posterior position of the truncal and/or entire body’s center of gravity with respect to specific spinopelvic structures (i.e., when corresponding posture types are considered), they may add to our understanding of sex-related prevalence ratios for the progressive forms of some spinal deformities (e.g., adolescent idiopathic scoliosis, ankylosing spondylitis or spondylolisthesis) via a biomechanical rationale.
Despite the widespread use of postural subgrouping in clinical practice, appropriate methods to perform an objective posture type assignment are lacking. Instead, to this date, subtype decision ultimately relies on the clinician’s individual judgment. Hence, the aim of this work was to develop a classification algorithm of pre-PHV subjects from three postural subgroups (neutral, sway-back, and leaning-forward) on the basis of three gross body segment orientation features. The underlying object and motive for this study was to strengthen the link between clinic and laboratory.
Methods
As part of a larger study on sagittal standing alignment and its clinical relevance at pre-PHV age, 1,196 healthy young adolescents were recruited [639 boys of mean age 12.6 (SD 0.54) years and 557 girls of mean age 10.6 (SD 0.47) years]. Male and female study members were 1.2 (SD 0.71) and 1.2 (SD 0.59) years before pubertal peak growth, respectively, as calculated using gender-specific predictive equations [23]. The study was approved by the local ethics committee at our institution. Before enrollment, each participant and a parent or guardian of each participant gave written informed consent.
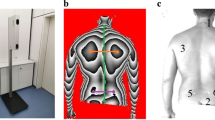
Retro-reflective markers were placed on the C7 spinous process and left greater trochanter by one trained examiner with clinical experience. A set of standardized lateral photographs was taken with each subject standing in his usual posture, equally balanced on both feet, arms by the sides and looking straight ahead. Using ImageJ software (National Institutes of Health, Bethesda, MD, USA), three angular measures describing gross body segment orientation relative to the vertical were quantified. These were pelvic displacement angle, trunk lean angle (i.e., C7 plumb line referenced to the greater trochanter) and body lean angle (Fig. 1). For more detailed methods, see previous articles by Dolphens et al. [13, 14].

Angular measures used in cluster and discriminant analyses: a pelvic displacement angle, b trunk lean angle, c body lean angle
Based on cluster analysis of the three postural measures, subjects were previously divided in three postural categories (neutral, sway-back, leaning-forward) [15, 16]. A stick figure representation of these posture clusters is shown in Fig. 2. Of the total of 639 boys, 266 were classified as neutral (41.6 %), 199 as sway-back (31.1 %) and 174 as leaning-forward (27.2 %). In the female data set (n = 557), these figures were 223 (40.0 %), 177 (31.8 %) and 157 (28.2 %), respectively.

Stick figure representation of the posture types obtained by cluster analysis [15, 16]. 1 Neutral global alignment (characterized by a small pelvic displacement angle, small trunk lean angle and a body lean angle close to 0), 2 sway-back [characterized by an intermediate pelvic displacement angle, large trunk lean angle and a large (positive) body lean angle], 3 leaning-forward [characterized by a large pelvic displacement angle, intermediate trunk lean angle and a small (negative) body lean angle]
To explore the possibility of classifying pre-PHV subjects accurately into one of the three “global” alignment clusters and to address the question of how to assign new cases to these groups, linear discriminant analysis (LDA) was carried out using SPSS (v.20.0, Statistical Package for the Social Sciences, Chicago, IL, USA). LDA is a supervised classificatory technique that maximizes group differences by creating a weighted linear combination of the discriminating (predictor) variables [24–26]. Where k is the number of subgroups, LDA involves the computation of k−1 discriminant functions with a form as follows:
where D discriminant function, b the discriminant coefficient or weight for that variable, X discriminating variables, i.e., respondent’s score for that variable, c a constant and n the number of predictor variables.
In the present study, predictors of membership in the three cluster groups were pelvic displacement, trunk lean and body lean angle. For each discriminant function, values of Wilks’ lambda (λ w) were obtained. Whereas values of λ w approaching 0 indicate well-resolved categories, overlapped categories make λ w to approach 1. To verify the performance of our classification algorithm, a cross-validation procedure (leave-1-out method) was adopted. The classification accuracy was determined by computing (1) sensitivity (i.e., true positive predictions/total positive cases), (2) specificity (i.e., true negative predictions/total negative cases) and (3) overall classification accuracy (i.e., total number of samples correctly classified/total number of samples).
Results
The mathematical model built by applying the LDA procedure on the three gross body segment orientation parameters as predictors, provided two significant linear classification functions for each gender.
-
Boys
D 1 = 0.570 × pelvic displacement angle + 0.206 × trunk lean angle − 0.225 × body lean angle − 4.172.
D 2 = −0.082 × pelvic displacement angle + 0.269 × trunk lean angle + 0.739 × body lean angle − 1.320.
-
Girls
D 1 = 0.475 × pelvic displacement angle + 0.359 × trunk lean angle − 0.184 × body lean angle − 4.714.
D 2 = −0.307 × pelvic displacement angle + 0.304 × trunk lean angle + 0.671 × body lean angle − 1.285.
In boys, the first discriminant function accounted for 60.3 % of the differences among the three groups (λ w = 0.202, P < 0.001). The second discriminant function explained the remaining variance (39.7 %) and was also statistically significant (λ w = 0.504, P < 0.001). In girls, the first discriminant function accounted for 57.2 % of the discriminant variance (λ w = 0.193, P < 0.001), whereas the second function accounted for an additional 42.8 % of the variance (λ w = 0.476, P < 0.001). The scatter plot in Fig. 3 shows the projection of the data points onto the 2D linear discriminant score space. This figure shows good performance of LDA for class separation as indicated by the weak overlap of classes in the discriminant score space.

Score plot on a 2D linear discriminant score space defined by the significant discriminant functions of the LDA model constructed to resolve the neutral, sway-back and leaning-forward categories. a Discriminant function plot for boys (n = 639), b discriminant function plot for girls (n = 557)
With regard to the relative importance of the independent (predictor) variables in the classification procedure, the discriminant coefficients in the gender-specific models presented above show that function 1 was dominated by the pelvic displacement angle in boys and by the trunk lean and pelvic displacement angle in girls. Function 2 was dominated by the body and trunk lean angle in both genders.
For the originally derived cases, the statistical model resulted in correct classification in 97.5 % of cases among boys (sensitivity (100 % (neutral), 96.5 % (sway-back) and 94.8 % (leaning-forward); specificity (96.8 % (neutral), 99.5 % (sway-back) and 99.6 % (leaning-forward)) and in 96.2 % of cases among girls [sensitivity (100 % (neutral), 96.6 % (sway-back) and 90.4 % (leaning-forward); specificity (94.3 % (neutral), 99.7 % (sway-back) and 99.8 % (leaning-forward)]. With respect to the cross-validation procedure used, the classification performance is summarized in the confusion matrix shown in Table 1. In sum, 97.0 % of the male cross-validated set and 95.9 % of the female cross-validated set were correctly assigned. This relatively consistent pattern indicates that the statistical classification model is robust and capable of discriminating accurately between postural subgroups as determined previously by cluster analysis.
Discussion
The primary goal for this study was to determine whether gross body segment orientation scores could be combined to differentiate between postural subgroups and, by extension, to predict group membership. LDA was performed using the pelvic displacement, trunk lean and body lean angles as predictors of membership in the “global” alignment groups as previously obtained by cluster analysis [15, 16]. Our results demonstrate that discriminant function analysis provides an effective and reliable means for classifying pre-PHV subjects according to their habitual standing posture, thereby eliminating subjectivity in sagittal plane posture classification. A classification as either “neutral”, “sway-back” or “leaning-forward” was achieved with high accuracies, as corroborated by a correct classification of >96.2 % for the originally derived cases with this latter feat falling minimally to 95.9 % for the cross-validation procedure. Hence, with regard to class prediction, a new case can be assigned reliably to a postural category by simply entering the person’s scores on the predictor variables in the discriminant functions presented here. Overall, the pelvic displacement angle was found to have the largest discriminant capability in boys, whereas the trunk lean and pelvic displacement angle were the major factors in girls.
Accurate classification into postural subtypes has been proposed to be critical for understanding sagittal balance in standing and its clinical relevance [4, 15–17, 20, 27]. In non-adult populations, for example, posture classes could be relevant to early stage diagnosis of disease progression. The method presented here to perform postural subgrouping in pre-PHV subjects is the first to produce quantitative and repeatable results, since the categorization is scored by a classification algorithm rather than by an observer. This novel and attractive approach enables an automatic, rapid and accurate identification of overall standing balance by means of three simple clinical measures. We expect that the adoption of our LDA for statistical classification will facilitate basic and clinical research towards a better understanding of sagittal plane alignment at young age as a mechanical risk factor for spinal disorder development, including spinal pain and deformity. Future prospective research is necessary to unveil the long-term relevance of postural alignment at pre-PHV age, indeed.
In utilizing our classifier based on LDA, one may argue that the method presented here only applies to pre-PHV subjects. This limitation could be overcome in the future by developing similar sound categorization schemes and prediction rules by means of cluster and determinant analyses, respectively, thereby covering subjects of other age and/or maturity groups. Future work elaborating on postural classification in other populations should be encouraged, indeed, yet this was beyond the scope of the present article. Neither did we aim here to reveal the “chicken or egg” dilemma regarding different postural types and spinal disorders, possible underlying mechanisms of such associations or potential long-term effects. A second limitation of the present research paper might involve the use of cluster analysis results [15, 16] as the gold standard, which implies that good performance of the postural classification model refers to good prediction of the classification obtained via cluster analysis. Nevertheless, the analytical method presented here enables an objective class allocation into a scientifically sound and practically oriented classification scheme that proved both clinically meaningful and relevant [15–17].
Conclusions
The present study establishes the feasibility of classifying pre-PHV subjects according to their overall sagittal standing alignment by applying a linear discriminant classifier using a person’s scores on three simple angular measures: pelvic displacement, trunk lean and body lean angle. With the application of our LDA model, pre-PHV subjects can correctly be classified as either “neutral”, “sway-back” or “leaning-forward” with a prediction capability higher than 95.9 %. The discriminant prediction equations presented here enable an objective class allocation of subjects who are in a critical phase of musculoskeletal development into a postural classification scheme that proved both clinically meaningful and relevant. As such, they may be an aid for both the clinician and researcher.
References
Scannell JP, McGill S (2003) Lumbar posture—should it, and can it, be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Phys Ther 83:907–917
Keller TS, Colloca CJ, Harrison DE, Harrison DD, Janik TJ (2005) Influence of spine morphology on intervertebral disc loads and stresses in asymptomatic adults: implications for the ideal spine. Spine J 5:297–309
Mitchell T, O’Sullivan PB, Burnett AF, Straker L, Smith A (2008) Regional differences in lumbar spinal posture and the influence of low back pain. BMC Musculoskelet Disord 9:152
Kendall FP, McCreary EK, Provance PG (1993) Muscles: testing and function, with posture and pain. Williams & Wilkins, Baltimore
Pezolato A, de Vasconcelos EE, Defino HLA, Nogueira-Barbosa MH (2012) Fat infiltration in the lumbar multifidus and erector spinae muscles in subjects with sway-back posture. Eur Spine J 21:2158–2164
Falla D, O’Leary S, Fagan A, Jull G (2007) Recruitment of the deep cervical flexor muscles during a postural-correction exercise performed in sitting. Man Ther 12:139–143
O’Sullivan PB, Grahamslaw KM, Kendell M et al (2002) The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine 27:1238–1244
Nissinen MJ, Heliövaara MM, Seitsamo JT, Könönen MH, Hurmerinta KA, Poussa MS (2000) Development of trunk asymmetry in a cohort of children ages 11 to 22 years. Spine 25:570–574
Dickson RA (1988) The aetiology of spinal deformities. Lancet 1:1151–1155
Janssen MMA, Drevelle X, Humbert L, Skalli W, Castelein RM (2009) Differences in male and female spino-pelvic alignment in asymptomatic young adults: a three-dimensional analysis using upright low-dose digital biplanar X-rays. Spine 34:E826–E832
Masi AT, Dorsch JL, Cholewicki J (2003) Are adolescent idiopathic scoliosis and ankylosing spondylitis counter-opposing conditions? A hypothesis on biomechanical contributions predisposing to these spinal disorders. Clin Exp Rheumatol 21:573–580
Patton GC, Viner R (2007) Pubertal transitions in health. Lancet 369:1130–1139
Dolphens M, Cagnie B, Coorevits P et al (2012) Sagittal standing posture and its association with spinal pain: a school-based epidemiological study of 1196 Flemish adolescents before age at peak height velocity. Spine 37:1657–1666
Dolphens M, Cagnie B, Vleeming A, Vanderstraeten G, Coorevits P, Danneels L (2012) A clinical postural model of sagittal alignment in young adolescents before age at peak height velocity. Eur Spine J 21:2188–2197
Dolphens M, Cagnie B, Coorevits P, Vleeming A, Danneels L (2013) Classification system of the normal variation in sagittal plane alignment: a study among young adolescent boys. Spine 38:E1003–E1012
Dolphens M, Cagnie B, Coorevits P, Vleeming A, Danneels L (2013) Classification system of the sagittal standing alignment in young adolescent girls. Eur Spine J. doi:10.1007/s00586-013-2952-9
Dolphens M, Cagnie B, Vleeming A, Vanderstraeten G, Danneels L (2013) Gender differences in sagittal standing alignment before pubertal peak growth: the importance of subclassification and implications for spinopelvic loading. J Anat (revision submitted 07/2013. JANAT-2013-0136. Currently under review)
Malina RM, Bouchard C, Bar-Or O (2004) Growth, maturation, and physical activity. Human Kinetics, Champaign
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J (2005) Classification of the normal variation in the sagittal salignment of the human lumbar spine and pelvis in the standing position. Spine 30:348–353
Smith A, O’Sullivan P, Straker L (2008) Classification of sagittal thoraco-lumbo-pelvic alignment of the adolescent spine in standing and its relationship to low back pain. Spine 33:2101–2107
Poussa MS, Heliövaara MM, Seitsamo JT, Könönen MH, Hurmerinta KA, Nissinen MJ (2005) Development of spinal posture in a cohort of children from the age of 11 to 22 years. Eur Spine J 14:738–742
Widhe T (2001) Spine: posture, mobility and pain. A longitudinal study from childhood to adolescence. Eur Spine J 10:118–123
Mirwald RL, Baxter-Jones ADG, Bailey DA, Beunen GP (2002) An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc 34:689–694
Duda RO, Hart PE, Stork DG (2000) Pattern classification. Wiley, New York, pp 117–120
Kleinbaum DG, Kupper LL, Muller KE (1988) Applied regression analysis and other multivariable methods. PWS-Kent Publishing, Boston
Vandeginste BGM, Massart DL, Buydens LMC, De Jong S, Lewi PJ, Smeyers-Verbeke J (1998) Data handling in science and technology. Handbook of chemometrics and qualimetrics: part B. Elsevier Science B.V., Amsterdam
Roussouly P, Pinheiro-Franco JL (2011) Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur Spine J 20(S5):S609–S618
Conflict of interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dolphens, M., Cagnie, B., Coorevits, P. et al. Posture class prediction of pre-peak height velocity subjects according to gross body segment orientations using linear discriminant analysis. Eur Spine J 23, 530–535 (2014). https://doi.org/10.1007/s00586-013-3058-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-013-3058-0