
Abstract
Introduction
Study aim was to find out if patients with Lenke type 1 curve exhibit smaller pedicles and specific pedicle width pattern compared with individuals with no scoliosis.
Materials and methods
4,828 pedicle width measurements (T1–L5) in 61 consecutive patients with adolescent idiopathic scoliosis of Lenke type 1 curve, 61 control subjects, and 20 patients with Lenke type 5 curve, were retrospectively performed by an experienced neuroradiologist.
Results
Among patients with Lenke type 1 curve, the differences between the width of right and left upper thoracic pedicles were statistically significant; smallest at right T4 (2.6 mm). At scoliotic apex, the pedicles on the concave (left) side were significantly smaller than those on the convex (right) side; smallest at left T7 (3.2 mm). Among patients with Lenke type 1 curve, 97% had pedicle width <4 mm.
Conclusions
Our study showed that patients with Lenke type 1 curve exhibit smaller pedicles and asymmetric pedicle width compared with control subjects.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Many reports have shown that segmental pedicle screw fixation in patients with adolescent idiopathic scoliosis (AIS) results in better three-dimensional deformity correction and higher pullout strength with subsequent improvement of the biomechanical stabilization when compared with other correction techniques [1–4]. Although the rate of neurovascular complications associated with screw misplacement in scoliosis surgery usually reported to be almost 0% [3, 5–7], reports on serious complications associated with screw misplacement have been published since the introduction of this procedure [8–11]. As segmental pedicle screw fixation has become a widely used method in scoliosis corrective surgery, the knowledge about the pedicle morphometry has become increasingly essential. Preoperative computed tomography (CT) or magnetic resonance imaging (MRI) enables the estimation of pedicle width, length and inclination. Low-dose spine CT with at least 20-fold reduction of the radiation doses has recently been introduced as a reliable method in the perioperative work-up of scoliosis [12]. Numerous reports on the pedicle morphometry in normal individuals as well as in cadavers and in patients with AIS have been published [13–20]. Many of these studies have pointed out a significant reduction of pedicle width at the concavity of the curve. Reports in normal population often include individuals of different age groups that make them unsuitable for comparison with patients with AIS [14, 15]. Liljenqvist et al. [17, 18] were among the first who presented data on pedicle morphometry based on patients data using CT and MRI17, 18, but their assessments were focused only on the morphological changes at the level of scoliotic apex. Upendra et al. [19] has recently published a report on pedicle morphometry of the whole spine in patients with scoliosis of King curve type II, III and IV.
We assessed the pedicle width in a more homogeneous group of patients with AIS, namely patients with Lenke type 1 with a single major structural thoracic curve. Our primary aim was to estimate the pedicle width in these patients. The second aim was to test the hypothesis, based on our own radiological and surgical observation, that these patients usually exhibit specific pattern with very small pedicles on the left (concave) side of the scoliotic apex as well as on right side of the upper thoracic pedicles.
Materials and methods
Low-dose CT has been used at our institution in the pre- and the postoperative work-up of patients with scoliosis since autumn 2005. The low-dose CT means a radiation dose of only 0.37 mSv per CT-examination covering 15 vertebral bodies (scan length of 36 cm) [12]. Sixty-one consecutive patients with AIS with Lenke type 1 curve (examined between January 2006 and September 2010) were included in this retrospective study. All CT examinations were performed on a 16-slice CT-scanner (SOMATOM Sensation 16, Siemens AG, Forchheim, Germany) according to our low-dose spine CT protocol: slice collimation 16 × 0.75 mm, rotation time 0.75 s, pitch 1.5, tube voltage 80 kV and quality reference for the effective tube current-time product 25 mAs. For comparison of the pedicle width measurements, an age- and sex-matched control subject was included (n = 61) with mean, median and range of age exactly similar to that of patients with Lenke type 1 curves. The control group included patients who underwent CT of thorax and abdomen following trauma during the period January 2006–September 2010. Control subjects whose CT showed spinal injuries or spinal deformity were excluded from the study analysis. Furthermore, 20 consecutive AIS patients with a Lenke type 5 curve (a single major structural thoracolumbar/lumbar curve) examined during the same period (January 2006–September 2010) were also included to test for the occurrence of any specific pedicle width pattern.
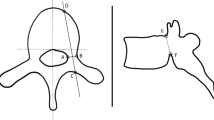
The measurements of the pedicle width were performed by an experienced neuroradiologist (KAK). The pedicle width measurements (n = 4,828; 34 pedicle width measurements T1–L5 per individual) were performed in the Picture Archiving and Communication System (SECTRA, IDS7) using 1-mm thick axial images with skeletal algorithm and skeletal window (window center 700 and window width 2,600). The pedicle width was measured as the smallest transverse diameter between the lateral border of outer cortex and the medial border of inner cortex of the pedicle perpendicular to the line of the expected ideal trajectory of the thoracic pedicle screw at the level of the pedicle rib unit (Fig. 1).

The way of measurement of pedicle width. The pedicle width was measured as smallest transverse diameter between lateral border of outer cortex and the medial border of inner cortex of the pedicle (a, b) perpendicular to the line of the expected ideal trajectory of the thoracic pedicle screw (c, d) at the level of the pedicle rib unit
The use of low-dose spine CT in the work-up of patients with AIS was approved by the Regional Radiation Protection Committee.
Statistical analysis
All statistical analyses were performed by means of SPSS version 17. Data are presented as proportions (%) or as mean ± standard deviations (SD). Spearman correlation was used to test the association between continuous variables and Mann–Whitney U or Kruskal–Wallis test to test the association categorical and continuous variables.
Results
Pedicle width in different study groups
Patients and curve characteristics are shown in Table 1.
Among patients with Lenke type 1 curve, the differences between the pedicle width of the right side and the left side was statistically significant at T2–T5 with smaller pedicles on the right side (at the concavity of the minor compensatory curve); smallest at T4 (mean value 2.6 mm), Table 2. At and around scoliotic apex (T7–T9), the pedicles on the left (concave) side were significantly smaller than corresponding pedicles on the right side; smallest at T7 (mean value 3.2 mm), Table 2. The pedicles of L3 and L4 were also significantly smaller on the left side than on right side. Pedicles among control subjects exhibited an almost similar width on both sides, Table 2. Among AIS patients with Lenke type 5 curve, there were no significant differences in pedicle width between the right and the left side around the apical vertebra (T12–L2). However, the pedicles on the convex side at T7–T8 (at the concavity of the minor compensatory curve), which are few vertebral levels above the major scoliotic apex, were significantly smaller than those on the concave side, Table 2.
Differences in pedicle width between different study groups
The width of the pedicles at all vertebral levels (except at right pedicle of T11) was smaller among patients with Lenke type 1 curve compared with control subjects. The differences were statistically significant at the majority of the vertebral levels on the right side, Table 3. Among patients with Lenke type 1 curve, the pedicles of T2–T4 on the right (convex side of the major curve) were 1.1 mm smaller than corresponding pedicles among patients with Lenke type 5 curve, Table 3. The same applied to the pedicles of T7–T8 on the left (concave) side, which were 0.9 and 0.8 mm, respectively, smaller than corresponding pedicles among patients with Lenke type 5 curve, Table 3. The patterns of pedicle width among the three different study groups are shown in Figs. 2 and 3.

The pedicle width at the right side (convex side of the major curve in patients with AIS) at the vertebral levels T1–L5

The pedicle width at the left side (concave side of the major curve in patients with AIS) at the vertebral levels T1–L5
Among patients with Lenke type 1 curve, 97% had pedicle width <4 mm and 62% had pedicle width <3 mm on right side at the level of T4. Corresponding values for T3 were 85 and 66%, respectively, and for T5 were 79 and 41%, respectively, Table 4. On the left side (major curve concavity), 80, 72 and 51% of the patients with Lenke type 1 curve had pedicle width <4 mm at the level of T7, T8 and T9, respectively, Table 4. In comparison to the control subjects, the differences between the proportions of patients with Lenke type 1 curve that exhibited pedicle <4 mm were statistically significant at all levels and at both sides T2–T10 as well as at L1 and L2, Table 4.
Correlation between pedicle width and different studied variables
Only at T3 on the right side, pedicle width was significantly smaller in females than males (2.8 vs. 3.5 mm) among patients with Lenke type 1 curve (Chi square test, p = 0.02). The correlation between pedicle width and the gender was not statistically significant in the remaining vertebral levels. No correlation was found between the pedicle width on one hand and the age or the degree of vertebral rotation on the other hand at any of the studied vertebral levels. Patients with Lenke type 1 curve were divided into two groups [≤15 years (n = 15) vs. ≥16 years (n = 31)]. There was no statistically significant difference between the pedicle width at the upper thoracic levels nor around the scoliotic apex between these two age groups, Table 5.
Only at T2 on the right side, the Cobb angle of the major curve was correlated to the pedicle width (Spearman correlation, p = 0.04). The mean value of Cobb angle among patients exhibited pedicle width <4 mm at the level of T2 was 58.5° compared with 50.3° among those with pedicle width ≥4 mm. The correlation between pedicle width and the Cobb angle of the major curve was not statistically significant in the remaining vertebral levels. However the small pedicles at T3 and T4 on the right side was correlated to the Cobb angle of the minor curve (Spearman correlation p = 0.007 and 0.020, respectively).
The pedicle width of T2 on the right side was in mean 3.7 mm among patients with Lenke type 1C curve compared with 4.4 and 5.4 mm among patients with Lenke type 1A curve, and type 1B curve, respectively (Kruskal–Wallis test, p = 0.01). At the remaining vertebral levels, there were no correlations between the pedicle width and the Lenke curve subtypes (A–C).
The pedicle width was not correlated with the degree of vertebral rotation, or with the Cobb angle of the major or the minor curve among patients with Lenke type 5 curve.
Discussion
This study showed that the pedicles in patients with AIS having Lenke type 1 curve are universally smaller than those in corresponding vertebrae in control subjects, with a clear asymmetry between the right and the left sided pedicles. Patients with AIS of Lenke type 1 curve exhibit a specific pattern not only on the left (concave) side at the scoliotic apex but also on the right (convex) side at the upper thoracic pedicles (concavity of the compensatory minor curve). Almost the same pattern has been shown in cadaveric spines with scoliosis [13]. Beside control subjects, our study has, however, also included patients with Lenke type 5 curve with single major structural thoracolumbar/lumbar curve. Patients with Lenke type 5 curve did not exhibit similar pattern of pedicle width reduction on the right side of the upper thoracic pedicles or asymmetry of the pedicle width at the apex of the major curve, often at the thoracolumbar or upper lumbar vertebrae. In patients Lenke type 5 curve, a significant pedicle narrowing was noticed at the convex side of the major curve few vertebral levels (T7–T8) above the apex (apex often thoracolumbar/lumbar), which is quite similar to the narrowing on the right (convex) side few vertebral levels (T2–T5) above the apex in patients with Lenke curve type 1 (apex often at T8–T9).
Small pedicles at the concave side of the scoliotic apex have also been shown by two previous studies [17, 19]. Pedicle width measurements reported by Liljenqvist et al. [17] were almost similar to the results of our study whereas Upendra et al. [19] surprisingly showed wider pedicles almost throughout the curve. In several levels, data on pedicle width reported by Liljenqvist et al. [17] showed smaller pedicles than our data. This may be explained by the fact that they presented the endosteal pedicle width whereas our data represent measurements between the inner and the outer cortex of the pedicles including the whole pedicle thickness. As pedicle screws with minimal cortical perforation showed to improve the biomechanical strength of the construct [21], we therefore included the whole pedicle cortex in the measurements of the pedicle width. The differences between our data and their data [17] were, however, ≤1 mm throughout the studied vertebral levels.
The data reported by Parent et al. [13] were based on cadaveric spine (scoliosis group and normal group) subjected for digitizing procedure developed for the purpose of the study. The authors claimed that their digitizing method recorded the exact surface measurements of the object measured and that axial images (CT or MRI) might not provide the perfectly oriented image in the transverse plane of the vertebrae directly at the level of the smallest diameter of the pedicles. In clinical practice, the axial CT images are, however, the usually used source of images for measurements of pedicle width. Availability of very thin slice collimation (0.75 mm in our CT-system and in most of the available multidetector CTs today) enables reconstruction of the axial images parallel to the pedicle on the sagittal plane and thus provides accurate axial orientation of the pedicles even in images obtained by CT. Data presented by Parent et al. [13] were similar to our results by showing the same trend of pedicle narrowing on the right side of the upper thoracic pedicles and on the left at the scoliotic apex with smallest pedicle width at T4 (mean value 2.6 mm).
Our study is a consecutive study including a large number of pedicles of two well defined homogeneous patient groups and included also an age- and sex-matched control group. A drawback of this study is that the measurements were performed by only one reader. The assessment of the reliability of CT in the measurement of the pedicle width is not the subject of this study as low-dose CT has previously been proved to be a reliable method in the measurements of pedicle width with an interobserver and intraobserver random error of difference of 0.3 mm [12]. Therefore, the measurements of this study were performed by only one reader who is experienced in the evaluation of images of patients with spinal deformities.
We believe that our findings of the extreme pedicle narrowing at several vertebral levels among the majority of patients with Lenke curve type 1 (e.g. 66% had pedicle width of <3 mm at T3 on the right side) exhibit an important clinical implication. Upon pedicle screw insertion, these findings mean the need to use smaller pedicle screws in the right upper thoracic pedicles (T2–T5) and in the left pedicles at the curve concavity (T7–T9) to avoid (a) medial cortical perforation and spinal canal encroachment with risk for spinal cord injury, and (b) lateral cortical perforation with increasing risk for injury to vital structures such as aorta, trachea, oesophagus ad pleura. The screw insertion at levels with pedicle width <3 mm might need to be performed with an in-out-in technique and hooks might need to be considered as an alternative type of anchor in some cases.
Conclusion
This study showed that patients with Lenke type 1 curve exhibit smaller pedicles than control subjects, asymmetric pedicle width, and smaller pedicles at the concave side of the apex as well as at the opposite side in the upper thoracic vertebrae. The most remarkable finding of this study was that the reduction of the pedicle width was more pronounced at the upper thoracic vertebra than at the scoliotic apex of the major curve. In most of the studied vertebral levels the pedicle width was not correlated to the degree of deformity on the coronal or the axial plane, nor with the age, gender or Lenke subtypes. However, the small pedicles of the T3 and T4 on the right side were correlated with the Cobb angle of the minor compensatory curve among patients with Lenke type 1 curve but not among patients with Lenke type 5 curve. The study also showed that patients with Lenke type 1 curve exhibit smaller pedicle regardless of the age, i.e. even among patients older than 15 years.
References
Suk SI, Kim WJ, Kim JH, Lee SM (1999) Restoration of thoracic kyphosis in the hypokyphotic spine: a comparison between multiple-hook and segmental pedicle screw fixation in adolescent idiopathic scoliosis. J Spinal Disord 12:489–495
Suk SI, Lee CK, Kim WJ, Chung YJ, Park YB (1995) Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine (Phila Pa 1976) 20:1399–1405
Liljenqvist UR, Halm HF, Link TM (1997) Pedicle screw instrumentation of the thoracic spine in idiopathic scoliosis. Spine (Phila Pa 1976) 22:2239–2245
Liljenqvist U, Hackenberg L, Link T, Halm H (2001) Pullout strength of pedicle screws versus pedicle and laminar hooks in the thoracic spine. Acta Orthop Belg 67:157–163
Di Silvestre M, Parisini P, Lolli F, Bakaloudis G (2007) Complications of thoracic pedicle screws in scoliosis treatment. Spine 32:1655–1661
Abul-Kasim K, Ohlin A, Strombeck A, Maly P, Sundgren PC (2010) Radiological and clinical outcome of screw placement in adolescent idiopathic scoliosis: evaluation with low-dose computed tomography. Eur Spine J 19:96–104
Halm H, Liljeqvist U, Link T, Jerosch J, Winkelmann W (1996) Computerized tomography monitoring of the position of pedicle screws in scoliosis surgery. Z Orthop Ihre Grenzgeb 134:492–497
Wegener B, Birkenmaier C, Fottner A, Jansson V, Dürr HR (2008) Delayed perforation of the aorta by a thoracic pedicle screw. Eur Spine J Suppl 2:S351–S354
Kakkos SK, Shepard AD (2008) Delayed presentation of aortic injury by pedicle screws: report of two cases and review of the literature. J Vasc Surg 47:1074–1082
Vaccaro AR, Rizzolo SJ, Balderston RA, Allardyce TJ, Garfin S, Dolinskas C, An HS (1995) Placement of pedicle screws in the thoracic spine. Part II: an anatomical and radiographic assessment. J Bone Joint Surg Am 77:1200–1206
Vanichkachorn JS, Vaccaro AR, Cohen MJ, Cotler JM (1997) Potential large vessel injury during thoracolumbar pedicle screw removal. A case report. Spine 22:110–113
Abul-Kasim K, Overgaard A, Maly P, Ohlin A, Gunnarsson M, Sundgren PC (2009) Low-dose helical computed tomography (CT) in the perioperative workup of adolescent idiopathic scoliosis. Eur Radiol 19:610–618
Parent S, Labelle H, Skalli W, de Guise J (2004) Thoracic pedicle morphometry in vertebrae from scoliotic spines. Spine 29:239–248
Kim JH, Choi GM, Chang IB, Ahn SK, Song JH, Choi HC (2009) Pedicular and extrapedicular morphometric analysis in the Korean population: computed tomographic assessment relevance to pedicle and extrapedicle screw fixation in the thoracic spine. J Korean Neurosurg Soc 46:181–188
Christodoulou AG, Apostolou T, Ploumis A, Terzidis I, Hantzokos I, Pournaras J (2005) Pedicle dimensions of the thoracic and lumbar vertebrae in the Greek population. Clin Anat 18:404–408
Chan CY, Kwan MK, Saw LB (2011) Thoracic pedicle screw insertion in Asian cadaveric specimen: does radiological pedicle profile affect outcome? Surg Radiol Anat 33:19–25
Liljenqvist UR, Link TM, Halm HF (2000) Morphometric analysis of thoracic and lumbar vertebrae in idiopathic scoliosis. Spine 25:1247–1253
Liljenqvist UR, Allkemper T, Hackenberg L, Link TM, Steinbeck J, Halm HF (2002) Analysis of vertebral morphology in idiopathic scoliosis with use of magnetic resonance imaging and multiplanar reconstruction. J Bone Joint Surg Am 84-A:359–368
Upendra B, Meena D, Kandwal P, Ahmed A, Chowdhury B, Jayaswal A (2010) Pedicle morphometry in patients with adolescent idiopathic scoliosis. Indian J Orthop 44:169–176
O’Brien MF, Lenke LG, Mardjetko S, Lowe TG, Kong Y, Eck K, Smith D (2000) Pedicle morphology in thoracic adolescent idiopathic scoliosis: is pedicle fixation an anatomically viable technique? Spine 25:2285–2293
Reichle E, Morlock M, Sellenschloh K, Eggers C (2002) Definition of pedicle malposition. Primary stability and loosening characteristics of pedicle screws in relation to position: spongious anchoring, cortical anchoring, perforation and malposition. Orthopade 31:402–405
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abul-Kasim, K., Ohlin, A. Patients with adolescent idiopathic scoliosis of Lenke type-1 curve exhibit specific pedicle width pattern. Eur Spine J 21, 57–63 (2012). https://doi.org/10.1007/s00586-011-2055-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-011-2055-4