
Abstract
The objective was to determine whether any measurable changes in sensory responses, kinesthetic sense, cervical motion, and psychological features were related to established fatty infiltration values in the cervical extensor musculature in subjects with persistent whiplash. It is unknown if fatty infiltrate is related to any signs or symptoms. Data on motor function, Quantitative Sensory Testing, psychological and general well-being, and pain and disability were collected from 79 female subjects with chronic whiplash. Total fat values were created for all subjects by averaging the muscle fat indices by muscle, level, and side from our MRI dataset of all the cervical extensor muscles. Results of this study indicate the presence of altered physical, kinesthetic, sensory, and psychological features in this cohort of patients with chronic whiplash. Combined factors of sensory, physical, kinesthetic, and psychological features all contributed to a small extent in explaining the varying levels of fatty infiltrate, with cold pain thresholds having the most influence (r 2 = 0.28; P = 0.02). Identifying and relating quantifiable muscular alterations to clinical measures in the chronic state, underpin some clinical hypotheses for possible pathophysiological processes in this group with a chronic and recalcitrant whiplash disorder. Future research investigations aimed at accurate identification, sub-classification, prediction, and management of patients with acute and chronic whiplash is warranted and underway.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The development of persistent pain and disability following whiplash injury is not uncommon and often results in sizeable clinical, social, and economic costs. People with persistent whiplash associated disorders (WAD) may present with a myriad of symptoms including pain, dizziness/unsteadiness, physical, and psychological deficits [50, 51, 54, 56, 61]. The variability of these symptoms underpins the difficulty in gathering accurate information related to the nosologic features of the chronic disorder. There continues to be long-standing concern about whether persistent pain is attributable to defined physical pathology or to other underlying outcome determinants such as culture [16] and/or psychological factors [25, 39].
The situation would be assisted if there were quantitative radiological markers of the disorder but markers of salient structural lesions in WAD remain inconclusive [26, 38, 42, 43, 47]. MRI markers of fatty infiltration have been reported in the cervical extensor musculature in females with chronic WAD [14]. Such fatty infiltrate was not present in those without history of neck pain and notably, was not identified in patients with chronic, non-traumatic neck pain [15]. Therefore, fatty infiltrate could be a quantitative radiological marker in patients with chronic WAD.
The first question to be answered is whether MRI markers of fatty infiltrate in the cervical extensors are aligned with any symptoms and/or physical and psychological manifestations in the chronic state. Previous research [14] has shown that fatty infiltrate occurs in widespread fashion across muscle and segmental level (C0–C7) and it is independent of age, Body Mass Index, duration, compensation, and self-reported levels of pain and disability. The widespread findings of fatty infiltrate could suggest generic signs of muscle degeneration. However, on the contrary, higher muscle fat indices in the subjects with chronic WAD were present in the sub-occipital muscles and the deep segmental multifidii, which may point to more specific pathophysiological processes. Two other studies have provided preliminary evidence of an association between sub-occipital muscle degeneration and persistent pain [1] and balance disturbance [37]. A higher incidence of dizziness and unsteadiness has been reported by patients with chronic WAD, suggesting that such disturbances were the result of altered somatosensory input [61]. Hayashi et al. [21] demonstrated abnormal MRI signal enhancement in the segmental musculature of patients with confirmed nerve root avulsion injury. They hypothesized that signal enhancement in the multifidus was an indirect sign of nerve root avulsion. Whilst nerve root avulsion is not likely the cause of chronic pain in whiplash, it is possible that a cause of these muscular changes in patients with chronic WAD could be the result of minor or major nerve injury. Such a condition could contribute to the development of neuropathic pain and align with the features of augmented central pain processing found in some patients with chronic WAD [10, 50].
Psychological disturbances have also been reported in some patients with WAD and it has been suggested that the presence of psychological distress results from ongoing pain and disability [13, 41, 45, 54]. There is no theoretical rationale to suggest that psychological disturbances would result in fatty infiltration, but it is reasonable to expect that fatty infiltration in the cervical extensor musculature could represent a greater injury and therefore higher self-reported pain and concomitant psychological distress.
Due to the compensable environment of whiplash, it is important that more ‘objective’ and quantifiable measures are explored and developed. Thus the aim of this study was to investigate if any relationships existed between fatty infiltrate in the extensor musculature documented in a previous study [14] and any particular symptoms and features documented for this group with chronic WAD. If there were associations, the presence of fat might contribute toward the development of a reliable and valid quantitative radiological measure for the evaluation of patients with chronic WAD.
Patients and methods
A total of 79 subjects with persistent WAD were included provided they experienced persistent pain and disability (3 months to 3 years) resulting from a motor vehicle crash (MVC) and were within the Quebec Task Force Classification category of Grade II [49]. The cohort was restricted to females (18–45 years) as they best represent the predominant population of patients suffering from persistent whiplash related pain and disability [27, 33]. Those with direct trauma to the head and/or loss of consciousness as a result of the MVC were excluded to limit the possibility of a central cause for their symptoms. Volunteers were also excluded if they had been previously involved in one or more MVCs, had treatment for other neck pain disorders in the past 10 years, or had been diagnosed with any nervous system disorder. This project was granted approval by Institutional Medical Research Ethical Committees and all subjects provided written informed consent.
A series of physical measures and questionnaires were taken to gain comprehensive data on subject demographics, neck pain and disability, symptoms of dizziness, physical impairment, psychosocial factors and psychophysical responses to pain. One researcher (JE) performed the physical measures on all subjects. The MRI measures were obtained at a separate radiology center, either that day or the next day.
Self-reported symptoms and disability
Self-reported symptoms and disability were measured in all individuals with a whiplash injury using the Neck Disability Index (NDI) and the Dizziness Handicap Inventory-short form (DHI-sf). The NDI [64] is a 10-item validated questionnaire which has been shown to be of value in quantifying pain and disability related to neck pain and WAD [44]. The DHI-sf is a 13-item questionnaire where a score of 13 represents no handicap and 0 = maximum handicap [57].
Psychological and quality of life measures
The battery of psychological measures included
-
1.
Tampa scale of Kinesphobia (TSK)—a reliable and valid 17-item self report measure of fear of re-injury due to movement (kinesophobia) [9, 30, 65].
-
2.
The General Health Questionnaire—28 (GHQ-28) [20]—a standard measure of emotional distress in a medical setting [19].
-
3.
The Short Form-SF-36 (SF-36) [66]—a measurement of general health and disability. Higher scores represent higher levels of function.
-
4.
The Impact of Events Scale (IES) [23]—a 15-item questionnaire measuring present stress related to a particular event. It has been validated in studies investigating emotional responses to acute trauma [28, 54] and shown to be predictive of poor outcome in the long-term following whiplash [52].
Tests of the sensorimotor system
Two measures were used for the sensorimotor system: total range of movement (ROM) and cervical joint reposition error (JPE). Range of active cervical movement was measured using an electromagnetic motion-tracking device (Fastrak, Polhemus, USA—www.polhemus.com) [11, 62]. The Fastrak system has been used previously to document cervical active range of movements in patients with neck pain disorders [11, 53, 61] and has demonstrated accuracy [40]. Three recordings each were obtained for active ROM in flexion, extension, rotation left and right, lateral flexion left and right. The mean values were combined in order to present a measure of total ROM for analysis.
Cervical JPE was measured according to Revel et al. [46] using previously established methodology [61] with the Fastrak system as described for ROM testing. The subjects’ ability, whilst blindfolded, to perform the repositioning task was measured by obtaining three recordings for each of the different planar movements (rotation left, right and extension). The mean values for each direction were used for analysis.
Psychophysical sensory tests
Pressure Pain Thresholds (PPTs) were measured using a pressure algometer (Somedic AB, Farsta, Sweden). PPTs were measured bilaterally over the left and right articular pillars of C2/3 and C5/6 and at a remote site (tibialis anterior (TA) muscle). This methodology has been previously established [6, 55]. Three recordings were taken at the C2/3, C5/6 and TA sites and were combined and averaged to present one value for PPT_local and PPT_remote, respectively.
Thermal Pain Thresholds (TPTs) (Cold (CPT)/Heat (HPT)) were measured over the cervical spine using the Thermal Sensory Analyzer (Medoc Advanced Medical Systems, Israel). To identify CPTs and HPTs, subjects were instructed to push a hand-held patient-controlled button when the cold or warm sensation first became painful [50]. A method of limits (mean of 3 measures) algorithm was utilized for thermal measurements and used for analysis.
The physical measures were collected in the same order; ROM (flexion, extension, left rotation, right rotation, left lateral flexion, right lateral flexion), JPE (left rotation, right rotation, extension), PPT (left and right articular pillars of C2/3, C5/6 and then left and right TA), TPTs (left and right CPT then left and right HPT).
MRI measures and analysis
The Intra-class correlation coefficients (ICC) for the reliability of the MRI measures of fat within muscle in this population have been previously reported and the measures were shown to have high levels of inter- and intra-rater reliability (ICC of 0.94 and 0.93, respectively) [14].
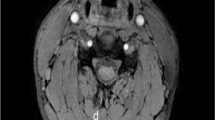
The MRI measure has been previously established [14]. In brief, the analysis consisted of manually tracing defined regions of interest (ROI) over each of the bilateral cervical extensor muscles on the axial T1-weighted images at each vertebral segment (C0-C7). T1 weighted images are very sensitive to the presence of fatty deposition in muscle and as a result, were chosen to quantify fatty infiltration in the cervical extensor musculature. The measure of relative fat within the muscle was created by taking a ratio between the pixel intensities of each muscle to that of a standardized region of intermuscular fat in the cervical spine, the specifics of which are detailed elsewhere [14].
For the purpose of this study, two measures of total average fat within the cervical extensors were used for analyses. Firstly, as fatty infiltrate was widespread in the extensor muscles, a total fat measure (TOTAL_FAT; TF) was developed by combining and averaging the muscle fat indices for the rectus capitis posterior minor, major and the multifidus, semispinialis cervicis, capitis, splenius capitis and upper trapezius musculature bilaterally across all cervical segments (C3-7). Secondly, a total upper fat index measure (TOTAL_UPPER_FAT; TUF) was produced by combining and averaging the muscle fat indices for the rectus capitis posterior minor, major, and the segmental multifidus at C3 bilaterally as these muscles had significantly higher levels of fatty infiltrate when compared to the other more superficial musculature at and below the C3 level [14].
Statistical analysis
Relationships between clinical measures (15 independent variables) and fatty infiltrate data (two dependent variables; TF and TUF) were analyzed with a stepwise backward elimination multivariate regression. Regressors were then tested for significance. On the grounds of a small study sample, the significance level was set at a conservative P < 0.20, a priori.
Results
The mean duration of symptoms for the subjects with WAD was 20.3 ± 9.6 months and 65% were involved in compensation claims at the time of the study. Table 1 presents the demographic details for the subjects with persistent WAD. Table 2 presents the psychophysical data as well as the scores on all questionnaires for subjects with persistent WAD. The fat/muscle indices (mean ± SD (range)) for the TF and TUF values were 0.31 ± 0.04 (0.21–0.40) and 0.41 ± 0.06 (0.29–0.55), respectively.
Prediction of fat in the cervical extensor musculature
The results of the multivariate regression analysis revealed that nine variables (age, scores on the NDI, IES, SF-36, CPT, PPT-local, total ROM, compensation status, and duration of symptoms) contributed to a small extent in explaining the variation in TF among the subjects with whiplash and together accounted for 24% of the variability (Table 3). The results also revealed that nine variables (age, scores on the IES, GHQ-28, TSK, CPT, PPT-local, PPT-remote, JPE, and compensation status) contributed to a small extent in explaining the variation in TUF for the group with WAD and together accounted for 28% of the variability Table 4. Tables 3 and 4 display the direction and magnitude of each variable’s effect on TF and TUF.
Discussion
This study attempted to determine if particular clinical symptoms, physical, and/or psychological features were related to findings of fatty infiltrate in the cervical extensor musculature which might assist in understanding underlying processes in chronic WAD. However, the results of the regression analyses, albeit significant, were marginal and varied. The combined factors of sensory, physical, kinesthetic, and psychological features all contributed to explaining the variation of the levels of fatty infiltrate for both dependent measures (TF—24% of the variance; TUF—28% of the variance). Thus, fatty infiltrate would seem from this study to be a generic sign for a homogenous group with chronic WAD and so likely represents more than one pathophysiological process. However, as these findings of fatty infiltrate were observed in the chronic state, the significance of these muscle changes with respect to outcomes such as pain and disability and recovery rates remains unclear. The participants of this study all showed concomitant sensory (hyperalgesia) and psychological disturbances that characterize and predict those with a complex, non-resolving injury [52]. These disturbances have not shown to feature in subjects with persistent non-traumatic neck disorders [48]. Thus it could be suggested that the fatty muscle changes in chronic WAD, may be associated with non-recovery. Further investigation into whether fatty muscle changes occur uniformly in all whiplash injured people irrespective of recovery or are unique to only those who develop chronic symptoms is required and currently underway.
From a neurobiological standpoint, the factor of CPT held in both regression models (TF (P = 0.1) and TUF (P = 0.02)). Cold hyperalgesia may be due to either alterations in the central nervous systems’ mediation of pain or a result of a peripheral nerve injury [12, 29]. The presence of cold hyperalgesia and other alterations in the central nervous systems’ ability to process pain (e.g., widespread mechanical and pressure pain thresholds (PPT)) have also been identified by others [2, 29, 50]. It is suggested that some of these changes are potentially irreversible [10]. It is noteworthy that PPT_remote, in tandem with CPT, held in the regression model for TUF (P = 0.1). This may align with previous work demonstrating that chronic WAD can result in findings of not just local, but rather widespread abnormal pain processing [2, 10, 52]. However, the direction of the association between PPT_local, TF (P = 0.09) and TUF (P = 0.1) was inverse (e.g., those with higher fat content had higher thresholds) and this is more difficult to explain. Nevertheless, the results of this study might provide some preliminary evidence that the presence of cold and widespread mechanical hyperalgesia in conjunction with the MRI findings of muscular fatty infiltrate in the upper cervical musculature could be reflective of a peripheral nerve injury in the cervical region [8, 18, 21, 35, 36, 63] and could explain the widespread sensory findings in this cohort. The presence of these sensory features in conjunction with the temporal development and magnitude of fatty infiltrate needs to be investigated in a prospective, longitudinal study with a more heterogeneous population to better identify a possible neuropathic [3, 24] element in at least some patients who transition to chronicity.
It is also possible that the fatty alterations in the deep suboccipital and extensor muscles, which are rich in muscle spindle density [4, 5, 34], may account for some of the common functional impairments observed in whiplash, such as kinesthetic deficits [22, 31, 32] and balance loss [17, 60]. Previous studies have shown that subjects with whiplash who complain of dizziness demonstrate greater deficits in cervical JPE, neck influenced eye movement control, and postural stability when compared to those not complaining of these symptoms and when compared to healthy controls [32, 58, 59]. Treleaven et al. [59] determined a relationship between pain levels (NDI) and complaints of dizziness amongst patients with persistent WAD. The present cohort had a mean NDI score of 45.5 and 92% complained of dizziness. This mirrors the NDI scores (46.4) for those subjects who complained of dizziness in the study of Treleaven et al. [59]. However, the findings did not fit a clear picture. The NDI held in the regression model for TF content but not in the model for TUF, which suggests that higher levels of pain and disability influence the fat content in the entire cervical region but not primarily in the upper cervical musculature. Further, the higher fat content in the upper cervical region was inversely related to the JPE deficits, suggesting that any kinesthetic deficits are not related to fatty infiltrate in the upper cervical region. However, caution should be exercised in the interpretation of these results at this time as it may be a factor of power in the study. The global measures combining the muscle: fat profiles may have been too conservative to determine significance. Nevertheless, the contention remains that altered afferent input from the upper cervical musculature may influence kinesthetic functioning in patients with chronic WAD. Larger scale studies involving measures of individual muscles across a more heterogeneous sample of subjects with WAD with varying degrees of kinesthetic deficits is required before more definitive conclusions can be drawn.
Further to the biological mechanisms, the entire cohort was psychologically distressed (GHQ-28) to some degree and this maintained in the regression model for TUF. The group mean data for total GHQ-28 scores (30.5) were well above the previously established cut-off threshold (23/24) [20]. This finding is consistent with previous studies showing elevated levels of psychological distress in subjects with acute and chronic WAD [13, 41, 45, 54]. It has been suggested that the presence of psychological distress is the result of persistent symptoms [13, 41, 45, 54]. Therefore, higher amounts of fat within the cervical muscles may provide a more objective measure to help characterize this narrow group of chronic patients. The WAD subjects were also characterized by the presence of post-traumatic stress symptoms (IES) and this persisted in both regression models. The total IES score for the group was 23.3 indicating an ongoing mild post-traumatic stress reaction [23], which is consistent with the findings from other investigations into patients with acute [13] and chronic WAD [52].
Furthermore, it also should be considered that such psychological distress in patients with chronic whiplash symptoms may result in the patient not moving their neck because of fear of movement. However, the direction of any effect with fear of movement (as measured by the TSK) was inversely proportional to the TUF measure, e.g., those with higher TUF had lower TSK scores. This is not altogether surprising as the role of fear of movement beliefs seems to be a less important factor in individuals with whiplash [52] than in those with other musculoskeletal disorders [65]. Further research involving a more heterogeneous sample of subjects with acute whiplash is needed before definitive conclusions can be drawn regarding any relationships between the factors of psychological distress (fear of movement), pain and disability, and fat within muscle.
Compensation status was included in the model as argument exists whether persistent whiplash symptoms results from physical insults or more to psychological disturbances and higher rates of personal compensation claims [25]. Sixty-five percent (51/79) of the cohort were involved in compensation claims at the time of the study and a direct relationship between compensation status and fatty infiltrate was noted in both regression models. That is, subjects who were seeking compensation had higher amounts of fatty infiltrate in the cervical extensor musculature. The mean NDI score for those seeking compensation was 50.6 and 36.2 for those not seeking compensation. The lower scores for non-compensation seekers are not surprising and generally support the argument that only those with more severe injuries seek personal assistance through compensation [7]. Despite lower pain and disability levels, the NDI scores in non-compensation seekers would still earn them membership into a group with moderate to severe injuries (>30/100) [50] and caution should be exercised in interpreting these preliminary results.
It is recognized that this study represents a narrow sample, e.g., a recalcitrant group with chronic WAD. All had sensory, motor, and psychological deficits and all had varying levels of fatty infiltrate in the cervical extensors. These findings may represent a debilitated state or a pathological process that is yet to be established. Strong conclusions cannot be generated with rejection of the null when power may be small and there is a risk of Type I error with a conservative P value <0.20; however, the standard errors reflect the precision of the estimates. Therefore, these data underpin some clinical hypotheses for possible pathophysiological processes for this chronic group.
Conclusion
Those with persistent pain and disability following whiplash injury present with disturbances in motor, sensory, psychological function and varying levels of fatty infiltrate in their cervical extensor musculature. The presence of fatty infiltrate in the cervical extensor muscles was marginally explained by a composite of sensory, physical, and psychological features in a homogenous group with chronic WAD. It is essential to evaluate the fidelity of the MRI measure for muscular changes in a longitudinal, prospective design involving sub-groups of patients with WAD, to determine how soon following injury these changes occur. In that way, it can be better identified whether or not muscular alterations are unique to only those subjects who transition to chronic pain and disability and whether fatty infiltrate can be more definitively aligned to pathophysiological processes that could influence assessment and management.
References
Andary MT, Hallgren R, Greenman PF et al (1998) Neurogenic atrophy of suboccipital muscles after a cervical injury: a case study. Am J Phys Med Rehabil 77:545–549
Banic B, Petersen-Felix S, Andersen OK et al (2004) Evidence for spinal cord hypersensitivity in chronic pain after whiplash injury and in fibromyalgia. Pain 107:7–15
Bennett G (2006) Can we distinguish between inflammatory and neuropathic pain? Pain Res Manag 11:11–15
Boyd-Clark LC, Briggs CA, Galea MP (2001) Comparative histochemical composition of muscle fibers in a pre- and a postvertebral muscle of the cervical spine. J Anat 199:709–716
Boyd-Clark LC, Briggs CA, Galea MP (2002) Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine 27:694–701
Brennum J, Kjeldsen M, Jensen K et al (1989) Measurements of human pressure-pain thresholds on fingers and toes. Pain 38:211–217
Cameron I, Rebbeck T, Sindhusake D et al (2008) Legislative change is associated with improved health status in people with whiplash. Spine 35:250–254
Campbell WW, Vasconcelos O, Laine FJ (1998) Focal atrophy of the multifidus muscle in lumbosacral radiculopathy. Muscle Nerve 21:1350F–1353F
Crombez G, Vlaeyen J, Heuts P et al (1999) Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain 80:329–339
Curatolo M, Petersen-Felix S, Arendt-Nielsen L et al (2001) Central hypersensitivity in chronic pain after whiplash injury. Clin J Pain 17:306–315
Dall’Alba P, Sterling M, Treleaven JM et al (2001) Cervical range of motion discriminates between asymptomatic persons and those with whiplash. Spine 26:2090–2094
De Medinaceli L, Hurpeau J, Merle M et al (1999) Cold and post-traumatic pain: modeling of the peripheral nerve message. Biosystems 43:145–167
Drottning M, Staff P, Levin L et al (1995) Acute emotional response to common whiplash predicts subsequent pain complaints: a prospective study of 107 subjects sustaining whiplash injury. Nord J Psychiatry 49:293–299
Elliott J, Jull G, Noteboom JT et al (2006) Fatty infiltration in the cervical extensor muscles in persistent whiplash-associated disorders: a magnetic resonance imaging analysis. Spine 31:E847–E855
Elliott J, Sterling M, Noteboom JT et al (2008) Fatty infiltrate in the cervical extensor muscles is not a feature of chronic, insidious-onset neck pain. Clin Radiol 63:681–687
Ferrari R (2005) The whiplash encyclopedia. The fact and myths of whiplash, 2nd edn. Jones and Bartlett Publishers, Sudbury, MA, pp 121–145
Field S, Treleaven J, Jull G (2007) Standing balance: a comparison between idiopathic and whiplash-induced neck pain. Man Ther 13(3):183–191
Fleckenstein JL, Watamull D, Conner KE et al (1993) Denervated human skeletal muscle: MR imaging evaluation. Radiology 187:213–218
Gargan M, Bannister G, Main C et al (1997) The behavioural response to whiplash injury. J Bone Joint Surg Br 79:523–526
Goldberg D (1978) Manual of the General Health Questionnaire. NFER-Nelson, Windsor
Hayashi N, Masumoto T, Abe O et al (2002) Accuracy of abnormal paraspinal muscle findings on contrast-enhanced MR images as indirect signs of unilateral cervical root-avulsion injury. Radiology 223:397–402
Heikkila HV, Wenngren B (1998) Cervicocephalic kinesthetic sensibility, active range of cervical motion, and oculomotor function in patients with whiplash injury. Arch Phys Med Rehabil 79:1089–1094
Horowitz M, Wilner N, Alvarez W (1979) Impact of Event Scale: a measure of subjective stress. Psychosom Med 41:209–218
Jorum E, Warncke T, Stubhaug A (2003) Cold allodynia and hyperalgesia in neuropathic pain: the effect of N-methyl-D-Aspartate (NMDA) receptor antagonist ketamine-a double-blind, cross-over comparison with alfentanil and placebo. Pain 101:229–235
Joslin CC, Khan SN, Bannister GC (2004) Long-term disability after neck injury: A comparative study. J Bone Joint Surg [Br] 86:1032–1034
Kaale BR, Krakenes J, Albrektsen G et al (2005) Head position and impact direction in whiplash injuries: associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. J Neurotrauma 22:1294–1302
Kamper SJ, Rebbeck TJ, Maher CG et al (2008) Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain 138:617–629
Karlehagen S, Malt U, Hoff H et al (1993) The effect of major railway accidents on the psychological health of train drivers. J Psychosom Res 37:807–817
Kasch H, Qerama E, Bach FW et al (2005) Reduced cold pressor pain tolerance in non-recovered whiplash patients: a 1-year prospective study. Eur J Pain 9:561–569
Kori S, Miller R, Todd D (1990) Kinesphobia: a new view of chronic pain behaviour. Pain Management 35–43
Kristjansson E, Dall’Alba P, Jull G (2001) Cervicocephalic kinaesthesia: reliability of a new test approach. Physiother Res Int 6:224–235
Kristjansson E, Dall’Alba P, Jull G (2003) A study of five cervicocephalic relocation tests in three different subject groups. Clin Rehabil 17:768–774
Larsen LB, Holm R (2000) Prolonged neck pain following automobile accidents. Gender and age related risk calculated on basis of data from an emergency department. Ugeskr Laeger 162:178–181
Liu JX, Thornell LE, Pedrosa-Domellof F (2003) Muscle spindles in the deep muscles of the human neck: a morphological and immunocytochemical study. J Histochem Cytochem 51:175–186
Lovitt S, Moore SL, Marden FA (2006) The use of MRI in the evaluation of myopathy. Clin Neurophysiol 117:486–495
McDonald CM, Carter G, Fritz RC (2000) Magnetic resonance imaging of denervated muscle: comparison to electromyography. Muscle Nerve 23:1431–1434
McPartland JM, Brodeur RR, Hallgren RC (1997) Chronic neck pain, standing balance, and suboccipital muscle atrophy—a pilot study. J Manip Physiol Ther 20:24–29
Myran R, Kvistad KA, Nygaard OP et al (2008) Magnetic resonance imaging assessment of the alar ligaments in whiplash injuries: a case-control study. Spine 33:2012–2016
Pearce J (1999) A critical appraisal of the chronic whiplash syndrome. J Neurol Neurosurg Psychiatry 66:273–276
Pearcy M, Hindle R (1989) New method for the non-invasive three-dimensional measurement of human back movement. Clin Biomech 4:73–79
Peebles JE, McWilliams LA, MacLennan R (2001) A comparison of symptom checklist 90-revised profiles from patients with chronic pain from whiplash and patients with other musculoskeletal injuries. Spine 26:766–770
Pettersson K, Hildingsson C, Toolanen G et al (1994) MRI and neurology in acute whiplash trauma. No correlation in prospective examination of 39 cases. Acta Orthopaed Scand 65:525–528
Pettersson K, Hildingsson C, Toolanen G et al (1997) Disc pathology after whiplash injury. A prospective magnetic resonance imaging and clinical investigation. Spine 22:283–287 discussion 8
Pietrobon R, Coeytaux RR, Carey TS et al (2002) Standard scales for measurement of functional outcome for cervical pain or dysfunction: a systematic review. Spine 27:515–522
Radanov B, Begre S, Sturzenegger M et al (1996) Course of psychological variables in whiplash injury—a 2-year follow-up with age, gender and education in pair-matched patients. Pain 64:429–434
Revel M, Minquet M, Gergory P et al (1994) Changes in cervicocephalic kinesthesia after a proprioceptive rehabilitation program in patients with neck pain: a randomized controlled study. Arch Phys Med Rehabil 75:895–899
Riley L, Long D, Riley L (1995) The science of whiplash. Medicine 74:298–299
Scott D, Jull G, Sterling M (2005) Widespread sensory hypersensitivity is a feature of chronic whiplash-associated disorder but not chronic idiopathic neck pain. Clin J Pain 21:175–181
Spitzer W, Skovron M, Salmi L et al (1995) Scientific monograph of Quebec Task Force on whiplash associated disorders: redefining “whiplash” and its management. Spine 20:1–73
Sterling M, Jull G, Vicenzio B (2003) Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain 104:509–517
Sterling M, Jull G, Vicenzio B (2003) Development of motor dysfunction following whiplash injury. Pain 103:65–73
Sterling M, Jull G, Kenardy J (2006) Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain 122(1–2):102–108
Sterling M, Jull G, Vicenzino B et al (2005) Physical and psychological factors predict outcome following whiplash injury. Pain 114:141–148
Sterling M, Kenardy J, Jull G et al (2003) The development of psychological changes following whiplash injury. Pain 106:481–489
Sterling M, Treleaven J, Edwards S et al (2002) Pressure pain thresholds in chronic whiplash associated disorder: further evidence of altered central pain processing. J Musculoskelet Pain 10(3):69–81
Stovner LJ (1996) The nosologic status of the whiplash syndrome: a critical review based on a methodological approach. Spine 21:2735–2746
Tesio L, Alpini D, Cesarani A et al (1999) Short form of the Dizziness Handicap Inventory: construction and validation through Rasch analysis. Am J Phys Med Rehabil 78:233–241
Tjell C, Tenenbaum A, Sandstrom S (2002) Smooth Pursuit Neck Torsion Test—a specific test for whiplash associated disorders? J Whiplash Relat Disord 1:9–24
Treleaven J, Jull G, LowChoy N (2004) Smooth-pursuit neck torsion test in whiplash-associated disorders: relationship to self-reports of neck pain and disability, dizziness and anxiety. J Rehabil Med 36:1–5
Treleaven J, Jull G, Lowchoy N (2005) Standing balance in persistent whiplash: a comparison between subjects with and without dizziness. J Rehabil Med 37:224–229
Treleaven J, Jull G, Sterling M (2003) Dizziness and unsteadiness following whiplash injury: characteristic features and relationship with cervical joint position error. J Rehabil Med 35:36–43
Trott P, Pearcy M, Ruston S et al (1996) Three-dimensional analysis of active cervical motion: the effect of age and gender. Clin Biomech 11:201–206
Uetani M, Hayashi K, Hashmi R (1997) Traction injuries of the brachial plexus: signal intensity changes of the posterior cervical paraspinal muscles on MRI. J Comput Assist Tomogr 21:790–795
Vernon H, Mior S (1991) The Neck Disability Index: a study of reliability and validity. J Manip Physiol Ther 14:409–415
Vlaeyen J, Linton S (2000) Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain 85:317–332
Ware J, Snow K, Kosinski M et al (1993) SF-36 health survey: manual and interpretation guide. The Health Institute, Boston, MA
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Elliott, J., Sterling, M., Noteboom, J.T. et al. The clinical presentation of chronic whiplash and the relationship to findings of MRI fatty infiltrates in the cervical extensor musculature: a preliminary investigation. Eur Spine J 18, 1371–1378 (2009). https://doi.org/10.1007/s00586-009-1130-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-009-1130-6