
Abstract
This is an experimental study on human cadaver spines. The objective of this study is to compare the pullout forces between three screw augmentation methods and two different screw designs. Surgical interventions of patients with osteoporosis increase following the epidemiological development. Biomechanically the pedicle provides the strongest screw fixation in healthy bone, whereas in osteoporosis all areas of the vertebra are affected by the disease. This explains the high screw failure rates in those patients. Therefore PMMA augmentation of screws is often mandatory. This study involved investigation of the pullout forces of augmented transpedicular screws in five human lumbar spines (L1–L4). Each spine was treated with four different methods: non-augmented unperforated (solid) screw, perforated screw with vertebroplasty augmentation, solid screw with vertebroplasty augmentation and solid screw with balloon kyphoplasty augmentation. Screws were augmented with Polymethylmethacrylate (PMMA). The pullout forces were measured for each treatment with an Instron testing device. The bone mineral density was measured for each vertebra with Micro-CT. The statistical analysis was performed with a two-sided independent student t test. Forty screws (10 per group and level) were inserted. The vertebroplasty-augmented screws showed a significant higher pullout force (mean 918.5 N, P = 0.001) than control (mean 51 N), the balloon kyphoplasty group did not improve the pullout force significantly (mean 781 N, P > 0.05). However, leakage occurred in some cases treated with perforated screws. All spines showed osteoporosis on Micro-CT. Vertebroplasty-augmented screws, augmentation of perforated screws and balloon kyphoplasty augmented screws show higher pullout resistance than non-augmented screws. Significant higher pullout forces were only reached in the vertebroplasty augmented vertebra. The perforated screw design led to epidural leakage due to the position of the perforation in the screw. The position of the most proximal perforation is critical, depending on screw design and proper insertion depth. Nevertheless, using a properly designed perforated screw will facilitate augmentation and instrumentation in osteoporotic spines.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
An increasingly elderly population in industrial countries is a well-known problem to societies and health services. In 2050, 54% of the population will be older than 65 years in countries with a human development index >0.9 [7, 31]. This epidemiological trend is resulting in increased numbers of patients with age related orthopedic diseases such as osteoporosis or degenerative scoliosis [12, 14, 21, 39]. Scoliotic deformities are prevalent in 36–48% of osteoporotic women and worsened by osteoporotic vertebral fractures. Adult scoliotic patients have a reduced bone stock, which may result in fractures or increased decompensation of the scoliotic curve [8, 14].
Increased patient numbers results in increased operation numbers. Indications for open surgery with screw stabilization in osteoporotic patients are spinal imbalances after fracture, tumors, instability, multisegmental spinal stenosis and neurological deficits warranting open decompression. The treatment goal for these diseases is, next to an adequate decompression in the case of neurological deficit, the achievement of a balanced and stable spine [19].
Polymethylmethacrylate (PMMA) augmentation is regarded as an efficient way to enhance screw strength in osteoporotic bones [10, 26]. Although vertebroplasty (VP) and balloon kyphoplasty (BKP) are generally used for vertebral body stabilization, they are also becoming more popular in screw augmentation [25, 36]. In both the techniques, cement is injected prior to screw insertion; in balloon kyphoplasty, a balloon is used to create a void which is filled with PMMA, whilst in vertebroplasty PMMA is injected directly into the vertebral body. The pedicle screw is then inserted into the cement in order to enhance its strength.
Further developments include expandable screws with augmentation or perforated screws [6]. Perforated screws are mainly based on cannulated screw for percutaneous placement [33]. The adjustments for cement injection include lateral slots or holes at the distal end of the screw to allow an even cement distribution throughout the vertebra.
The objective of our study was the comparison of the pullout forces of solid pedicle screws augmented with vertebroplasty or balloon kyphoplasty against a new technique of screw augmentation which allows injection of the cement through a perforated screw. The biomechanical behavior of the different screw designs and augmentation methods were studied in osteoporotic human cadaver spines.
Materials and methods
Five adult lumbar spines (four females, 1 male; age 72–89 years, mean 79.8 years) were treated with bilateral pedicle screws in L1–L4. Each augmented vertebra was treated bilaterally with the same augmentation technique.
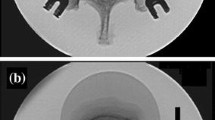
Three of four lumbar vertebrae received the solid Dualcore 6.2–50 mm pedicle screw (Click’X, Synthes Inc. Solothurn, CH) and one vertebra received the perforated Dualcore 6.2–50 mm pedicle screw optimized for bone augmentation (Click’X, Synthes, Fig. 1). The perforated screw has a central canal without a distal opening and 2 × 2 holes at 20 and 40% of the thread length from the tip. Each cadaver spine was treated with different augmenting or stabilization techniques and control resulting in ten screws per group.

Example of a perforated transpedicular screw, b cement distribution during injection and attachment of screw with luer-lock connector
The following groups were investigated and three different augmentation techniques were used to augment screws:
-
Group 1 (vertebra L1) solid screw, no augmentation (control).
-
Group 2 (vertebra L2) perforated screw/vertebroplasty (P/VP).
-
Group 3 (vertebra L3) solid screw/vertebroplasty (S/VP).
-
Group 4 (vertebra L4) solid screw/balloon kyphoplasty (S/BKP).
The placement of all screws was done purely under image intensifier on the intact lumbar spine and the vertebrae were dissected after the operative procedure. The placement was performed using a starter awl on the cortex of the pedicle and a blunt pedicle probe. All screws were inserted two-thirds of the vertebral width without tapping.
A vertebral PMMA (Vertecem, Synthes Inc, Solothurn, CH) was used for bone augmentation and 2 ml was injected per screw in the levels L2–L4 (e.g. groups 2–4).
Group 2: The perforated screws were inserted into the vertebra with the same approach as the solid screws and the cement was injected through a special adapter (Fig. 1b) with a 2-ml syringe.
Group 3: After transpedicular probing, the cement was injected bilaterally using the same bone fillers as in group 4 in a vertebroplasty technique (Kyphon Inc. Sunnyvale, USA) and the screws were placed immediately after filling.
Group 4: A standard balloon kyphoplasty technique as described by Garfin et al. [11] was performed using a 20-mm kyphoplasty balloon (Kyphon Inc. Sunnyvale, USA). The cement was injected using the bone fillers.
The cement was injected in the groups 2–4 after a minimum of 6 min after mixing. The correct viscosity was observed visually by the criteria that the cement stopped dripping off the injection cannula.
Leakage was assessed by visual examination and ap/lateral radiography.
The pullout forces were measured on an Instron universal testing machine (model 4301) with a load cell of 5 kN. The vertebra were dissected and individually attached with a vice. The screw was fixed to a screw holder and visually attached longitudinally along the axis of the screw to the load cell. The pullout tests were performed at a rate of 5 mm/min until the screw was pulled out completely. The maximum load during testing was defined as maximum failure load (e.g., pullout strength of the screw).
After testing, the histological examples of the vertebra were examined by micro-CT in order to evaluate the osteoporosis. Micro-CT was performed with 340 slices; the overall bone mineral density (BMD) was calculated along three different depths (slice 1–100, 100–200 and 200–300 at a resolution of 17 μm in all dimensions) .
The statistical analysis was performed using the F test for equality of variance followed by two-sided independent student t tests. To correct for multiple testing, the t tests were performed at the 1.7% level of significance (Bonferroni correction).
The BMD per vertebra was analyzed as mean of the three different depths. The BMD adapted pullout forces were calculated based on the difference from the overall mean BMD in the sample group (Table 1) and a BMD adapted statistical analysis was performed based on the relative difference from the overall BMD.
The primary endpoint of this study was the screw strength regarding pullout forces. Secondary endpoints included the injection characteristics and leakage.
Results
A total of 20 lumbar vertebrae were stabilized with 40 screws (10 screws per group). The mean pullout forces were 513 ± 214 N in group 1 (control), 917 ± 253 N in group 2 (P/VP), 920 ± 268 N in group 3 (S/VP) and 781 ± 349 N in group 4 (S/BKP, Fig. 2). The overall and the individual analysis of the pullout forces (Figs. 3, 4) were significantly higher in groups 2 and 3 relative to the control (P = 0.001; Table 2). The balloon kyphoplasty group could not show a significantly higher strength than the control (P > 0.05). Furthermore, no statistical difference (P between 0.33 and 0.97) was found between the treatment groups (groups 2–4).

Overall pullout forces of Group 1 (control), Group 2 [perforated screw/vertebroplasty (VP)], Group 3 (solid screw/vertebroplasty) and Group 4 [solid screw/balloon kyphoplasty (BKP)]

Mean pullout forces of two screws of the five spinal specimens separately

Example of pullout-force recording of right and left screws (control group)
The histological analysis with micro-CT (Table 1) showed an overall mean bone density of 830 ± 27 mg HA/cm3 per vertebra and a mean bone volume to tissue volume (BV/TV) ratio of 0.09. As all specimens had a different BMD, the pullout forces were adapted to the BMD based on the mean BMD. The non-adapted and the BMD-adapted overall values are shown in Table 2. Statistically, the evaluation of the non-BMD adapted results and BMD-adapted results was similar.
The injection through the perforated screw was uneventful and easy to perform. It was possible to inject the required amount of PMMA (2 ml/pedicle) in all vertebrae. However, the post-op radiography and the intraoperative visual control showed a posterior leakage in two cases of group 2 (P/VP). Leakage occurred exclusively into the epidural veins (Fig. 5).

Example of instrumented spine (L2–L4) with the three investigational groups. P/VP Perforated screw, vertebroplasty, S/VP solid screw/vertebroplasty, S/BKP solid screw/balloon kyphoplasty. Note the different cement distribution between P/VP and S/VP or S/BKP. Cement leakage in L2 (arrow)
In group 2, the cement was inserted generally much more posterior than in group 3 or group 4.
After the pullout, the visual inspection of the solid screws showed incorporation into the cement mantle in balloon kyphoplasty and vertebroplasty, whereas the perforated screw could be clearly stripped out of the cement mantle (Fig. 6).

Example of screws after experiment. Screws of group 2 a showed no cement mantle. b Represents a screw from group 3, and c from group 4
Discussion
PMMA augmentation is regarded as the best method to enhance screw strength significantly in osteoporotic bones [10, 26, 30, 32, 41, 43]. Although PMMA was primarily used for pelvic surgery, special changes were made to meet the needs of spinal surgery. Today PMMAs used in spinal surgery are radioopaque and have a reduced exothermic polymerization reaction to reduce tissue necrosis and nerve damage in the case of leakage [1].
The cementing techniques enhance the fixation of the screw within the vertebral body transferring the biomechanical load anteriorly from the pedicle to the vertebral body. Screw augmentation with PMMA cement is indicated in osteoporotic cases requiring instrumentation such as instability, neurological damage, multisegmental decompression or degenerative scoliosis. The application of PMMA augmented screws also allows a shorter fusion segment compared to non-augmented screws. Furthermore, also the strength of anterior implants can be enhanced in osteoporotic bone by posterior screw augmentation [37].
Two cementing techniques, vertebroplasty and balloon kyphoplasty, for stabilization of a vertebra are currently in clinical use. Vertebroplasty is furthermore used for augmenting transpedicular screws showing the above-mentioned results [10, 30, 32, 41, 43]. Balloon kyphoplasty is generally used for reduction of vertebral fracture. The void created by the balloon can be either filled with PMMA or resorbable bone cements [2, 26–28, 38]. Vertebroplasty has considerable risks regarding cement leakage and a slightly higher perioperative morbidity than balloon kyphoplasty [38]. Therefore surgeons may favor balloon kyphoplasty for screw augmentation to minimize these risks. However, clinical experience, familiarity with both the procedures and the large price difference between both the techniques may influence the general use of balloon kyphoplasty in augmentation procedures.
Alternative techniques to enhance the strength of the implants are techniques combining sublaminar hooks, wires, conical screws, iliac screws or expandable screws [6, 35, 43]. These techniques not only show a higher strength than transpedicular screws alone in osteoporosis, but also have inherent risks [5, 13, 32].
Several studies have confirmed that screws in osteoporotic spines have a significant lower-screw strength with more frequent screw movements within the vertebra than normal spines [5, 13, 23, 29, 35] leading to overall higher failure rates of up to 12% [2, 26, 41].
However, PMMA augmentation of screws has shown to provide higher strength than all alternative techniques [9, 30, 41, 43]. A possible further advantage of additional adjacent segment augmentation has been discussed with the potential of reducing adjacent vertebral fractures [15].
The insertion depth of the screw plays a significant role. Screws implanted deeper than 50% into the vertebral body or bicortical screws perforating the anterior vertebral cortex enhance screw anchorage in the bone [11, 22, 42]. We observed those rules and inserted the screws as shown in Fig. 5. However, bicortical fixation was avoided because of the anterior leakage risk.
Finally the diameter of the screws plays a role in normal bone, screws with diameters 7 mm and higher show better strength. In osteoporotic bone, such screws may cause pedicle fractures in 24–40% of cases, leading to screw failure [3, 43]. Therefore we used only 6.2-mm screws in our study.
As shown above, larger screw diameters can lead to pedicle fractures in osteoporotic bone. This leaves the question whether the primary strength of a screw in osteoporosis can be compared to the strength in healthy bone.
In a non-osteoporotic spine, screw anchorage in an intact and healthy pedicle assures 80% craniocaudal stiffness and 60% pullout force. By inserting the screw into a healthy vertebra, the pullout force can be further enhanced by 20% and by another 20% using bicortical fixation [18, 40].
Furthermore, the bone density of healthy vertebral bodies is six times lower than that in the pedicle overall. The trabecular pedicular bone, however, is only twice as stiff as the vertebral trabecular bone and the cortical pedicular bone is eight times stiffer than the trabecular vertebral bone, hence the need of pedicular fixation of screws. But in osteoporosis, the trabecular and cortical pedicular bone can be reduced by up to 50% versus a healthy bone and may therefore not be able to provide the required strength [18].
Taking this fact into account and the above-mentioned fact that screws with diameter 7 mm and higher may break the pedicle in case of osteoporosis, we could not rule out pedicle perforation with the 6.2-mm screws and therefore avoided cement injection into the area of the pedicle. Furthermore, the screws are designed such that, if inserted at the required depth, all of the perforations lie well within the vertebra and none in the pedicle. Finally it has been described that no tapping is to be preferred for screw stability [43], which we considered in our study.
The results of our study reflect the results of those studies regarding the concept of screw augmentation; we could enhance the screw strength by 1.8 in the vertebroplasty groups and 1.5 in the balloon kyphoplasty group. We tried to simulate clinical conditions and inserted bilateral screws with the same augmentation technique always in one vertebra and treated all spines with all different augmentation procedures. We found no difference between the uses of perforated and not perforated screws regarding the pullout forces of the screws, although the screws after the pullout looked different (Fig. 6). This might be an advantage in the case of loosening in order to avoid large defects of the bone by the dislocation of the screw with an intact cement mantle.
In our study, leakage occurred in two cases in group 2, which can be due to the positioning of the lateral holes. In assessing the images, 50% of the screw itself was fixed within the pedicle and 50% of the screw within the vertebral body. The insertion of the screw was consistently performed to maximize anchorage within the vertebral body, e.g., 80% of the vertebral depth. It is possible, that the perforations of the screw lie directly attached or within a venous vessel allowing a posterior leakage via the basovertebral vein into the epidural space and veins. This has to be considered during screw insertion. Furthermore, it is important to specify the operation technique and aim to insert the screws at the 20%/80% limit of the vertebral depth. This deep implantation is important to avoid a positioning of the perforations within the pedicle which then, in the case of a pedicle perforation, can easily lead to leakage into the spinal canal. We did not observe any anterior leakage of cement in our study.
Nevertheless, a perforated screw has handling advantages. The injection of PMMA cement through perforated screws is technically easier than performing a vertebroplasty or balloon kyphoplasty and inserting a screw into the cement. In first positioning of the perforated screw, the position can be verified and, if needed, optimized. After vertebroplasty or balloon kyphoplasty, there remains a risk of dislocation or misalignment of the screw during insertion into the cement. It is furthermore possible to first position the screws on several segments and then to perform an augmentation of those screws simultaneously; a simultaneous multisegmental approach is more difficult in vertebroplasty and nearly impossible in a balloon kyphoplasty.
The screw strength after balloon kyphoplasty was 1.5 times higher than that of the control according to the literature [4, 25], but just failed to reach significance in our study. This may be due to the fact that we injected an equal amount of PMMA cement in all groups. In the balloon kyphoplasty group, the balloon was inflated to 2 ml and 2 ml was injected. The balloon itself creates a void, with an impactation of the surrounding trabeculae and may therefore prevent cement penetration into the surrounding bone. It is obvious, that the injection of an amount of cement, which just fills the void, does not have the same interdigitation as a vertebroplasty. Therefore, it is possible that the injection of more cement might have led to better results; however, it would have biased the study towards balloon kyphoplasty. A study investigating the pul-out behavior of screws, augmented with different amounts of cement found no increase of strength after the injection of more cement [9]. A different study design investigated the behavior of a 4 ml cement augmentation with balloon kyphoplasty versus a 2 ml cement augmentation of vertebroplasty and found a significant higher stability in balloon kyphoplasty [4]. This study injected a vertebra with two different augmenting methods and can therefore not be compared to our study. A different study, investigating the bilateral augmentation of pedicle screws with balloon kyphoplasty versus a non-augmented control found a significant higher strength towards the non- augmented control [25]. The same group documented furthermore a higher strength of solid anterior screws augmented with balloon kyphoplasty towards a non-augmented control [24].
All our specimens were in the reported range of osteoporosis [20]. The BMD differences were marginal, which explains that the BMD did not have a significant impact on the pullout results. As it has been shown that BV/TV values give a better idea about osteoporosis and are the best values regarding stability of the vertebra [20], we analysed those values as well showing that all specimen were osteoporotic. However, a Micro CT analysis of a slice of a vertebra does not reflect the overall BV/TV ratio as they vary depending on the vertebral region [20]. To minimize a bias, we sampled out bone from the intact and non-augmented central region of the vertebra.
We used non-resorbable PMMA cement developed for vertebroplasty augmentation in our study. The discussion whether resorbable calcium phosphate cements (CPC) result in a higher strength than PMMA is still going on.
Both the substances have shown in various studies to enhance screw stiffness; PMMA up to 49–162% and CPC up to 102% [28, 30, 37, 41, 43]. Therefore, it seems that both the substances can be used in normal bone to enhance screw strength.
There are several limitations to this study. As mentioned in other comparable studies, the pullout forces do not reflect the real biomechanics in situ and can be influenced by various factors, such as diameter of the screws, pitch distance and partially or fully threaded screws [17, 29, 34]. We tried to rule out most of those parameters using the same fully threaded screw and inserted the screw perpendicular to the superior endplates. Although the biomechanics in vivo are different, a comparison of different augmentation techniques with the same biomechanical model is in our opinion acceptable.
In order to avoid intraindividual bone stock differences, we treated every spine with all four different stabilization techniques. However, we always treated the same vertebra with the same stabilization technique, so differences in the pedicle diameter and the size of the vertebra could influence the outcome to some extend. In osteoporosis, the screw strength in the pedicle is significantly reduced to a healthy spine; therefore we believe that pedicle size had only a small impact in our model [7, 18]. Furthermore, it has also been demonstrated in biomechanical studies that pedicle size has no impact on the pullout force [16]. Nevertheless, we tried to challenge the treatment effect using the smallest diameter and therefore strongest pedicle (L1) as control.
We also did not measure the injection time as the injection time is clinically not as important as the precise injection viscosity; therefore we strictly adhered to the parameters to inject the PMMA cement not earlier than 6 min after mixing. In the future, a more correct analysis of the viscosity should be possible with the use of a viscosimeter, which is being currently developed. Whether a leakage could have been avoided using a viscosimeter remains still unknown.
Furthermore, the implantation technique may vary slightly; small aberrations/angulations differences during implantation technique or a different local bone stock within the body and pedicle may lead to different results (Fig. 4), therefore all screws were assessed separately in the statistical analysis.
Conclusion
The pullout strength of a solid and perforated Dualcore transpedicular screw can be significantly enhanced by vertebroplasty. Balloon kyphoplasty augmentation is not superior to vertebroplasty augmentation. The new perforated Dualcore screw allows for an easier operation with considerable intraoperative advantages.
An accurate implantation technique and cement handling technique of the perforated screw is necessary in order avoid cement leakage into local vessels.
References
Belkoff SM, Molloy S (2003) Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine 28(14):1555–1559. doi:10.1097/00007632-200307150-00015
Bohner M (2008) Injectable cements for vertebroplatsy and kyphoplasty. In: Becker S, Ogon M (eds) Balloon kyphoplasty. Springer Wien, New York, pp 143–149
Brantley AG, Mayfield JK, Koeneman JB, Clark KR (1994) The effects of pedicle screw fit. An in vitro study. Spine 1 19(15):1752–1758
Burval DJ, McLain RF, Milks R, Inceoglu S (2007) Primary pedicle screw augmentation in osteoporotic lumbar vertebrae: biomechanical analysis of pedicle fixation strength. Spine 1 32(10):1077–1083
Coe JD, Warden KE, Herzig MA, McAfee PC (1990) Influence of bone mineral density on the fixation of thoracolumbar implants. A comparative study of transpedicular screws, laminar hooks, and spinous process wires. Spine 15(9):902–907. doi:10.1097/00007632-199009000-00012
Cook SD, Salkeld SL, Stanley T, Faciane A, Miller SD (2004) Biomechanical study of pedicle screw fixation in severely osteoporotic bone. Spine J 4(4):402–408. doi:10.1016/j.spinee.2003.11.010
Crafts NFR (1997) The human development index and changes in standards of living: some historical comparisons. Eur Rev Econ Hist 1:299–322
DeWald CJ, Stanley T (2006) Instrumentation-related complications of multilevel fusions for adult spinal deformity patients over age 65: surgical considerations and treatment options in patients with poor bone quality. Spine 1 31(19 Suppl):144–151
Frankel BM, D’Agostino S, Wang C (2007) A biomechanical cadaveric analysis of polymethylmethacrylate-augmented pedicle screw fixation. J Neurosurg Spine 7(1):47–53. doi:10.3171/SPI-07/07/047
Frankel BM, Jones T, Wang C (2007) Segmental polymethylmethacrylate-augmented pedicle screw fixation in patients with bone softening caused by osteoporosis and metastatic tumor involvement: a clinical evaluation. Neurosurgery 61(3):531–537
Garfin SR, Hansen A, Reiley MA (2001) New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 26(14):1511–1515. doi:10.1097/00007632-200107150-00002
Grubb SA, Lipscomb HJ, Coonrad RW (1988) Degenerative adult onset scoliosis. Spine 13(3):241–245. doi:10.1097/00007632-198803000-00004
Halvorson TL, Kelley LA, Thomas KA, Whitecloud TS 3rd, Cook SD (1994) Effects of bone mineral density on pedicle screw fixation. Spine 1 19(21):2415–2420
Healey JH, Vigorita VJ, Lane JM (1985) The coexistence and characteristics of osteoarthritis and osteoporosis. J Bone Joint Surg 67-A:586–592
Heini PF (2005) The current treatment—a survey of osteoporotic fracture treatment. Osteoporotic spine fractures: the spine surgeon’s perspective. Osteoporos Int 16(Suppl 2):85–92. doi:10.1007/s00198-004-1723-1
Herzig M Das Festigkeitsverhalten transpedikulärer Fixationssysteme für die lumbale Wirbelsäule im zyklisch-dynamischen Dauerversuch (2004) German National Library. http://deposit.ddb.de/cgi-bin/dokserv?idn=971004986urn:nbn:de:hbz:061-20040418-000797-5. Accessed Jan 2008
Hilibrand AS, Moore DC, Graziano GP (1996) The role of pediculolaminar fixation in compromised pedicle bone. Spine 21(4):445–451
Hirano T, Hasegawa K, Takahashi HE, Uchiyama S, Hara T, Washio T, Sugiura T, Yokaichiya M, Ikeda M (1997) Structural characteristics of the pedicle and its role in screw stability. Spine 22(21):2504–2509
Hu SS (1997) Internal fixation in the osteoporotic spine. Spine 22(24 Suppl):43–48
Hulme PA, Boyd SK, Ferguson SJ (2007) Regional variation in vertebral bone morphology and its contribution to vertebral fracture strength. Bone 41(6):946–957. doi:10.1016/j.bone.2007.08.019
Kanis JA, Pitt FA (1992) Epidemiology of osteoporosis. Bone 13(Suppl 1):S7–S15. doi:10.1016/8756-3282(92)90189-4
Krag MH, Beynnon BD, Pope MH, Frymoyer JW, Haugh LD, Weaver DL (1986) An internal fixator for posterior application to short segments of the thoracic, lumbar, or lumbosacral spine. Design and testing. Clin Orthop Relat Res 203:75–98
Law M, Tencer AF, Anderson PA (1993) Caudo-cephalad loading of pedicle screws: mechanisms of loosening and methods of augmentation. Spine 18(16):2438–2443. doi:10.1097/00007632-199312000-00012
Linhardt O, Lüring C, Matussek J, Hamberger C, Herold T, Plitz W et al (2006) Stability of anterior vertebral body screws after kyphoplasty augmentation. An experimental study to compare anterior vertebral body screw fixation in soft and cured kyphoplasty cement. Int Orthop 30(5):366–370. doi:10.1007/s00264-006-0100-4
Linhardt O, Lüring C, Matussek J, Hamberger C, Plitz W, Grifka J (2006) Stability of pedicle screws after kyphoplasty augmentation: an experimental study to compare transpedicular screw fixation in soft and cured kyphoplasty cement. J Spinal Disord Tech 19(2):87–91. doi:10.1097/01.bsd.0000177212.52583.bd
Lonstein JE, Denis F, Perra JH, Pinto MR, Smith MD, Winter RB (1999) Complications associated with pedicle screws. J Bone Joint Surg Am 81(11):1519–1528
Maestretti G, Cremer C, Otten P, Jakob RP (2007) Prospective study of standalone balloon kyphoplasty with calcium phosphate cement augmentation in traumatic fractures. Eur Spine J 16(5):601–610. doi:10.1007/s00586-006-0258-x
Moore DC, Maitra RS, Farjo LA, Graziano GP, Goldstein SA (1997) Restoration of pedicle screw fixation with an in situ setting calcium phosphate cement. Spine 22(15):1696–1705
Okuyama K, Abe E, Suzuki T, Tamura Y, Chiba M, Sato K (2001) Influence of bone mineral density on pedicle screw fixation: a study of pedicle screw fixation augmenting posterior lumbar interbody fusion in elderly patients. Spine J 1(6):402–407. doi:10.1016/S1529-9430(01)00078-X
Pfeifer BA, Krag MH, Johnson C (1994) Repair of failed transpedicle screw fixation. A biomechanical study comparing polymethylmethacrylate, milled bone, and matchstick bone reconstruction. Spine 19(3):350–353
Riggs BL, Melton LJ 3rd (1995) The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 17(5 Suppl):505–511. doi:10.1016/8756-3282(95)00258-4
Sarzier JS, Evans AJ, Cahill DW (2002) Increased pedicle screw pullout strength with vertebroplasty augmentation in osteoporotic spines. Neurosurg 96(3 Suppl):309–312
Schizas C, Michel J, Kosmopoulos V, Theumann N (2007) Computer tomography assessment of pedicle screw insertion in percutaneous posterior transpedicular stabilization. Eur Spine J 16:613–617. doi:10.1007/s00586-006-0221-x
Skinner R, Maybee J, Transfeldt E, Venter R, Chalmers W (1990) Experimental pullout testing and comparison of variables in transpedicular screw fixation. A biomechanical study. Spine 15(3):195–201. doi:10.1097/00007632-199003000-00007
Soshi S, Shiba R, Kondo H, Murota K (1991) An experimental study on transpedicular screw fixation in relation to osteoporosis of the lumbar spine. Spine 16(11):1335–1341. doi:10.1097/00007632-199111000-00015
Takigawa T, Tanaka M, Konishi H, Ikuma H, Misawa H, Sugimoto Y et al (2007) Comparative biomechanical analysis of an improved novel pedicle screw with sheath and bone cement. J Spinal Disord Tech 20(6):462–467. doi:10.1097/BSD.0b013e318030d2d6
Tan JS, Bailey CS, Dvorak MF, Fisher CG, Cripton PA, Oxland TR (2007) Cement augmentation of vertebral screws enhances the interface strength between interbody device and vertebral body. Spine 1 32(3):334–341
Taylor RS, Taylor RJ, Fritzell P (2006) Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine 31(23):2747–2755
Vanderpool DW, James JI, Wynne-Davies R (1969) Scoliosis in the elderly. J Bone Joint Surg Am 51(3):446–455
Weinstein JN, Rydevik BL, Rauschning W (1992) Anatomic and technical considerations of pedicle screw fixation. Clin Orthop Relat Res (284):34–46
Wittenberg RH, Lee KS, Shea M, White AA 3rd, Hayes WC (1993) Effect of screw diameter, insertion technique, and bone cement augmentation of pedicular screw fixation strength. Clin Orthop Relat Res 296:278–287
Zdeblick TA, Kunz DN, Cooke ME, McCabe R (1993) Pedicle screw pullout strength. Correlation with insertional torque. Spine 18(12):1673–1676
Zindrick MR, Wiltse LL, Widell EH, Thomas JC, Holland WR, Field BT et al (1986) A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop Relat Res 203:99–112
Acknowledgments
The authors thank several people for their contribution and advice for this work: G. Zanoni from the Ludwig Boltzmann Institute for Experimental and Clinical Traumatology, Vienna; I. Boecken, D. Beer, R. Egger and B. Schenk, Synthes, Bettlach, Switzerland and L. Kaufman, Vrije Universiteit Brussel, Belgium for advising on the statistical analysis. The study was financed from a grant from Synthes (Bettlach, Switzerland).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Becker, S., Chavanne, A., Spitaler, R. et al. Assessment of different screw augmentation techniques and screw designs in osteoporotic spines. Eur Spine J 17, 1462–1469 (2008). https://doi.org/10.1007/s00586-008-0769-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-008-0769-8