
Abstract
As the average life expectancy of the population increases, surgical decompression of the lumbar spine is being performed with increasing frequency. It now constitutes the most common type of lumbar spinal surgery in older patients. The present prospective study examined the 5-year outcome of lumbar decompression surgery without fusion. The group comprised 159 patients undergoing decompression for degenerative spinal disorders who had been participants in a randomised controlled trial of post-operative rehabilitation that had shown no between-group differences at 2 years. Leg pain and back pain intensity (0–10 graphic rating scale), self-rated disability (Roland Morris), global outcome of surgery (5-point Likert scale) and re-operation rates were assessed 5 years post-operatively. Ten patients had died before the 5-year follow-up. Of the remaining 149 patients, 143 returned a 5-year follow-up (FU) questionnaire (effective return rate excluding deaths, 96%). Their mean age was 64 (SD 11) years and 92/143 (64%) were men. In the 5-year follow-up period, 34/143 patients (24%) underwent re-operation (17 further decompressions, 17 fusions and 1 intradural drainage/debridement). In patients who were not re-operated, leg pain decreased significantly (p < 0.05) from before surgery to 2 months FU, after which there was no significant change up to 5 years. Low back pain also decreased significantly by 2 months FU, but then showed a slight, but significant (p < 0.05), gradual increase of <1 point by 5-year FU. Disability decreased significantly from pre-operative to 2 months FU and showed a further significant decrease at 5 months FU. Thereafter, it remained stable up to the 5-year FU. Pain and disability scores recorded after 5 years showed a significant correlation with those at earlier follow-ups (r = 0.53–0.82; p < 0.05). Patients who were re-operated at some stage over the 5-year period showed significantly worse final outcomes for leg pain and disability (p < 0.05). In conclusion, pain and disability showed minimal change in the 5-year period after surgery, but the re-operation rate was relatively high. Re-operation resulted in worse final outcomes in terms of leg pain and disability. At the 5-year follow-up, the “average” patient experienced frequent, but relatively low levels of, pain and moderate disability. This knowledge on the long-term outcome should be incorporated into the pre-operative patient information process.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The average life expectancy of the population is steadily increasing, and best estimates indicate that this will be accompanied by a marked increase in the incidence of degenerative disorders seen in clinical practice [7, 38]. Degenerative disorders of the lumbar spine are often characterised by a compression of the neural elements, resulting in radicular pain and neurogenic claudication, weakness, numbness/tingling and (often) pain in the lower back or buttocks [13, 37]. These complaints not only cause a great deal of discomfort, but also marked restrictions in mobility and function. Together with the inevitable age-associated decline in musculoskeletal function [6, 17], this results in impairment in the patient’s ability to perform activities of daily living and a threat to his/her independence. Since the symptoms are largely due to mechanical (structural) obstruction [39], in all but the most moderate of cases the problem is best treated surgically, with decompression of the affected segment(s) [3, 4, 41].
Long-term outcome studies are essential for all surgical procedures to ascertain whether results deteriorate (or improve) in the long-term and, if so, to identify factors that might influence such change over time. As far as decompression surgery is concerned, the literature reports a general decrease of about 10–20% in the proportion of good outcomes over time, from around 67–88% successes in the initial year after surgery to approximately 52–70% after 5–8 years [4, 19, 21, 33, 36]. Katz et al. [22] reported that after an average 8 years follow-up 33% of patients had severe back pain, 53% were unable to walk two blocks, and 25% were not satisfied with the results of surgery; 23% of them had undergone re-operation. The severity of the spine-related symptoms was a stronger correlate of physical functional status at the time of follow-up than age or non-spinal comorbid conditions. Similar outcomes after 4–12 years were reported by others [4, 8, 21]. These are not particularly impressive long-term results.
One of the problems confronting patients with such spinal disorders is that although decompression surgery addresses the immediate mechanical obstruction, it cannot halt the ongoing degenerative process. Degenerative changes of the spine are often accompanied by instability of the affected motion segment [12, 42] and this, coupled with any iatrogenic instability as a result of the decompression procedure itself, may lead to impaired mechanical integrity of the spine and the recurrence of symptoms [20, 32]. Recent years have seen a trend towards the use of “less destructive” techniques in lumbar spine decompression, in an attempt to avoid the (potential) instability associated with extensive bony resection [9]. However, the long-term impact on symptoms, function and re-operation rates has not been studied extensively.
The aim of the present study was to investigate the 5-year outcome of decompression without fusion in a large group of patients who had participated in a randomised controlled trial (RCT) comparing different post-operative programmes of rehabilitation (self-management versus two different types of active physiotherapy) [25]. Consistent with the findings of a comparable study of structured rehabilitation in a similar patient group [1], our 2-year follow-up results suggested no notable benefits of physiotherapy compared with self-management [25]. As such, for the purposes of the present investigation, the patients were considered as one group.
Methods
Study admission criteria
The inclusion criteria for the study were: age over 45 years; diagnosis of degenerative spinal disease with compression of the neural elements [in association with either hard tissue (osteophytes, calcification, etc.) or soft tissue (herniated disc material)] as ascertained from the medical history, clinical examination, conventional radiography and MRI/CT of the lumbar spine, with an indication for decompression surgery without fusion (if fusion was subsequently deemed necessary, intraoperatively, the patient was excluded from further analysis); failed conservative therapy; willingness to comply with any programme to which randomly assigned (for the original RCT), attendance for all necessary follow-ups and completion of postal questionnaires; a good understanding of written and spoken German.
The exclusion criteria were: previous spinal fusion (although other spinal surgery carried out more than 6 months previously was acceptable); disorders preventing active rehabilitation.
Recruitment of patients
Patients were recruited into the trial from the authors’ hospital, a non-profit making (foundation) orthopaedic clinic. The hospital operation list for the forthcoming 2 months was examined on a weekly basis, and consecutive patients who appeared to satisfy the main admission criteria were sent a letter inviting them to participate, along with an information sheet about the study and a questionnaire booklet (see later). All patients were contacted by phone a week later to enquire about their interest in participating, to check the inclusion/exclusion criteria, and to address any queries in connection with the study. Those who agreed to participate were invited to attend the research department on the day of admission to clarify any remaining issues and sign the informed consent form.
The study was approved by the local university ethics committee.
Surgical and post-operative procedures
Four experienced surgeons operated on the patients. Decompression surgery was carried out using a minimally destructive approach. Briefly, using a posterior midline approach to the laminae, the spinal canal was entered by removal of the ligamentum flavum. Undercutting laminotomy of the caudal and rostral laminae and, where necessary, partial medial facetectomy and removal of disc fragments were performed. Patients were allowed to leave bed the day after surgery. To promote wound healing, no specific treatment or rehabilitation was carried out in the first 6–8 weeks, but the patients were encouraged to walk and move around as normal. Between 2 and 5 months post-operatively, the patients completed a rehabilitation programme comprising either self-management (patients were simply instructed to “keep active”), physiotherapeutic “spine segmental stabilisation exercises” or mixed physiotherapy techniques. The results up to 2 years, indicating no significant between-group differences, have already been published [25]. Examination of the data at 5 years confirmed no significant benefit of physiotherapy compared with self-management, supporting an analysis of all patients together in the present report.
Administration of the outcome questionnaires
Questionnaires were completed before surgery, and at 2 months, 5 months, 1 year, 2 years and 5 years after surgery. The patients filled in the questionnaires at home, to achieve consistent conditions for completion, and returned them by mail. Questionnaires were always checked immediately and patients were requested to complete any missing information. Non-responders during follow-up were contacted by study personnel not involved in the patients’ care until the questionnaire was returned or the patient explicitly stated that no questionnaire would be returned.
Questionnaires
The questionnaire variables enquired about before surgery and at follow-up are shown in Table 1.
For all patients, re-operations (co-interventions) were enquired about in the follow-up questionnaires up to 5 years post-operatively and also checked in the hospital information system (or by communication with the patient). At the longer-term follow-ups, in addition to completing the serial outcome instruments, patients rated the global effectiveness of the treatment they had received (“How much did the operation and post-operative rehabilitation help?”) on a 5-point Likert Scale; responses were then dichotomised into “good” (helped a lot, helped) and “poor” (helped only little, did not help, made things worse) [30].
Statistics
As most of the continuous variables under investigation were approximately normally distributed, parametric statistics were employed for the analyses. Changes in continuous variables were assessed using analysis of variance with repeated measures (time of assessment). Independent t tests were used to examine differences in 5-year outcome scores between those who did and those who did not undergo re-operation in the 5-year period. Relationships between variables were analysed using Pearson coefficients (parametric data) or Spearman rank correlation coefficients with correction for ties (non-parametric).
Statistical significance was accepted at the p < 0.05 level.
Results
Study sample
A total of 159 patients were included in the original trial [25]. Ten had died by the 5-year follow-up. Of those still alive, 143/149 (96%) returned a 5-year questionnaire and these comprised the group under study in the present investigation. Their mean ± SD age was 64 ± 11 years and 92/143 (64%) were men.
Re-operation rate
By the time of the 5-year follow-up, 34/143 patients (24%) had undergone re-operation, at an average of 29.1 ± 20.9 months (range 0.3–59.6 months) after the primary surgery (Table 2). In 30/34 (88%) re-operations, surgery involved the same segment as in the initial surgery; in 2 (6%) cases it involved the adjacent segment, and in 2 (6%) cases, a different segment. 8/143 (5.6%) underwent a third operation.
Outcome in patients with no further surgery up to 5 years post-operatively
The changes in each of the outcome scores over time for the group that did not undergo further surgery are shown in Fig. 1.

a–d Changes in (a) leg pain, (b) low back pain, (c) Roland Morris disability and (d) general health throughout the course of the study, up to 5-years’ follow-up in patients who did not undergo any further surgery
Leg pain intensity
From pre-operative to 2 months post-operative, there was a significant reduction in mean leg pain of 3.6 ± 2.5 points (p < 0.0001), after which there was no significant further change up to 5 years follow-up (Fig. 1a).
Back pain intensity
The mean score for back pain intensity showed a significant reduction of 2.2 ± 2.5 points from before surgery to the first follow-up at 2 months (p < 0.0001) and a small, statistically significant (p = 0.02), but clinically non-relevant, increase of 0.5 ± 2.1 points from 2 months to 5 years post-operatively (Fig. 1b).
Roland Morris disability score
There was a significant decrease of 2.7 ± 5.2 points in the mean Roland Morris (RM) score from before surgery to 2 months post-operatively (p < 0.0001) and a further decrease of 2.5 ± 3.6 points up to 5 months post-operatively (p < 0.0001) (Fig. 1c). After this, no further changes were seen up to 5 years post-operatively.
General health
The general health score increased slightly, but significantly, by 0.7 ± 2.5 points from pre-operative to 2 months post-operative (p = 0.006) and then showed no further change up to 5 years (Fig. 1d).
For each of the above scores, there were highly significant correlations between the scores at the final follow-up after 5 years and each of the previous follow-ups (Table 3).
Frequency of back/leg trouble
Pre-operatively, the frequency of back/leg trouble was 1%, never; 7%, occasional; 29%, often; and 63%, constant. Two months post-operatively, the frequency decreased markedly (p < 0.0001) to 10%, never; 48%, occasional; 34%, often; and 8%, constant. After 5 years, there were somewhat more patients in the two “extreme” categories (never and constant): 25%, never; 37%, occasional; 18%, often; and 20%, constant. There was a significant correlation between the responses at 2 months and 5 years follow-up (ρ = 0.39, p < 0.0001), with the frequency of back/leg trouble differing by no more than one category (i.e. was just one category higher or lower) in 86% patients.
Use of pain medication
Pre-operatively, the frequency of pain medication use was 23%, never; 31%, occasional; 17%, often; and 29%, constant. Medication use declined significantly after surgery (p < 0.0001) and was similar at both the short-term and long-term follow-ups: 2 months post-operatively, 66%, never; 18% occasional, 10% often, and 6% constant use; after 5-year, 60% never, 22% occasional, 9%, often; and 9%, constant.
The responses at the two time points showed a moderate, significant correlation (ρ = 0.49, p < 0.0001), and in a high proportion of patients (87%), medication use did not vary by more than one category between 2 months and 5 years.
Global outcome of treatment
When the global outcome measured on the 5-point Likert scale was dichotomised into “good” and “poor” (see “Methods”), the proportion of patients reporting a “good” global outcome reduced from 86.1% at 2 months to 78.7% at 5 years follow-up (p = 0.057). 87.0% patients gave exactly the same global outcome rating (i.e. either good or poor) at both 2 months and 5 years; 2.8% gave a better rating at 5 years (poor became good), and 10.2% a worse rating (good became poor).
Final outcomes in patients who underwent re-operation during the 5-year follow-up
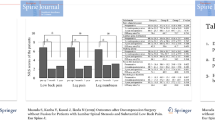
Compared with the patients who were not re-operated, the patients who had undergone further surgery during the course of the study showed significantly less improvement in Roland Morris Disability and leg pain scores from baseline to the 5-year follow-up [reduction in Roland Morris score: no further surgery, 5.6 ± 6.2 points vs. further surgery, 1.8 ± 4.8 points (p = 0.0012); reduction in leg pain: no further surgery, 3.6 ± 2.9 points vs. further surgery, 2.2 ± 3.6 points (p = 0.018)] (Fig. 2). There were similar tendencies in relation to the degree of improvement in back pain and general health, but they failed to reach significance (p > 0.05).

(a) Leg pain and (b) Roland Morris disability scores before surgery and at 5 years follow-up in patients who did not undergo re-operation (“no reop”; black bars) and those who did undergo further surgery (“re-op”; grey bars) during the course of the study. For both outcomes, there was a significant difference between the groups (no re-op vs. re-op) for the reduction in score after 5 years (p < 0.05)
Good global outcomes were reported by 27/34 (79%) of the group after 2 months, and just 22/34 (64.7%) at the follow-up 5 years after the first surgery.
Discussion
Main findings and methodological considerations/limitations
The present study sought to quantify the long-term outcome of lumbar spinal decompression surgery in patients with degenerative spinal disorders. The main findings were that the mean levels of pain and disability reported at 2 months post-operatively remained fairly stable up to 5 years. However, almost one in four patients required further surgery on the lumbar spine in the 5-year study period and those that were re-operated had significantly worse final outcomes, in terms of leg pain and disability, than did those who had no further surgery.
The group under study did not include all eligible patients undergoing decompression within our spine unit, but instead comprised patients who had offered their voluntary participation in a RCT [25]. Nonetheless, adequate external validity of the findings was suggested by the fact that the medical history, clinical status and treatment outcomes of the study patients were broadly comparable to those of the typical patient undergoing decompression surgery described in the literature [10, 31] and of consecutive patients from our own centre [23], documented systematically in connection with the Spine Tango Spine Registry of the Spine Society of Europe [34]. The only exception to this was that the study attracted a predominance of male volunteers, with slightly lower baseline symptoms than the “typical patient”. This type of gender and symptom severity bias has frequently been reported for trials in other areas of medicine [5, 16, 24]. Whilst the reasons for it are not clear, they include suggestions that men and women may react differently to presentations of risk–benefit analysis or that women may feel less able to release themselves from their homemaking duties to participate in trials [18]. Studies involving elderly patients are notoriously difficult to carry out, and the present study was no exception. The repeat surgery and deaths during follow-up were just some of the problems that beset the current investigation. Nonetheless, a highly respectable follow-up rate (96% of those still alive) was still achieved up to 5 years post-surgery.
In any studies of surgical outcome, deciding on the most appropriate method of dealing (in the analysis) with patients who undergo re-operation is never straightforward. In the present study, when examining the course of change in the main outcomes, we decided to exclude the re-operated patients, on the basis that if their (presumably more severe) symptoms prior to the second intervention had been remedied by re-operation, they could have falsely elevated the outlook after 5 years in the whole group. In practice, however, when examined as a separate group, even after re-operation they displayed less improvement on their pre-operative status compared with the patients who were not re-operated (see later). We could not depict the whole course of change over the 5 years in the re-operated group, because the precise time of re-intervention differed for the individual patients, rendering it impossible to calculate meaningful point estimates of the group’s level of pain or disability at the fixed follow-ups. Hence, we elected to present only their results for the final follow-up, as compared with baseline values (i.e. before the first index operation). Interestingly, a secondary analysis including all patients together (re-operated and not re-operated; actual results not shown) did not substantially alter the overall course of change shown in Fig. 1.
Consistency of changes over time
On an individual basis, the outcomes recorded 5 years post-operatively showed a relatively high, significant correlation with those recorded at the earlier follow-ups. In other words, the early outcome was a reasonably good predictor of the longer-term outcome. This phenomenon has been reported before by ourselves [26, 29] and other groups [15, 31] for patients with degenerative disorders followed up for up to 2 years, and by Amundsen et al. [3] for patients followed up even longer (10 years). Since surgery for degenerative diseases typically serves a “mechanical” purpose, aiming to relieve pain by removing a physical obstruction (e.g. by decompression in the case of spinal stenosis), as far as the main symptoms are concerned, the success (or otherwise) of the operation should be evident relatively early [29]. It may be expected that a somewhat longer time would be required for the final improvements in disability or function to manifest themselves, but clearly even here the early results are able to herald the longer-term outcome. This suggests that we should pay close attention to the early failures and not simply expect time to heal. Timely and evidence-based re-interventions (either conservative or operative) should be implemented for unimproved patients in an attempt to forestall the development of chronic disability and its accompanying psychological sequelae.
Long-term outcome after decompression
In keeping with other reports in the literature, the proportion of overall “good” outcomes recorded in the present study declined slightly over the 5-year follow-up period, though to a lesser extent compared with earlier studies [4, 19, 21, 22, 33, 36] and still remaining fairly good after 5 years (79% with a “good” global outcome after 5 years). It is not possible to ascertain whether the less marked deterioration over time in the present study was the result of the modern-day, less “destructive” surgical techniques used or was due to unidentified differences between studies in the patient populations examined.
In view of the observed changes over time in the serially measured outcomes (Fig. 1), the slightly poorer global outcome ratings at 5 years may have been the result of the slight, but significant, increases in pain (especially LBP) over time, and the fact that almost 40% of the patients declared that they had back trouble either “often” or “constantly”. Since decompressive surgery serves only to eliminate the immediate obstruction and does not reverse or even halt the degenerative process per se, it is only to be expected that the degenerative changes will progress with time. These should not necessarily be considered as “failure” in relation to the index procedure, though they obviously need to be acknowledged in explaining the likely long-term outcome to the patient.
The need for re-operation was almost certainly a factor that rendered the global outcome ratings as less positive over time in the group that underwent further surgery. The re-operation rate in the present study was 24%, which was slightly higher than the 5-year re-operation rate reported by Jonsson et al. (18%; [21]) and comparable to the 8-year repeat surgery rate reported by Katz et al. (23%; [22]). Analogous to these other reports, the majority of repeat surgeries in the present study also occurred at the same level as the primary surgery and involved either further decompression or fusion of the segment. The average time of re-operation after the primary surgery was approximately two and a half years, which would certainly be commensurate with a gradual recurrence of further symptoms as a result of ongoing degenerative changes in the spine. However, the range of values was quite wide and fairly evenly spread across the 5-year follow-up period and, on an individual basis (results not shown), whilst some patients had a clear increase in symptoms in the period preceding their re-operation, others appeared to have simply waited with a relatively poor result from the outset. Either way, it was clear that re-operation—whether due to recurrence of symptoms or as an attempted remedy for an initially poor result—generally resulted in a less good outcome in the end. This concurs with previous reports that the probability of a good surgical outcome generally decreases with each successive surgery [40].
It was interesting to note that, at the final follow-up in the present study, 5 years after surgery, patients experienced (on average) moderate levels of disability in everyday activities, not dissimilar to the levels recorded using the same instruments in patients with non-specific chronic LBP [28]. Similar values have been reported in other long-term investigations of patients after decompression surgery [22, 31]. Hence, this may well represent the level of symptoms and function that these patients finally have to learn to cope with, if there is no clear indication for further surgery. The exploitation of this valuable information for the purposes of patient education in relation to the likely outcome of surgery should at least lead to better informed and potentially more satisfied patients in the long run [27], whilst pain management programmes, of the type commonly used in patients with non-specific chronic LBP [2], might be considered for those with the most severe, persistent problems.
References
Aalto T, Leinonen V, Herno A, Kroger H, Turunen V, Savolainen S, Airaksinen O (2009) Postoperative rehabilitation after spinal stenosis surgery—no effect on outcome in 2-year follow-up. International Society for the Study of the Lumbar Spine, Miami, FL
Adams N, Poole H, Richardson C (2006) Psychological approaches to chronic pain management: part 1. J Clin Nurs 15:290–300
Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleas F (2000) Lumbar spinal stenosis: conservative or surgical management?: A prospective 10-year study. Spine 25:1424–1435
Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine Lumbar Spine Study. Spine 30:936–943
Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, Dieppe P (2005) The causes and effects of socio-demographic exclusions from clinical trials. Health Technol Assess 9:iii–iv, ix–x, 1–152
Chung SG, Van Rey EM, Bai Z, Rogers MW, Roth EJ, Zhang LQ (2005) Aging-related neuromuscular changes characterized by tendon reflex system properties. Arch Phys Med Rehabil 86:318–327
Ciol MA, Deyo RA, Howell E, Kreif S (1996) An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr Soc 44:285–290
Cornefjord M, Byrod G, Brisby H, Rydevik B (2000) A long-term (4- to 12-year) follow-up study of surgical treatment of lumbar spinal stenosis. Eur Spine J 9:563–570
Detwiler PW, Spetzler CB, Taylor SB, Crawford NR, Porter RW, Sonntag VK (2003) Biomechanical comparison of facet-sparing laminectomy and Christmas tree laminectomy. J Neurosurg 99:214–220
Dullerud R, Amundsen T, Lie H, Juel NG, Magnaes B (1995) CT-diskography, diskomanometry and MR imaging as predictors of the outcome of lumbar percutaneous automated nucleotomy. Acta Radiol 36:613–619
Exner V, Keel P (2000) Erfassung der Behinderung bei Patienten mit chronischen Rückenschmerzen. Schmerz 14:392–400
Fujiwara A, Tamai K, An HS, Kurihashi T, Lim TH, Yoshida H, Saotome K (2000) The relationship between disc degeneration, facet joint osteoarthritis, and stability of the degenerative lumbar spine. J Spinal Disord 13:444–450
Goh KJ, Khalifa W, Anslow P, Cadoux-Hudson T, Donaghy M (2004) The clinical syndrome associated with lumbar spinal stenosis. Eur Neurol 52:242–249
Haefeli M, Elfering A (2006) Pain assessment. Eur Spine J 15(Suppl 1):S17–S24
Hakkinen A, Ylinen J, Kautiainen H, Airaksinen O, Herno A, Kiviranta I (2003) Does the outcome 2 months after lumbar disc surgery predict the outcome 12 months later? Disabil Rehabil 25:968–972
Heiat A, Gross CP, Krumholz HM (2002) Representation of the elderly, women, and minorities in heart failure clinical trials. Arch Intern Med 162:1682–1688
Hopp JF (1993) Effects of age and resistance training on skeletal muscle: a review. Phys Ther 73:361–373
Jagsi R, Motomura AR, Amarnath S, Jankovic A, Sheets N, Ubel PA (2009) Under-representation of women in high-impact published clinical cancer research. Cancer 115:3293–3301
Javid MJ, Hadar EJ (1998) Long-term follow-up review of patients who underwent laminectomy for lumbar stenosis: a prospective study. J Neurosurg 89:1–7
Johnsson KE, Redlund-Johnell I, Uden A, Willner S (1989) Preoperative and postoperative instability in lumbar spinal stenosis. Spine 14:591–593
Jonsson B, Annertz M, Sjoberg C, Stromqvist B (1997) A prospective and consecutive study of surgically treated lumbar spinal stenosis Part II: five-year follow-up by an independent observer. Spine 22:2938–2944
Katz JN, Lipson SJ, Chang LC, Levine SA, Fossel AH, Liang MH (1996) Seven- to 10-year outcome of decompressive surgery for degenerative lumbar spinal stenosis. Spine 21:92–98
Kleinstuck FS, Grob D, Lattig F, Bartanusz V, Porchet F, Jeszenszky D, O’Riordan D, Mannion AF (2009) The influence of preoperative back pain on the outcome of lumbar decompression surgery. Spine 34:1198–1203
Klosky JL, Tyc VL, Lawford J, Ashford J, Lensing S, Buscemi J (2009) Predictors of non-participation in a randomized intervention trial to reduce environmental tobacco smoke (ETS) exposure in pediatric cancer patients. Pediatr Blood Cancer 52:644–649
Mannion AF, Denzler R, Dvorak J, Muntener M, Grob D (2007) A randomised controlled trial of post-operative rehabilitation after surgical decompression of the lumbar spine. Eur Spine J 16:1101–1117
Mannion AF, Elfering A (2006) Predictors of surgical outcome and their assessment. Eur Spine J 15(Suppl 1):S93–S108
Mannion AF, Junge A, Elfering A, Dvorak J, Porchet F, Grob D (2009) Great expectations: really the novel predictor of outcome after spinal surgery? Spine 34:1590–1599
Mannion AF, Müntener M, Taimela S, Dvorak J (1999) A randomised clinical trial of three active therapies for chronic low back pain. Spine 24:2435–2448
Mannion AF, Porchet F, Kleinstück F, Lattig F, Jeszenszky D, Bartanusz V, Dvorak J, Grob D (2009) The quality of spine surgery from the patient’s perspective: Part 1. The Core Outcome Measures Index (COMI) in clinical practice. Eur Spine J 18:367–373
Mannion AF, Porchet F, Kleinstuck FS, Lattig F, Jeszenszky D, Bartanusz V, Dvorak J, Grob D (2009) The quality of spine surgery from the patient’s perspective: Part 2. Minimal clinically important difference for improvement and deterioration as measured with the Core Outcome Measures Index. Eur Spine J 18:374–379
McGregor AH, Hughes SPF (2002) The evaluation of the surgical management of nerve root compression in patients with low back pain. Part 1: The assessment of outcome. Spine 27:1465–1470
Postacchini F, Cinotti G (1992) Bone regrowth after surgical decompression for lumbar spinal stenosis. J Bone Joint Surg Br 74:862–869
Postacchini F, Cinotti G, Gumina S, Perugia D (1993) Long-term results of surgery in lumbar stenosis. 8-year review of 64 patients. Acta Orthop Scand Suppl 251:78–80
Roder C, Chavanne A, Mannion AF, Grob D, Aebi M, El-Kerdi A (2005) SSE Spine Tango–content, workflow, set-up. Eur Spine J 14:920–924. http://www.eurospine.org, Spine Tango
Roland M, Morris R (1983) A study of the natural history of back pain. Part 1:development of a reliable and sensitive measure of disability in low-back pain. Spine 8:141–144
Scholz M, Firsching R, Lanksch WR (1998) Long-term follow up in lumbar spinal stenosis. Spinal Cord 36:200–204
Spengler DM (1987) Degenerative stenosis of the lumbar spine (current concepts review). J Bone Joint Surg 69A:305–308
Szpalski M, Gunzburg R, Melot C, Aebi M (2003) The aging of the population: a growing concern for spine care in the twenty-first century. Eur Spine J 12(Suppl 2):S81–S83
Truumees E (2005) Spinal stenosis: pathophysiology, clinical and radiologic classification. Instr Course Lect 54:287–302
Waddell G, Kummel EG, Lotto WN, Graham JD, Hall H, McCulloch JA (1979) Failed lumbar disc surgery and repeat surgery following industrial injuries. J Bone Joint Surg Am 61:201–207
Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, Herkowitz H, Cammisa F, Albert T, Boden SD, Hilibrand A, Goldberg H, Berven S, An H (2008) Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 358:794–810
Zhao F, Pollintine P, Hole BD, Dolan P, Adams MA (2005) Discogenic origins of spinal instability. Spine 30:2621–2630
Acknowledgements
This study was supported by the Swiss National Science Foundation (Grant no. 32-57123.99) and the Schulthess Klinik Research Fund. We are especially grateful to Renata Heusser, Gordana Balaban and Katrin Knecht for their valuable assistance in managing the study and collecting the data. We also thank Astrid Junge for her help in planning the questionnaire battery.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mannion, A.F., Denzler, R., Dvorak, J. et al. Five-year outcome of surgical decompression of the lumbar spine without fusion. Eur Spine J 19, 1883–1891 (2010). https://doi.org/10.1007/s00586-010-1535-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1535-2