
Abstract
Exercise rehabilitation is one of the few evidence-based treatments for chronic non-specific low back pain (cLBP), but individual success is notoriously variable and may depend on the patient’s adherence to the prescribed exercise regime. This prospective study examined factors associated with adherence and the relationship between adherence and outcome after a programme of physiotherapeutic spine stabilisation exercises. A total of 32/37 patients with cLBP completed the study (mean age, 44.0 (SD = 12.3) years; 11/32 (34%) male). Adherence to the 9-week programme was documented as: percent attendance at therapy, percent adherence to daily home exercises (patient diary) and percent commitment to rehabilitation (Sports Injury Rehabilitation Adherence Scale (SIRAS)). The average of these three measures formed a multidimensional adherence index (MAI). Psychological disturbance, fear-avoidance beliefs, catastrophising, exercise self-efficacy and health locus of control were measured by questionnaire; disability in everyday activities was scored with the Roland–Morris disability scale and back pain intensity with a 0–10 graphic rating scale. Overall, adherence to therapy was very good (average MAI score, 85%; median (IQR), 89 (15)%). The only psychological/beliefs variable showing a unique significant association with MAI was exercise self-efficacy (Rho = 0.36, P = 0.045). Pain intensity and self-rated disability decreased significantly after therapy (each P < 0.01). Adherence to home exercises showed a moderate, positive correlation with the reduction in average pain (Rho = 0.54, P = 0.003) and disability (Rho = 0.38, P = 0.036); higher MAI scores were associated with greater reductions in average pain (Rho = 0.48, P = 0.008) and a (n.s.) tendency for greater reductions in disability (Rho = 0.32, P = 0.07) Neither attendance at therapy nor SIRAS were significantly related to any of the outcomes. The benefits of rehabilitation depended to a large extent on the patient’s exercise behaviour outside of the formal physiotherapy sessions. Hence, more effort should be invested in finding ways to improve patients’ motivation to take responsibility for the success of their own therapy, perhaps by increasing exercise self-efficacy. Whether the “adherence–outcome” interaction was mediated by improvements in function related to the specific exercises, or by a more “global” effect of the programme, remains to be examined.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic low back pain (cLBP) is a complex and poorly understood problem and its management represents a major challenge to our health-care systems. According to current evidence-based clinical guidelines, exercise therapy (of any type) is one of the few recommended treatments for non-specific cLBP [2]. However, a recent meta-analysis of the results of exercise therapy trials reveals that even this gold standard treatment does not elicit a positive response in all patients, and the group mean changes in pain and disability, although statistically significant, are clinically only modest [25]. The reasons for the widely varying individual response to treatment are largely unknown; few studies have been able to identify predictors of a positive outcome [67]. Conceivably, one factor influencing individual success with such programmes may be the adherence of the patient to the treatment, where adherence implies active voluntary involvement in the planning and implementation of the treatment and is defined as the extent to which the patient undertakes the clinic-based and home-based prescribed components of the physiotherapy programme [6, 40, 54]. If the exercises that patients are instructed to perform are aimed at addressing specific functional deficits, have a sound underlying physiological rationale and demonstrate a dose–response relationship, then it could be expected that patients who adhere well to the prescribed exercise programme would fare better in terms of their final outcome.
Interindividual variability in adherence to medical treatment/therapy has been shown to be related to various personal characteristics including patients’ convictions in relation to their and others’ responsibility for their health and illness [12], self-efficacy, i.e. the belief that one is capable of performing in a certain manner to attain certain goals [3, 5, 12, 42, 49], patient activation, i.e. an individual’s declared propensity to engage in positive health behaviour [55], self-motivation [9, 10], sex and age [16], and the patient–therapist relationship [46]. Other psychological variables such as fear avoidance, catastrophising and psychological disturbance—factors that have been shown to be strong determinants of self-rated disability in cLBP [38, 41, 57]—have not yet been examined within the context of adherence, but might also be expected to represent barriers to exercise for the same reasons that they influence perceived disability in activities of daily living or work.
A number of studies have examined adherence to exercise rehabilitation in patients with LBP [16, 18, 19, 22, 29, 31, 52] or after back surgery [55], but only one of these [18, 19] specifically involved patients with a chronic problem. Further, most of these studies focused on the use of adherence-enhancing strategies in groups of patients [18, 19, 22, 29, 52], the evaluation of different measures of adherence [31] or the identification of factors predicting adherence per se [16, 55], rather than on the relationship between individual adherence and clinical outcome after therapy. Although Kolt and McEvoy [31] found that higher levels of adherence significantly predicted the global perception of the “degree of rehabilitation” after a 4-week exercise programme, they did not quantify the changes in clinical status prospectively, using established and standardised LBP outcome instruments. Moreover, their use of a mixed group of acute and chronic LBP patients, for whom current management guidelines differ somewhat with regard to the benefit of special exercises [2, 62], and the fact that “duration of current LBP” was itself identified as a predictor of outcome in their multivariate model, complicates the interpretation of their findings.
The purpose of the present study was twofold. The primary aim was to examine the influence of adherence on changes in self-rated pain and disability after a programme of therapeutic “spinal segmental stabilisation” exercises [47] in patients with cLBP. The specific exercises, which aim to restore deep trunk muscle motor control [47], have become a popular concept in contemporary physiotherapy, following numerous scientific reports of the trunk muscle dysfunction in connection with LBP (reviewed in [28]). A secondary aim was to evaluate the influence of various cognitive factors and beliefs on adherence to the exercise programme.
Methods
Patients
A total of 37 patients with cLBP participated in the study (see later for further details), which was part of a larger investigation of various aspects of deep trunk muscle activation in cLBP. The patients were recruited from the departments of rheumatology, orthopaedics and neurology of local participating hospitals (one university hospital, two foundation hospitals) and a local GP practice. The inclusion criteria for the study were: non-specific LBP [2, 64] with or without referred pain (of a non-radicular nature) for at least 3 months and about to undergo physiotherapy; average pain intensity over the last 2 weeks ≥3 and ≤8 on a 0–10 visual analogue scale; good understanding (written and oral) of the German language; and willingness to comply with the study protocol. Exclusion criteria included factors reflecting the presence of serious spinal disorders, as described in LBP treatment guidelines [2, 64], as well as pregnancy within the last 2 years (potential for subsequent changes in abdominal muscle function) and prior participation in a programme of spine segmental stabilisation exercises. The study was approved by the local medical ethics committee. All participants gave their signed informed consent to participate after receiving verbal and written information about the study.
Therapy
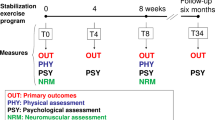
Patients were referred to a 9-week programme of spine segmental stabilisation exercises, directed by a physiotherapist who was specially trained in this therapy concept and in the additional needs of the study, but otherwise treating the patient as one of his/her normal clinical referrals. In total, 12 treating therapists were involved. Attendance at physiotherapy was required once/week. Patients firstly underwent a manual assessment by the physiotherapist to determine if there were any signs of segmental hypomobility or hypermobility [43]; if present, these were categorised according to their directional nature (flexion, extension, lateral bending or multidirectional pattern), and the progression of the exercises was directed accordingly [43]. The treatment approach was based on the methods described by Richardson et al. [47]. Stage 1 involved training of preferential activation of the deep abdominal muscles, with correct breathing and without substitution from large torque-producing muscles (e.g. M. rectus abdomis), using the abdominal drawing in manoeuvre. The hold was assessed using a pressure biofeedback monitor and the holding time was gradually increased to the point where patients were able to perform ten contractions with 10-s holds. The physiotherapist then used B-mode ultrasound to verify the contraction, i.e. to ensure that there was visible thickening and shortening of the muscles [26, 47]. Stage 2 included training of specific contraction of the deep abdominal muscles with co-activation of the pelvic floor muscles (if signs of pelvic floor muscle insufficiency were present), M. multifidus and M. iliopsoas. Stage 3 comprised integration of the use of these specific exercises during performance of different activities of daily living or sport (tailored to the patient’s needs), especially in relation to movements where the patient demonstrated fear of pain [27, 30, 47, 48]. Exercise progression was achieved by applying low, but increasingly greater, loads to the muscles by adding leverage through the limbs. During at least one of the nine physical therapy sessions, ultrasound was used as a biofeedback instrument for the patient [26] and to guide progression through the stages.
Patients were asked to perform home exercises comprising a sequence of 10 × 10 s repetitions, ten times a day (total exercise time, approximately 20–25 min/day). Patients were given approximately three different exercise positions to use; the aim was to find an exercise setting that was not associated with excessive time demands or alterations to the individual’s usual daily routine. To explain the rationale behind the treatment concept and increase motivation for the programme, patients were given illustrated information brochures describing the exercises, their purpose and how to perform them, and offering various tips and advice on how to integrate the exercises into their activities of daily living. The physiotherapist was instructed to enquire at every treatment session about the patient’s success with the home exercises and to discuss any problems/provide support and advice where necessary.
Adherence to therapy
Since clinical exercise programmes typically make multiple demands on the patient (attendance for treatment, home exercises and the incorporation/elimination of certain movements during everyday activities [10, 36]), three indices, and a multidimensional index (aimed at incorporating all components into one score) were used to capture these various dimensions of adherence. Firstly, a self-report daily exercise diary completed by the patient served to document the frequency of exercises performed at home. The total number of home exercise sessions carried out was expressed as a proportion (%) of the recommended total number of sessions to be performed during the 9-week programme (the maximum value for this was set to 100%, even if more than the required number were performed). The diary was given out anew each week and returned (complete) by the patient at the next therapy session. Secondly, the treating physiotherapist documented his/her impression of the patient’s adherence during each therapy session using the Sports Injury Rehabilitation Adherence Scale (SIRAS) [7]; this assesses the effort that the patient displays when carrying out the exercises, the frequency with which the patient follows the therapist’s instructions and the receptiveness of the patient towards progression. Each of these three aspects was assessed on a 5-point scale, giving a total score between 3 and 15 for each session. The average score over the nine treatment sessions was then determined and expressed as a percentage (where a score of 15 = 100%). Finally, the percent attendance at the prescribed therapy sessions was documented, as described previously [36, 51, 52]. The scores for each of these three dimensions (expressed as a percentage) were averaged to give a score for the multidimensional adherence index (MAI).
At the end of the programme, the physiotherapist was asked to give a global rating of the patient’s overall adherence: poor, fair, good, very good and excellent (range, 0–4). This was used to compare with the MAI score, with the expectation that there would be a moderately high, significant correlation between the scores.
Questionnaires
Before and after therapy, the patients completed a questionnaire booklet. It contained amongst other things:
-
Questions on sociodemographic variables;
-
Questions on pain history (duration of problem, length of time in treatment, work absence, etc.);
-
The Exercise Self-Efficacy Questionnaire, which comprises 11 items enquiring about how confident the patient is that he will carry out the home exercises despite various distractions (0–66, from not certain at all through to absolutely certain) [5];
-
The multidimensional health locus of control (HLC) questionnaire, which examines beliefs that the source of reinforcement for health-related behaviour is primarily internal, a matter of chance or under the control of powerful others [35, 66];
-
Roland and Morris disability questionnaire (RM), which measures 24 activity limitations due to back pain (score 0–24: higher score, increased disability) [17, 50];
-
Pain graphic rating scale (PGRS) [37]: the average and worst back pain intensity during the last week was measured using a 0–10 graphic rating scale.
-
Pain frequency, assessed using a four-point adjectival scale (0 = never, 1 = occasionally, 2 = frequently, 3 = constantly);
-
Pain medication usage, assessed with a four-point adjectival scale (0 = never, 1 = few times/month, 2 = few times/week, 3 = daily);
-
Fear-avoidance beliefs, determined with the fear avoidance beliefs questionnaire [57, 65]. This assesses the patient’s beliefs about physical activity/work being a cause of back trouble and their fears about the dangers/consequences of such activities when experiencing an episode of low back pain;
-
Pain catastrophising questionnaire [41, 60]. This comprises three subscales, helplessness, magnification and rumination, which among them assess the extent of the patient’s catastrophising thoughts and behaviours;
-
Psychological disturbance/distress, determined using the combined scores of the Modified Somatic Perception Questionnaire (heightened somatic awareness) and the modified Zung self-rating depression questionnaire [23, 39].
After the therapy programme, the questionnaire booklet also included six questions regarding the patient’s impression of the therapist, in terms of his/her friendliness, competence, provision of advice for performing everyday activities, ability to motivate, empathy/understanding and strictness/consistency, each graded on a 0–4-point adjectival scale [39]. The sum score for these six items was used to describe the patient’s overall relationship with the therapist.
Statistical analysis
The main aim of the study was to examine the influence of adherence on outcome. A sample size of approximately 35–40 patients allowed for the determination of a moderate correlation between multidimensional adherence and the post-treatment change in pain/disability of r = 0.5 (i.e. 25% shared variance), with a probability of 85% (power) against the null hypothesis of r = 0, at a two-sided significance level of 5% and allowing for ~20% dropout.
Descriptive data are presented as means and standard deviations (SD), or medians and interquartile ranges (IQR), depending on whether the data were approximately normally distributed when examined graphically. The interrelationships between adherence and various personal characteristics were quantified using Spearman’s rank correlation coefficients. Differences in adherence between the sexes were examined using Mann–Whitney U tests. Differences between clinical variables before and after treatment were examined using paired t tests, and effect sizes for the changes were calculated as standardised response means (SRMs), given by the mean change scores divided by the SD of the change scores. Forward stepwise multiple regression analysis was used to identify unique predictors of adherence, entering those variables that were significant on bivariate testing. The negatively skewed data for adherence (SIRAS, attendance and MAI) underwent reflection and inverse transformation as described by Brewer et al. [10] to produce a more normal distribution for use in multiple regression.
Significance was accepted at the 5% level. Following the reasoning of Perneger et al. [45], no corrections were made for multiple testing. The analyses were carried out using Statview 5.0 (SAS Institute Inc, San Francisco, USA).
Results
Patient flow through the study
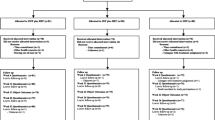
A total of 32/37 (86%) patients completed the 9-week physiotherapy programme of spine stabilisation exercises and completed the pre- and post-therapy questionnaire assessments. Five patients were considered to be dropouts: for two patients, recruited early on in the study, it transpired that they had never fulfilled the study’s admission criteria [one for language reasons and one for medical reasons (specific spinal pathology)], and three patients did not wish to continue for various reasons, mainly to do with the time commitment.
The baseline physical, psychological and clinical characteristics of the 32 patients are shown in Table 1 and in the first column of Table 3.
Adherence to therapy
Overall, the patients showed good adherence to the programme, with median scores for attendance, commitment (SIRAS) and adherence to home exercises of 100% (IQR 11%), 96% (IQR 8%) and 75% (IQR 41%), respectively (for further details, see Table 2).
Each adherence subscale showed at least a moderate correlation with the MAS score (Rho corrected for ties = 0.51–0.94; P < 0.05), whereas the intercorrelations between any two subscales were relatively low (Rho corrected for ties P = 0.29–0.34; P = 0.06–0.10).
The physiotherapists’ retrospective global rating of the patients’ adherence was as follows: 37.5% excellent, 25.0% very good, 28.1% good, 3.1% fair and 6.3% poor. There was a significant correlation between the global ratings and the MAI scores (Rho = 0.57; P = 0.0014).
Factors associated with adherence to therapy
Men had significantly higher scores than women for the MAI (P = 0.02), and for the individual dimensions ‘home exercises’ (P = 0.02) and ‘SIRAS’ (P = 0.01), but not for ‘attendance at therapy’ (P = 0.92). The physiotherapist’s global rating was also higher for men than for women (median (IQR) values, 4 (1) and 3 (0.3), respectively; P = 0.03). There was no significant relationship between age and MAI or any of its component dimensions (Rho < 0.16, P > 0.37 in each case).
The scores for exercise self-efficacy showed a low, but significant, correlation with the MAI scores (Rho = 0.36, P = 0.045). None of the scores for the different domains of the MHLC (internal, powerful others, fate) showed any significant correlation with the MAI scores (all Rho < −0.21, P > 0.24). Further, none of the psychological questionnaire scores (fear-avoidance beliefs, catastrophising or psychological disturbance/distress) were significantly correlated with the MAI scores (all Rho < −0.18, P > 0.32).
The median sum score for the patients’ overall impression/rating of the therapist was 22 (IQR 3) out of a maximum 24. There was no significant correlation between this score and the MAI score (Rho = −0.051, P = 0.77).
Forward stepwise multiple linear regression analysis of gender and self-efficacy scores (significant in the bivariate analyses) on the transformed MAI adherence scores revealed that both variables were significant predictors, together accounting for approximately 32% variance (adjusted R 2) in MAI (P = 0.0013; standardised coefficient (beta) for gender (1 = female/2 = male), 0.457; for self-efficacy, 0.400).
Clinical outcomes before and after therapy
Significant reductions in disability, pain intensity (both average and worst in the last week), pain frequency and pain medication usage were found after the 9-week therapy programme (Table 3). Effect sizes ranged from 0.49 (for worst pain) to 0.94 (pain frequency).
Relationship between adherence to therapy and clinical outcome
The “percent adherence to home exercises” showed a moderate, significant correlation with the reduction in average pain (Rho = 0.54, P = 0.003) and reduction in Roland–Morris disability (Rho = 0.38, P = 0.036). The MAI also correlated significantly with the reduction in average pain (Rho = 0.48, P = 0.008); its relationship with disability just failed to reach significance (Rho = 0.32, P = 0.07), although there was a significant concordance between the scores (higher MAI and reduced disability; Kendall’s tau = 0.25, P = 0.048). Attendance at therapy and the SIRAS score were not significantly related to any of the clinical outcomes.
Discussion
Summary of main findings
The present study sought to evaluate the personal factors associated with adherence to a programme of “spinal segmental stabilisation” exercises in patients with chronic LBP and to determine whether adherence had any significant relationship with clinical outcome. Exercise self-efficacy was the only psychological/beliefs variable that uniquely explained a significant proportion of the variance in individual patterns of multidimensional adherence; in turn, adherence showed a significant association with the reductions in average pain and disability after therapy.
Adherence to the programme of exercises
The overall level of adherence shown by the patients in the present study was high. The average attendance at the prescribed therapy sessions was 94%, which compares well with previous reports of 76% [55], 88% [31] and 86%, increasing to 96% with deliberate motivational efforts [19]. The positive patient ratings of the physiotherapist, and perhaps also the need to attend only once per week, may have contributed to the high attendance rates. The physiotherapists’ rating of the patients’ commitment during therapy was also high, with the group scoring an average of 93% of maximum on the SIRAS scale. This was somewhat higher than the score reported in a previous study of exercise therapy for (mainly acute) LBP (75%, rising to 81% for non-compensable patients) [31], although the demands of the clinic-based part of the current treatment, in terms of its complexity, were probably much lower.
In the present study, the patients reported completing on average 68% of their home exercises, which compares well with the 71% reported by Kolt and McEvoy [31]. The slightly lower adherence rate in the present study may be the result of the daily exercise requirement and the longer course of treatment (9 weeks) compared with previous studies (2 weeks [52], 4 weeks [31]). Attempts were made to optimise adherence to home exercises by providing written and illustrated instructions, explaining both the purpose of the exercises and the manner in which they should be executed. In previous studies, such additional reference material was shown to improve adherence to home exercise programmes from 38% (when giving verbal instructions only) up to 77% [52].
In relation to all the above aspects, the special study setting and the Hawthorne effect, in which individuals temporarily change their performance in response to being observed, may also have played a role in eliciting such good adherence rates (see later).
Factors explaining the variance in adherence
Of all the psychological and personal characteristics that were examined, only male gender and self-efficacy had any significant role in explaining the variance in (some aspects of) adherence. Men had significantly higher scores for adherence to home exercises, SIRAS and MAI, and for the physiotherapist’s global rating of adherence, but not for attendance at therapy. This may reflect a greater commitment to the more “active” part of the treatment (home exercises and behaviour during the therapy) in contrast to the part of “simply turning up”, or it may result from the fact that attendance was the only objective measure amongst the battery of otherwise subjective (patient or physiotherapist) indices. Some previous studies have similarly identified women as being less adherent than men, at least in terms of their exercise frequency, if not in terms of their overall completion rates of rehabilitation programmes [16]. This has been interpreted as a reflection of the known tendency of women to prioritise others before themselves in terms of time, money and devotion [16]. Others, however, have found no influence of gender on adherence [56], even when measured using the same three dimensions used in the present study [31]. It has been reported that, with regard to adherence to medical treatments in general, patients’ demographic characteristics (age, gender, education) prove less important than psychological or social factors [15].
Self-efficacy, i.e. the belief that one is capable of performing in a certain manner to attain certain goals, correlates positively with success in all realms of personal endeavour. It has received recognition as a predictor of health behaviour change and maintenance in various fields of medicine [59]. In the present study, self-efficacy showed a relatively low, but nonetheless significant, correlation with multidimensional adherence and remained the only significant predictor when entered together with gender into a multivariate model. Skolasky et al. [55] reported similar findings on the importance of self-efficacy in predicting “attendance at therapy” and “engagement in therapy” in patients undergoing rehabilitation after spinal surgery, with self-efficacy being the strongest unique predictor in their multivariate model. Since self-efficacy is susceptible to modification with appropriate education and training [53], it obviously constitutes an important target of intervention when striving to improve adherence to exercise therapy programmes.
In other fields of medicine, it has been shown that individuals who believe their own behaviour is instrumental in governing their health (high internal HLC) are more likely to adhere to exercise therapy [11, 12]. However, in relation to exercise adherence in LBP, the role of HLC appears to be equivocal. In the present study, HLC explained none of the variance in multidimensional adherence. A similar lack of association with adherence measured as “engagement in therapy” was found in patients undergoing rehabilitation after back surgery, although internal HLC did explain a small, but significant, amount of the variance in “attendance at therapy” [55]. Engstrom et al. [16] reported no difference in the scores for HLC in completers and non-completers of a musculoskeletal rehabilitation programme, but a minor influence of one HLC dimension in governing exercise frequency during rehabilitation. As has been argued before [24, 32], it may be that the generic measure of HLC lacks specificity and that a condition-specific HLC scale would have had more predictive power.
In the present study, no associations were observed between psychological disturbance (depression and heightened somatic awareness) and adherence to exercise therapy, confirming the findings of Skolasky et al. [55] and Alexandre et al. [4]. Harkapaa et al. [24] showed that the ability to correctly perform the given back exercises, but not the frequency of their execution, was lower in patients with psychological distress, hypothesising that this may reflect an influence of distress on the learning process per se.
In recent years, fear-avoidance beliefs (FAB) have received a lot of attention in the literature in relation to their association with self-rated disability and work capacity [20, 38, 57, 63, 68] and the outcome of physical therapy [21]. However, they have not been examined within the context of adherence. We hypothesised that FAB might have a bearing on adherence, especially in relation to the performance of home exercises, done without the guidance and “protection” of the physiotherapist. However, we could demonstrate no such associations. Possibly, this was the result of the low-intensity nature of the exercises used in the present study, and their lack of perceived “threat” in terms of their potential to overload or damage the painful back. Given its role in priming fear mechanisms [13, 63] and its influence on the individual’s perception of their ability to function [61], catastrophising was similarly investigated as a potential determinant of adherence to exercise. However, maybe for the same reasons as described for FAB, it too displayed no association with any of the dimensions of adherence.
Influence of adherence on outcome
It would seem logical to assume that the more adherent an individual is to the prescribed therapy, the more successful his/her outcome should be. Indeed, this is the motivation behind attempts to develop adherence-promoting measures to accompany medical therapies. In the present study, both the MAI and adherence to home exercises demonstrated significant relationships with outcome, measured either as a reduction in pain intensity or reduction in self-rated disability. The SIRAS and “attendance at therapy” scores alone, however, had no influence on outcome.
Few studies have specifically examined the dose–response relationship (adherence–outcome) in relation to cLBP patients, but the literature from closely related fields, examining groups dichotomised by their level of adherence, suggests that the situation is not straightforward. In a group of workers with musculoskeletal pain, Linton et al. [34] revealed that “compliers” with an exercise programme achieved a significantly higher aerobic capacity than “non-compliers”, but the change in pain after the programme did not differ between the groups. Similarly, Göhner and Schlicht [22] were able to develop methods for successfully enhancing exercise adherence in patients with subacute LBP, but this did not result in any improvement in pain reduction compared with a control group doing exercise alone. Jackson et al. [29] also applied methods to maximise treatment adherence to therapeutic exercise in patients with LBP (of an unspecified duration) and though they recorded an adherence rate of 92% compared with 50% in the control group, they nonetheless found no significant differences between groups in the pain levels reported at the end of the therapy programme. In a mixed group of predominantly acute/subacute LBP patients undertaking a 4-week exercise programme, Kolt and McEvoy [31] found that the SIRAS made a significant contribution to a multivariate model predicting the patients’ (though not the physiotherapist’s) rating of “the extent to which they had been rehabilitated”. However, this rating is not an established LBP outcome measure [14], and there may be unknown biases associated with the retrospective nature of this global measure of improvement.
There are a number of potential reasons explaining why the expected relationship between adherence and outcome was able to be identified in the present study, but not (or less convincingly so) in earlier studies of LBP patients. Many previous studies included acute LBP patients for whom the prognosis is considerably more favourable than for chronic patients [44]. This would be expected to confound the measures of outcome, since there would be many patients, who, simply due to the favourable natural history, would recover regardless of what they did (or did not do). Indeed, in the Kolt and McEvoy study [31], the duration of the LBP episode was itself a significant predictor of outcome in both their multivariate models. Possibly, also the more intensive nature of the exercises used in some studies and the fact that their performance caused a transient increase in pain [33] may explain the lack of a dose–response relationship when outcome was measured as overall pain. These types of exercises may be limited in the immediacy of their benefits and may be better perceived as something of an “investment”, leading to improved physical capacity and fewer or less severe attacks of LBP in the future. Perhaps, the assessment of outcome as the change in disability (rather than pain) would have led to different conclusions on the adherence–outcome relationship in some of the earlier studies.
It is interesting to speculate on the “cause and effect” nature of the adherence–outcome relationship observed in the present study, i.e. were patients adherent over the 9-week period because their symptoms were decreasing (for whatever reason) and, convinced that the exercises were responsible, this gave them both the motivation and capacity to persevere? Or was the clinical change truly the result of the regular performance of the specific exercises? One way to address this issue would be to examine whether the adherence–outcome interaction is mediated by improvements in function related to the specific exercises. This will be the subject of a future paper. Either way, it seems likely to be some sort of reinforcement mechanism, whereby improved clinical status provides positive feedback to continue exercising. In the present study, it appeared that the critical part of the therapy concerned how much the patient did for himself/herself outside of the formal physiotherapy sessions. This seems to be typical of rehabilitation protocols that call for relatively few clinic visits [8]. Clearly, more effort should be invested in finding ways to improve patients’ motivation to take responsibility for the success of their own therapy. In accordance with the findings discussed earlier regarding predictors of adherence, this would likely involve the introduction of educational or cognitive-behavioural measures to improve self-efficacy.
Limitations of the study
The present study was not without its limitations. The prime limitation was that, although commensurate with the figures reported for similar studies in the literature, our adherence rates were more positive than those reported for physiotherapy rehabilitation in clinical practice (poor adherence in up to 65% patients [6]). As alluded to earlier, this may reflect a sort of Hawthorne effect (improved performance on observation), or it may indicate that the characteristics of the group under study were “atypical” in some respect. Either way, it may question the external validity of the study and its generalisability to “daily practice”. On the other hand, if it simply reflects the benefits of providing supplementary adherence-enhancing material (and this was an intentional and integral part of the current programme), then it delivers valuable information for daily practice. This warrants further evaluation in relation to this particular form of exercise therapy. It should also be noted that the patients were predominantly recruited from tertiary care providers and hence the results may not be generalisable to patients with cLBP in other health-care settings.
The high levels of adherence to the clinic-based part of the treatment, coupled with the relatively small group size, posed another notable difficulty: the lack of variability among patients when attempting to predict individual adherence patterns. These factors may have accounted for the failure to identify any associations between the clinic-based measures of adherence and baseline characteristics or outcome. To reveal any such potential associations (or, indeed, repudiate their existence), a larger group of patients with a greater range of scores for attendance and commitment to therapy would perhaps be required. The findings of this initial exploratory study should hence be re-examined in larger groups of patients, in the everyday clinical setting.
Completion of the exercise diary on a daily basis was expected to introduce less recall bias than reports completed retrospectively at the end of each week [31], or upon the conclusion of treatment [29]. Nonetheless, as with all such self-report measures, they may have been susceptible to social desirability effects [1, 58].
The largely correlational nature of the study precludes conclusions being drawn regarding causality for many of the associations described, although the prospectively collected data provides some evidence of at least a time-order relationship between self-efficacy and adherence. Randomised controlled studies should be carried out in which self-efficacy is manipulated and the consequences are observed, to confirm the predictive nature of the relationship within this rehabilitation setting.
References
Adams SA, Matthews CE, Ebbeling CB, Moore CG, Cunningham JE, Fulton J, Hebert JR (2005) The effect of social desirability and social approval on self-reports of physical activity. Am J Epidemiol 161:389–398. doi:10.1093/aje/kwi054
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G (2006) Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J 15(Suppl 2):S192–S300. doi:10.1007/s00586-006-1072-1
Alewijnse D, Mesters I, Metsemakers J, Adriaans J, van den Borne B (2001) Predictors of intention to adhere to physiotherapy among women with urinary incontinence. Health Educ Res 16:173–186. doi:10.1093/her/16.2.173
Alexandre NM, Nordin M, Hiebert R, Campello M (2002) Predictors of compliance with short-term treatment among patients with back pain. Rev Panam Salud Publica 12:86–94. doi:10.1590/S1020-49892002000800003
Bandura A (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 84:191–215. doi:10.1037/0033-295X.84.2.191
Bassett S (2003) The assessment of patient adherence to physiotherapy rehabilitation. NZ J Physiotherapy 31:60–66
Brewer BW, Avondolglio JB, Cornelius AE (2002) Construct validity and interrater agreement of the sport injury rehabilitation adherence scale. J Sport Rehabil 11:170–178
Brewer BW, Cornelius AE, Van Raalte JL, Brickner JC, Sklar JH, Corsetti JR, Pohlman MH, Ditmar TD, Emery K (2004) Rehabilitation adherence and anterior cruciate ligament reconstruction outcome. Psychol Health Med 9:163–175. doi:10.1080/13548500410001670690
Brewer BW, Cornelius AE, Van Raalte JL, Petitpas AJ, Sklar JH, Pohlman MH, Krushell RJ, Ditmar TD (2003) Age-related differences in predictors of adherence to rehabilitation after anterior cruciate ligament reconstruction. J Athl Train 38:158–162
Brewer BW, Van Raalte JL, Cornelius AE, Van Raalte JL, Petitpas AJ, Sklar JH, Pohlman MH, Krushell RJ, Ditmar TD (2000) Psychological factors, rehabilitation adherence, and rehabilitation outcome following anterior cruciate ligament reconstruction. Rehabil Psychol 45:20–37. doi:10.1037/0090-5550.45.1.20
Chen CY, Neufeld PS, Feely CA, Skinner CS (1999) Factors influencing compliance with home exercise programs among patients with upper-extremity impairment. Am J Occup Ther 53:171–180
Christensen AJ (2004) Patient adherence to medical treatment regimes: bridging the gap between behavioural science and biomedicine. Yale University Press, New Haven
Crombez G, Eccleston C, Baeyens F, Eelen P (1998) When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 75:187–198. doi:10.1016/S0304-3959(97)00219-4
Deyo RA, Battie M, Beurskens AJHM, Bombardier C, Croft P, Koes B, Malmivaara A, Roland M, Von Korff M, Waddell G (1998) Outcome measures for low back pain research. A proposal for standardized use. Spine 23:2003–2013. doi:10.1097/00007632-199809150-00018
DiMatteo MR (2004) Evidence-based strategies to foster adherence and improve patient outcomes. JAAPA 17:18–21
Engstrom LO, Oberg B (2005) Patient adherence in an individualized rehabilitation programme: a clinical follow-up. Scand J Public Health 33:11–18. doi:10.1080/14034940410028299
Exner V, Keel P (2000) Erfassung der Behinderung bei Patienten mit chronischen Rückenschmerzen. Schmerz 14:392–400. doi:10.1007/s004820070004
Friedrich M, Gittler G, Arendasy M, Friedrich KM (2005) Long-term effect of a combined exercise and motivational program on the level of disability of patients with chronic low back pain. Spine 30:995–1000. doi:10.1097/01.brs.0000160844.71551.af
Friedrich M, Gittler G, Halberstadt Y, Cermak T, Heiller I (1998) Combined exercise and motivation program: effect on the compliance and level of disability of patients with chronic low back pain: a randomized controlled trial. Arch Phys Med Rehabil 79:475–487. doi:10.1016/S0003-9993(98)90059-4
Fritz JM, George SZ (2002) Identifying psychosocial variables in patients with acute work-related low back pain: the importance of fear-avoidance beliefs. Phys Ther 82:973–983
George SZ, Fritz JM, Childs JD (2008) Investigation of elevated fear-avoidance beliefs for patients with low back pain: a secondary analysis involving patients enrolled in physical therapy clinical trials. J Orthop Sports Phys Ther 38:50–58
Göhner W, Schlicht W (2006) Preventing chronic back pain: evaluation of a theory-based cognitive-behavioural training programme for patients with subacute back pain. Patient Educ Couns 64:87–95. doi:10.1016/j.pec.2005.11.018
Greenough CG, Fraser RD (1991) Comparison of eight psychometric instruments in unselected patients with back pain. Spine 16:1068–1074. doi:10.1097/00007632-199109000-00010
Harkapaa K, Jarvikoski A, Mellin G, Hurri H, Luoma J (1991) Health locus of control beliefs and psychological distress as predictors for treatment outcome in low-back pain patients: results of a 3-month follow-up of a controlled intervention study. Pain 46:35–41. doi:10.1016/0304-3959(91)90031-R
Hayden JA, van Tulder MW, Malmivaara AV, Koes BW (2005) Meta-analysis: exercise therapy for nonspecific low back pain. Ann Intern Med 142:765–775
Henry SM, Teyhen DS (2007) Ultrasound imaging as a feedback tool in the rehabilitation of trunk muscle dysfunction for people with low back pain. J Orthop Sports Phys Ther 37:627–634
Hodges PW (2001) Changes in motor planning of feedforward postural responses of the trunk muscles in low back pain. Exp Brain Res 141:261–266. doi:10.1007/s002210100873
Hodges PW, Moseley G (2003) Pain and motor control of the lumbopelvic region: effect and possible mechanisms. J Electromyogr Kinesiol 13:361–370. doi:10.1016/S1050-6411(03)00042-7
Jackson LD (1994) Maximizing treatment adherence among back-pain patients: an experimental study of the effects of physician-related cues in written medical messages. Health Commun 6:173–191. doi:10.1207/s15327027hc0603_1
Jull GA, Richardson CA (2000) Motor control problems in patients with spinal pain: a new direction for therapeutic exercise. J Manipulative Physiol Ther 23:115–117. doi:10.1016/S0161-4754(00)90079-4
Kolt GS, McEvoy JF (2003) Adherence to rehabilitation in patients with low back pain. Man Ther 8:110–116. doi:10.1016/S1356-689X(02)00156-X
Laffrey SC, Isenberg M (1983) The relationship of internal locus of control value placed on health, perceived importance of exercise, and participation in physical activity during leisure. Int J Nurs Stud 20:187–196. doi:10.1016/0020-7489(83)90058-5
Linton SJ (1994) Chronic back pain: integrating psychological and physical therapy-an overview. Behav Med 20:101–104
Linton SJ, Hellsing A-L, Bergstrom G (1996) Exercise for workers with musculoskeletal pain: does enhancing compliance decrease pain? J Occup Rehabil 6:177–190. doi:10.1007/BF02110754
Lohaus A, Schmitt GM (1989) Kontrollüberzeugungen zu Krankheit und Gesundheit (KKG): Bericht über die Entwicklung eines Testverfahrens. Diagnostica 35:59–72
Lyngcoln A, Taylor N, Pizzari T, Baskus K (2005) The relationship between adherence to hand therapy and short-term outcome after distal radius fracture. J Hand Ther 18:2–8. quiz 9. doi:10.1197/j.jht.2004.10.008
Mannion AF, Balague F, Pellise F, Cedraschi C (2007) Pain measurement in patients with low back pain. Nat Clin Pract Rheumatol 3:610–618. doi:10.1038/ncprheum0646
Mannion AF, Junge A, Taimela S, Muntener M, Lorenzo K, Dvorak J (2001) Active therapy for chronic low back pain: part 3. Factors influencing self-rated disability and its change following therapy. Spine 26:920–929. doi:10.1097/00007632-200104150-00015
Mannion AF, Müntener M, Taimela S, Dvorak J (1999) A randomised clinical trial of three active therapies for chronic low back pain. Spine 24:2435–2448. doi:10.1097/00007632-199912010-00004
Meichenbaum D, Turk DC (1987) Facilitating treatment adherence: a practitioner’s guidebook. Plenum Press, New York
Meyer K, Sprott H, Mannion AF (2008) Cross-cultural adaptation, reliability, and validity of the German version of the pain catastrophizing scale. J Psychosom Res 64:469–478. doi:10.1016/j.jpsychores.2007.12.004
Nicholson RA, Houle TT, Rhudy JL, Norton PJ (2007) Psychological risk factors in headache. Headache 47:413–426
O’Sullivan PB (2000) Lumbar segmental ‘instability’: clinical presentation and specific stabilizing exercise management. Man Ther 5:2–12. doi:10.1054/math.1999.0213
Pengel LH, Herbert RD, Maher CG, Refshauge KM (2003) Acute low back pain: systematic review of its prognosis. BMJ 327:323. doi:10.1136/bmj.327.7410.323
Perneger TV (1998) What’s wrong with Bonferroni adjustments. BMJ 316:1236–1238
Pizzari T, McBurney H, Taylor NF, Feller JA (2002) Adherence to anterior cruciate ligament rehabilitation: a qualitative analysis. J Sport Rehabil 14:90–102
Richardson C, Jull G, Hodges P, Hides J (1999) Therapeutic exercise for spinal stabilisation: scientific basis and practical techniques. Churchill Livingstone, Edinburgh
Richardson CA, Jull GA (1995) Muscle control—pain control. What exercises would you prescribe? Man Ther 1:2–10. doi:10.1054/math.1995.0243
Robertson D, Keller C (1992) Relationships among health beliefs, self-efficacy, and exercise adherence in patients with coronary artery disease. Heart Lung J Crit Care 21:56–63
Roland M, Fairbank J (2000) The Roland Morris disability questionnaire and the oswestry disability questionnaire. Spine 25:3115–3124. doi:10.1097/00007632-200012150-00006
Scherzer CB, Brewer BW, Cornelius AE, Van Raalte JL, Petitpas AJ, Sklar JH, Pohlman MH, Krushell RJ, Ditmar TD (2001) Psychological skills and adherence to rehabilitation after reconstruction of the anterior cruciate ligament. J Sport Rehabil 10:165–172
Schneiders AG, Zusman M, Singer KP (1998) Exercise therapy compliance in acute low back pain patients. Man Ther 3:147–152. doi:10.1016/S1356-689X(98)80005-2
Schumacher JE, Engle M, Reynolds K, Houser S, Mukherjee S, Caldwell E, Kohler C, Phelan S, Raczynski JM (2000) Measuring self-efficacy in substance abuse intervention in obstetric practices. South Med J 93:406–414
Shumaker SA, Schron EB, Ockene JK (1990) The handbook of health behaviour change. Springer Publishing, New York
Skolasky RL, Mackenzie EJ, Wegener ST, Riley LH 3rd (2008) Patient activation and adherence to physical therapy in persons undergoing spine surgery. Spine 33:E784–E791
Sluijs EM, Kok GJ, Van der Zee J, Turk DC, Riolo L (1993) Correlates of exercise compliance in physical therapy. Phys Ther 73:771–786
Staerkle R, Mannion AF, Elfering A, Junge A, Semmer NK, Jacobshagen N, Grob D, Dvorak J, Boos N (2004) Longitudinal validation of the fear-avoidance beliefs questionnaire (FABQ) in a Swiss–German sample of low back pain patients. Eur Spine J 13:332–340. doi:10.1007/s00586-003-0663-3
Stone AA, Turkkan JS, Bachrach CA, Jobe JB, Kurtzman HS, Ciain VS (1999) The science of self-report: implications for research and practice. Lawrence Erlbaum Associates Incp 261 Mahwah, NJ
Strecher VJ, DeVellis BM, Becker MH, Rosenstock IM (1986) The role of self-efficacy in achieving health behavior change. Health Educ Q 13:73–92
Sullivan M, Bishop S, Pivik J (1995) The pain catastrophising scale. Development and validation. Psychol Assess 7:524–532. doi:10.1037/1040-3590.7.4.524
Turner JA, Jensen MP, Romano JM (2000) Do beliefs, coping, and catastrophizing independently predict functioning in patients with chronic pain? Pain 85:115–125. doi:10.1016/S0304-3959(99)00259-6
van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Laerum E, Malmivaara A (2006) Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15(Suppl 2):S169–S191. doi:10.1007/s00586-006-1071-2
Vlaeyen JW, Linton SJ (2000) Fear avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain 85:317–332. doi:10.1016/S0304-3959(99)00242-0
Waddell G (1999) The back pain revolution. Churchill Livingstone, London
Waddell G, Newton M, Henderson I, Somerville D, Main CJ (1993) A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 52:157–168. doi:10.1016/0304-3959(93)90127-B
Wallston KA, Wallston BS, Devellis R (1978) Development of multidimensional health locus of control (MHLC) scales. Health Educ Monogr 6:160–170
Wessels T, van Tulder M, Sigl T, Ewert T, Limm H, Stucki G (2006) What predicts outcome in non-operative treatments of chronic low back pain? A systematic review. Eur Spine J 15:1633–1644
Woby SR, Watson PJ, Roach NK, Urmston M (2004) Adjustment to chronic low back pain–the relative influence of fear-avoidance beliefs, catastrophizing, and appraisals of control. Behav Res Ther 42:761–774. doi:10.1016/S0005-7967(03)00195-5
Acknowledgments
This study was supported by a grant from the Swiss National Research Program NRP 53 “Musculoskeletal Health–Chronic Pain” of the Swiss National Science Foundation (Project 405340-104787/2) and the Schulthess Klinik Research Funds. We would like to express our thanks to: Prof Beat A. Michel for providing the infrastructure to carry out this work within the Department of Rheumatology and Institute of Physical Medicine, University Hospital Zürich, Switzerland; Filomena Caporaso, Deborah Gubler and Valeriu Toma for their assistance with the data collection; the physiotherapists Martin Litschi, Tamar Bon, Konstanze Wagner, Elfi Raffainer, Luca Scascighini, Raymond Denzler, Wiebke Schubien, Manuela Meier, Melanie Knecht, Selina Bühler, Christina Gruber and Diana Brun-Walser for treating the patients and completing the necessary documentation; Doctors Bischoff, Camenzind, Distler, Haltinner, Klipstein, Rörig, Schmidt, Sprott, Stärkle-Bär, Tamborrini, Thoma, Zimmermann (USZ), Bartanusz, Kramers-de Quervain, Marx, Pihan (Schulthess Klinik), Brunner (Balgrist), Kern, Kurmann, Schuler, Stössel and Zoller (GP practices) for referring patients to the study; all the patients who took part in the study; and Britton Brewer for his advice with regard to the adherence measures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mannion, A.F., Helbling, D., Pulkovski, N. et al. Spinal segmental stabilisation exercises for chronic low back pain: programme adherence and its influence on clinical outcome. Eur Spine J 18, 1881–1891 (2009). https://doi.org/10.1007/s00586-009-1093-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-009-1093-7