
Abstract
The aim of this study is to evaluate the efficacy and safety of balloon kyphoplasty (BK) in the management of vertebral compression fractures (VCFs). This study is based on a systematic review of the literature (until October 2004) and meta-analysis of clinical studies assessing the efficacy and safety of BK in the treatment of VCFs. Estimates of effect were based on a random effects model. Meta-regression analyses were carried out where required. A total of 26 studies met the inclusion criteria. Although studies displayed considerable methodological limitations, the results of the clinical series indicate significant improvements in pain intensity, vertebral height, sagittal alignment, functional capacity, and quality of life. Compared with conventional medical management, BK afforded significant improvement in pain intensity and mobility. Likewise, a significant reduction was observed in vertebral collapse, kyphotic deformity, the development of new vertebral fractures, and hospital stay. Compared with vertebroplasty, the technique reduced the loss of height and the degree of kyphotic deformity, and afforded a significantly lower leakage rate—with no differences in relation to other variables. Regarding adverse effects, leakage affected 7% of all levels treated, while complications were recorded in 2% of the patients, and new vertebral fractures in 16%. The available evidence suggests that BK can be effective and safe in application to VCFs. However, existing studies evince substantial methodological limitations and relatively short follow-up periods. Better clinical research is required to determine the capacity of BK to avoid the functional and physiological sequelae of VCFs and to define the true role of the technique among the existing therapeutic options.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The growing prevalence of vertebral compression fractures (VCFs) [44, 52], the confirmation of their serious physiological, functional, and psychological repercussions [23, 32, 38, 46, 48], and a large number of patients’ refractory to habitual treatment [38, 39, 50] have favored the development of minimally invasive surgical techniques such as balloon kyphoplasty (BK)—the aim of which is not only to improve the patient symptoms but also to reduce the biomechanical alterations of the spine produced by fracture, thereby avoiding its long-term consequences [2, 19, 40, 60].
The term “kyphoplasty” was introduced by Kyphon Inc. to describe balloon-assisted vertebroplasty. The technique is carried out in the operating room by means of a specific fracture reduction system (The KyphX®, Kyphon Inc.), and comprises several phases: trans- or extrapedicular bone access until reaching the vertebral body; placement of the inflatable bone impactor within the bone; balloon insufflation under manometric control, elevating the vertebral plate, and creating a cavity within the vertebral body; balloon deflation and filling of the cavity with viscous radiopaque bone cement under low pressure (PMMA KyphX®) through a bone filling device to stabilize the fracture.
The procedure was first used in 1998, and unlike vertebroplasty, it aims not only to secure fracture fixation and stabilization but also to reconstruct the vertebral anatomy and correct the spinal deformity, with the aim of avoiding the medical sequelae of VCFs. While BK has been introduced to clinical practice, no firm conclusions have yet been drawn as to the efficacy and safety of the technique [24, 36, 54]. For this reason, and considering the rate at which the procedure is being diffused and incorporated to clinical practice, the present systematic review aims to analyze the collected body of evidence regarding the efficacy and safety on BK in the treatment of VCFs.
Methods
For the identification of studies, we performed a systematic review of the literature up until October 2004, involving the following databases: Medline (WebSPIRS, SilverPlatter); CINAHL (WebSPIRS); CC Search Life/Clin, Pollution & Toxicology; The Cochrane Library; Serline: Biomedical Journals; Science citation index expanded (sci-expanded), INAHTA (NHS, DARE, EED, HTA). The search strategy has been: #1: (kyphoplasty) or (vertebroplasty), #2: (fracture*) or (vertebra*) or (osteop*) or (tumor*), #3: #1 and #2. Likewise, bibliographies of relevant articles were manually examined for additional studies and the industry has been contacted to identify still unpublished material. There were no language restrictions. However, we explicitly excluded proceedings of meetings or congresses.
Selection of studies
All articles identified were evaluated by two reviewers. For inclusion, the studies were required to meet the following criteria: (a) design: studies conducted in ten or more patients that contained relevant primary clinical data. Since the aim was to analyze the available clinical evidence on BK, no other limitations were imposed—inclusion being made of both experimental and observational designs [45]; (b) population: patients with VCFs of osteoporotic and/or tumoral origin; (c) intervention: BK; (d) comparator: any other medical or surgical procedure; (e) outcomes: the studies were required to include quantitative information relating to at least one of the following primary interest variables: pain, vertebral height, kyphotic deformity, functional capacity, quality of life (QoL), cement material leakage, complications, and the development of new vertebral fractures. The use of health care resources was included as a secondary variable.
The studies that met the inclusion criteria were exhaustively and independently examined by two reviewers to discard publication duplicity or redundancy. During the trial selection and data extraction, we were not masked to authors, institutions, journal, or interventions assessed.
Quality assessment
Methodological quality and grade of scientific evidence was evaluated for each selected paper using previously validated recommendations [37]. The possible presence of systematic errors has been analyzed following the recommendations of the Cochrane Collaboration [7].
Data analysis
The principal characteristics of each of the studies included are detailed in the corresponding tables. To obtain a global measure of the effect of BK upon the variables of interest, use was made of meta-analytical techniques based on the Intercooled Stata 8 program (StataCorp LP Texas USA 1984–2005). The studies were combined according to their clinical homogeneity and outcome measures [16], using a random effects model. Prior to inclusion, we confirmed that all variables were comparable and adequate. The estimation of effect is expressed, in the case of dichotomous variables, as an Odds Ratio (OR) (with a 95% confidence interval, 95% CI) or as a proportion with its corresponding 95% confidence interval. In the case of continuous variables, the estimation of effect is expressed as the difference of means (WMD with 95% CI) between the values at baseline and after BK—estimating the difference of variances by standard formulas [47]. When the original study failed to provide the standard deviation of a continuous variable, it was estimated from the publication data (range or P value) [47]. When the original study provided standard error instead of standard deviation, this was calculated using ordinary formulas.
Statistical heterogeneity was analyzed by means of the χ 2 statistic. The potential reasons for heterogeneity were explored by meta-regression techniques using as analytical variables the etiology of VCF, its estimated age, and the duration of the follow-up period. In those cases where because of the study characteristics or the way in which the results were expressed it proved impossible to apply meta-analytical procedures, an individual analysis was carried out. Results were deemed significant at a value of P<0.05. Because of their limitations and potential misleading results [51], funnel plots were not used to analyze the possibility of publication bias.
Results
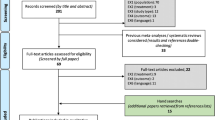
Figure 1 summarizes the search for relevant studies, the excluded studies, and the studies finally included after eliminating the redundancies attributable to the use of several databases. No studies were found that formally analyzed the costs related to BK.

Study selection and inclusion process
Of the studies located, 26 satisfied the inclusion criteria. Of these, 25 have been published in complete form, and one [15] consists of the case registry corresponding to the formulas submitted to the United States Food and Drug Administration (FDA) (510 kd). This latter study was supplied by the company that owns the system (Kyphon Inc.) without any restrictions on the content of the manuscript.
The 21 noncomparative studies include 1,490 patients and 2,637 treated levels. Five studies [11, 25, 41, 56] are comparative and include 220 patients, of which 118 were subjected to BK. Although the number of VCFs per patient is not uniform, most studies involve only a single procedure per patient (generally under general anesthesia). The population mostly comprises women over 65 years of age with painful VCFs secondary to osteoporosis and/or multiple myeloma and located between T4 and L5. The individual characteristics of studies are shown in Tables 1 and 2.
Quality assessment of studies is presented in Tables 3 and 4. These are studies with observational designs (cohorts, cases and controls, and clinical series), and the evidence they provide can be regarded as corresponding to degree II–III [37]. As Tables show, the quality of studies appears to be good on the basis of some biases but only mild in terms of others [7]. Additionally, in many cases the risk of bias is unclear as the studies failed to provide methodological details. Thus, many studies make no reference to concomitant treatments in order to assess performance bias. Same lack of information is revealed as to blind or independent outcome measurement. Further, in only a minimum number of cases is it specified that evaluation is made by professionals not implicated in carrying out the procedure. In some cases the measurement instruments used are unknown. While the duration of follow-up varies from 3 to 24 months, it generally does not exceed 10–12 months—and an important number of losses are also seen during this period. In effect, in some studies [11] the final populations do not reach 20% of the patients actually treated. Only one study [25] explicitly indicates that analysis of the results is made on an intention to treat basis.
Additionally, heterogeneity was also observed in the criteria used for the selection of patients, the estimated age of the fractures, the functional class, the degree of progression of the disease, and refractoriness to previous treatments. Moreover, some studies include fractures secondary to osteoporosis and malignancy, without identification of the results corresponding to each etiological group. The time points and instruments used to assess response differ and there is no standard criterion regarding the definition of treatment response or success. Due to this lack of homogeneity, the units in which the results are expressed vary among studies (Tables 1, 2). Only exceptionally are the statistical comparisons made fitting for the baseline values of age, sex, and number of fractures, with an analysis of the lost values and the adoption of specific correction measures when performing multiple comparisons.
Efficacy
Noncomparative studies
Pain: The 18 studies that analyze this variable before and after BK report significant reductions in pain intensity that is moreover maintained during follow-up (Table 1). The combined analysis of the studies that contribute data shows that kyphoplasty affords a significant reduction in pain score using a visual analog scale (VAS) both in the postoperative period (Fig. 2) and at the end of follow-up (Table 5). The heterogeneity among studies observed in this latter case seems to be related to the duration of the follow-up period (P=0.06) in the meta-regression analysis. Likewise, the results of individual studies show that BK produces significant improvement in variables that indirectly measure pain symptoms, such as the need for opiates [10], the number of days during which pain interferes with daily life activities [15], and the number of days of bedrest because of pain [15] (Table 5).

Visual analog scale (VAS). Changes in pain score versus baseline. Results of the meta-analysis
As to the behavior of acute versus chronic vertebral fractures, the results of a single study [10] show that BK significantly and similarly reduces pain intensity in both groups (Table 1).
Vertebral height: The studies that analyze this variable report an effect significantly in favor of BK. Regarding the percentage of levels in which the technique proves able to increase vertebral height, the results of various studies [10, 13, 28, 30] yield values in the range of 70–96%.
The combined analysis of the studies that contribute data on the pre- and postoperative values shows that the technique significantly increases vertebral height regardless of the segment subjected to measure (Table 5). Figure 3 shows the combined results of ballon kyphoplasty on anterior region of vertebral body. All the studies include VCFs of osteoporotic origin, and in the meta-regression analysis it is seen that the heterogeneity among studies appears to be related to the different estimated ages of the treated fractures (P=0.005).

Mean difference in vertebral height before versus after balloon kyphoplasty: anterior region of vertebral body. Results of the meta-analysis
Various studies [10, 15] indicate that the increase in vertebral height is related to the estimated age of the VCFs—with superior results in fractures less than 2–3 months old. Thus, the results obtained by Garfin [15] indicate that in patients with a baseline loss of height equivalent to over 15% of the estimated normal value, the favorable effects of the technique only reach statistical significance in the case of fractures less than 60 days old. On the other hand, the results of a prospective study [10] specifically contrasting the results of BK in acute VCFs (defined as being less than 10 weeks old) versus chronic fractures (with an estimated age of over 4 months) show that in both cases the vertebral height is significantly greater than the preoperative height, though the degree of restitution achieved is greater in the former group (Table 1). Likewise, the data obtained indicate that in 60% of the acute fractures and in 26% of the chronic fractures, the restitution achieved exceeds 89% of the height lost (P=0.01), while in 8 and 20% of the acute and chronic fractures, respectively, the restitution obtained does not exceed 10%—no significant differences being observed between the two groups [OR (95% CI): 3 (0.75, 11.97), P=0.12].
Spinal sagittal alignment: The results of each of the nine studies [4, 10, 13, 18, 21, 42, 53, 58] that consider the absolute value of the Cobb angle show the latter to decrease after kyphoplasty, though the mean reduction varies between −1.8° and −9.9°. The combined examination of the studies [4, 10, 13, 18, 42, 53] that contribute data amenable to analysis confirms that following BK, the absolute value of this angle decreases significantly (Fig. 4). In Table 5 it can also be seen that kyphoplasty produces a significant percentage correction of the kyphotic deformity, though the number of levels that can be subjected to analysis is limited [4, 53].

Spinal sagittal alignment. Changes in absolute Cobb angle values versus baseline (°). Results of the meta-analysis
In osteoporotic VCFs, the number of levels in which the kyphotic deformity is reduced varies between 57 [42] and 85% [4]; in this context, it should be taken into account that the authors use different criteria for defining correction.
Regarding the age of VCFs, the results are divergent. Thus, while Crandall et al. [10] report similar reductions in mean kyphosis angle between acute and chronic fractures (Table 1), other investigators [4, 13, 21] indicate that the possibilities for reduction seem to be greater the younger the fractures. However, these results are difficult to evaluate, due to the limited number of cases [4] and the lack of data amenable to analysis [13, 21].
The authors of two studies indicate that the degree of reduction of the kyphotic deformity is not correlated to the level treated [4, 42] or to pain relief [4].
QoL and functional capacity: Although the instruments used to evaluate these aspects are not always described, the results of each of the studies that take such variables into account reveal evident improvements after kyphoplasty (Table 1). The combined analysis of the studies [9, 15, 30, 31] that analyze the impact of the technique upon QoL based on the SF-36 questionnaire shows (Fig. 5) that statistically significant improvements are afforded on the subscales corresponding to physical function, physical role, body pain, vitality, social function, and mental health. Although considerable statistical heterogeneity is detected among the studies, the meta-regression analysis has been unable to identify the underlying cause—no significant association being observed with any of the variables employed.

Changes in the SF-36 subscales. Results of the meta-analysis
The impact on functional capacity has been analyzed in nine studies, though two [22, 42] fail to specify the evaluation approach adopted. The results of individual studies (Table 1) show significant improvements with any of the measurement instruments used, i.e., back function index [15], the Roland–Morris disability questionnaire [43] or walking status [13, 28]. Moreover, the combined analysis of four studies [9, 13, 18, 31] with 263 patients using the Oswestry Disability Index, confirms that BK affords significant improvement [WMD (95% CI): −23.8 (−34.0, −13.55), P=0.00].
Comparative studies
BK versus conventional medical treatment
Pain: The results of each of the studies (Table 2) show significant improvements with BK both in the postoperative evaluation and during follow-up. Regarding the percentage reduction in pain intensity, the combined analysis of the studies that contribute data [25, 26, 56], with 83 and 59 patients in the of treatment and control groups, respectively, shows BK to yield a mean reduction in pain intensity 55.6% greater than that afforded by conservative management (Table 6).
The results of a study [25] indicate effects favorable to BK in relation to other variables such as the need for opiates or the number of medical visits because of pain in 6 months (Table 6).
Vertebral height: The results of a controlled study [25] show that 6 months after treatment, vertebral height increases in the patients subjected to BK and decreases in the control group—the difference being statistically significant (Table 6). However, the authors indicate that there is no significant correlation between the improvement in vertebral height and other variables such as pain relief or mobility. Komp et al. [26] reported significant differences favorable to BK—though they afford no data amenable to analysis (Table 2).
Spinal sagittal alignment: Two studies [25, 56] describe the results in relation to this variable. Weisskopf [56] found that in only 11% of the levels was it possible to correct the kyphotic deformity, though he contributed no data on its evolution in the comparator group. Kasperk [25] found that 6 months after treatment, the kyphosis angle remained relatively constant in the group subjected to BK but increased gradually in the control group—the difference between both groups being significant (Table 6).
QoL and Functional capacity: The results of Kasperk [25] show that after 6 months of follow-up, the QoL score among the patients subjected to BK is better than in the control group, although the differences did not reach the required level of significance (Table 6). The same study reports a statistically significant improvement in mobility in the group subjected to kyphoplasty (P=0.03)—though no significant correlation is observed between such improvement and the degree of recovery of vertebral height.
BK versus vertebroplasty
The results of a retrospective analysis contrasting BK versus vertebroplasty in tumoral VCFs [11] show that, globally, no significant differences are found between the two techniques in terms of pain relief [OR (95% CI): 0.89 (0.29–2.67); P=0.8] or the degree of functional improvement achieved. BK produced a significant increase (P=0.01) in vertebral height, with a mean value of 4.5±3.6 mm—which implies a 42±21% restoration of the height lost. Likewise, statistically significant improvement is observed in local kyphosis [WMD (95% CI): −5.2 (−9.71, −0.89, P=0.02]. The authors contribute no data on the degree of kyphosis or vertebral height of the levels subjected to vertebroplasty.
Safety
Filler material leakage
The analysis of the 19 studies that contribute data [4, 9, 13, 15, 18, 21, 25, 28, 30, 34, 42, 53, 56, 58] (Fig. 6) shows a total of 134 cement leakages in 1,742 treated levels, i.e., a proportion of 7.13% (95% CI: 4.83–9.42%). Of these, only two (1.5%) are described as symptomatic or cause clinical sequelae. The heterogeneity observed among the studies is associated to the etiology of VCFs (P=0.032), with a greater presence of leakage in the studies that include VCFs of osteoporotic origin [10.49% (6.23–14.7)] than in those that only consider VCFs of tumor origin [3.7% (0.5–6.8)] or both etiologies [4.4% (1.6–7.1)]. The meta-regression also revealed a possible association with the estimated age of VCFs, though the relationship did not reach statistical significance (P=0.096).

Balloon kyphoplasty. Combined analysis of bone cement leakage
In comparative studies with vertebroplasty, Fourney et al. [11] recorded no cement leakage in the levels subjected to kyphoplasty, while 9% of the levels subjected to vertebroplasty showed leakage. In turn, Phillips et al. [41], in a prospective study, reported a significantly smaller number of contrast extravasations with kyphoplasty than with vertebroplasty [OR (95% CI): .04 (.00–.68) P=0.03], as well as a significantly lesser mean score with BK in terms of contrast extravasation considered both globally and for each of the regions analyzed.
Major complications
The combined analysis of the 16 noncomparative studies that contribute data [4, 9, 13, 22, 27, 30, 34, 42, 53, 58, 59] reveals 23 complications in 1,154 patients and 1,974 levels treated—this corresponding to a complication rate of 2 and 1.16%, respectively. As can be seen in Table 7, most of the problems were of a cardiopulmonary or neurological nature. In three cases (0.26% of the patients)—comprising partial motor loss [14], epidural hematoma [14], and digestive bleeding [4]—emergency surgery was required.
In comparative studies, Komp [26] reported the presence of two cases of perforation of the fractured lamina without posterior repercussions in the group subjected to BK, while among the patients subjected to conventional medical treatment, changes in medication proved necessary in 10 of 17 patients (in eight cases because of treatment failure and in two because of intolerance). Likewise, intolerance or difficulties with the external fixation systems were reported in nine patients. On the other hand, Fourney et al. [11] reported the need for readmission to hospital due to exacerbation of heart failure in one patient 2 weeks after kyphoplasty, and the development of sudden onset of paraplegia due to progressive epidural metastasis in one patient subjected to vertebroplasty.
New vertebral fractures
Noncomparative studies: The results of eight studies [4, 12, 15, 20, 31, 42, 43] show that 87 of the 450 patients included developed new vertebral fractures during the follow-up period. The combined analysis of these studies shows (Fig. 7) that 16.5% (95% CI: 10.7–22%) of the patients suffered new vertebral fractures 1 year after treatment. There is evident heterogeneity among the studies (χ 2=20.17, P=0.00), which in the meta-regression analysis was found to be independent of the duration of follow-up (P=0.19) and the estimated age of the fractures (P=0.58), and appeared to be associated to fracture etiology (P=0.02). Thus, the studies that include only osteoporotic VCFs show a new fracture rate of 17.8% (95% CI: 11.7–24%)—this figure being clearly greater than the percentage recorded in the studies that include patients with tumor VCFs [(7.4% (95% CI): 0–17%)]. On the other hand, the results of a retrospective study involving 115 patients with osteoporotic VCFs and a follow-up duration of over three months [20] indicate that the risk of new fractures is significantly greater in the cases of secondary osteoporosis (17/35 patients vs. 9/80, P<0.001).

Noncomparative studies: incidence of new vertebral fractures
In five studies [4, 12, 20, 42] it was seen that 33 of the patients developed new fractures in levels adjacent to the treated levels, and two of these studies [12, 13] report that most such fractures occur in the first 2 months after BK.
Comparative studies: As can be seen in Table 6, the combined analysis of two studies [25, 26] indicates that patients subjected to kyphoplasty are at a significantly lesser risk of suffering new fractures 6 months after the procedure than patients in the comparator group subjected to medical management. There are no data to allow comparison of this variable between BK and vertebroplasty.
Use of health care resources
The estimated mean duration of the procedure is about 1 h per level [15, 22, 26, 53, 56, 58].
Regarding hospital stay, the great majority of studies [4, 9, 11, 14, 18, 25, 27, 30, 42, 58] report stays of between 1and 3 days after the procedure, while only 10–15% of the patients remain in hospital for more than 72 h. These latter cases are moreover attributed to the presence of disorders unrelated to the technique [4, 28].
The results of a comparative study with historical controls [56] show that hospital stay to be significantly shorter in patients subjected to BK versus conventional medical treatment [WMD: −10 (−16.7; −3.3); P=0.003], though in both cases the duration of stay was longer than reported in other studies (10.4±7.4 days in the BK group; 20.4±13.5 days in the control group).
The results of a comparative and controlled study [25] indicate that in the 6 months after BK, the number of medical visits due to pain is significantly lower than in the control group (8.6 vs. 3.3 visits/patient, P=0.01).
Discussion
The results of this review, which includes 26 studies with primary clinical data, show BK to be effective and safe for the treatment of painful VCFs of both osteoporotic and tumor origin. Likewise, there are data indicating that over the short term, BK may offer greater clinical benefits than conventional medical treatment or vertebroplasty. However, little is known of the long-term effects of the technique and its capacity to avoid the physiological and functional sequelae of VCFs. This fact, and the heterogeneity and methodological limitations of the studies, complicates the definition of the true role of the technique in clinical practice.
The present systematic review includes published and unpublished studies, and data from the FDA [5, 33, 45], and we believe it to be the largest such effort made to date. The results obtained show that BK produces significant reduction in pain intensity, regardless of the method used to evaluate it, and moreover also affords significant improvement in mobility, functional capacity, and quality of life. These benefits are maintained over the course of follow-up. The technique is also able to at least partially restore and correct vertebral height and the kyphotic deformity produced by VCFs. The results of the noncomparative studies indicate that, globally, BK affords a mean increase in vertebral height of 15±5%, though there are variations according to the segment subjected to measurement. Regarding kyphosis, a significant reduction is observed in both the absolute value of the Cobb angle and the degree of kyphotic deformity.
Assessment of the safety of the procedure reveals the presence of habitually asymptomatic cementing material leakage in 7% of the levels treated. Regarding the complications of the technique, problems were only noted in 2 and 1.16% of the patients and levels treated, respectively, though some of the complications appeared to be serious and required intensive care and/or emergency surgery (three cases). Complications are more frequent in patients with a larger number of underlying comorbidities [27, 28, 42], and with metastatic fractures [31]. Furthermore, in some cases, complications have been associated with both patient positioning maneuvers [15, 30] and insertion of the device during the learning curve of the technique [14]. On the other hand, the results of this review show that, globally, about 16% (95% CI: 10.7–22) of the patients subjected to BK suffer new vertebral fractures 1 year after treatment. The incidence in this case is highest among the patients with osteoporotic fractures. These figures are similar to the percentages (19–24%) described for the general population of patients with VCF [32], and do not confirm the greater risk associated with kyphoplasty postulated by some authors [55, 60].
In addition, the studies analyzed indicate that despite the age and fragility of the population involved, BK is generally well tolerated by the patients, who report high levels of satisfaction, and hospital stay after the procedure is short.
BK appears to be more safe and effective than vertebroplasty in the treatment of tumor VCFs, as it is able to reduce the loss of height and the degree of kyphotic deformity, and generates a lesser leakage rate while affording similar responses in terms of pain reduction and improvement in patient function quality of life [11]. Likewise in osteoporotic VCFs, it has been shown that kyphoplasty offers a significantly lesser contrast leakage rate [41]. These results are in turn ratified on establishing an indirect comparison with the available literature on vertebroplasty, where it is conclusively shown that the cement leakage rates and complications are lower when using BK [1, 6, 17, 29, 57]. On the other hand, the risk of new vertebral fractures appears to be similar with both techniques [1, 6, 17, 29, 57]—though the lack of direct comparisons does not allow us to confirm this entirely.
Compared with habitual medical management, BK at least over the short to middle term affords better management control, with a statistically significant reduction in pain and associated analgesic use, and improved mobility and independence. On the other hand, the fractures treated show no progression toward the vertebral collapse and kyphotic deformity associated with conventional medical treatment [8, 25, 26]. In turn, over the short term, the technique significantly reduces the risk of new fractures in adjacent vertebras. Likewise, there are data indicating that BK reduces the use of health care resources by shortening both hospital stay and the number of medical consultations due to pain in the 6 months after the application of the technique.
All these considerations define BK as a technique that is both promising and very interesting from the clinical point of view. However, many areas of uncertainty remain that do not allow us to firmly define the true role of the technique in clinical practice. Thus, while it is clear that BK significantly improves both vertebral height and spinal sagittal alignment, the clinical importance and repercussions of these effects have not yet been established, and little is known of their influence upon the medical complications secondary to VCFs. Knowledge is also lacking as to whether or not an association exists between the changes in spinal anatomy and variables of such great clinical importance as patient pain relief or functional capacity. Marked variability is moreover seen in the results of the individual studies. For example, the percentage of levels where kyphoplasty is able to reduce kyphosis angle is reported to be between 11 [56] and the 85% [4]. Such discrepancy seems attributable not only to the different criteria used to define the outcome threshold [4, 10, 42] and the different methods used to measure it (a lack of consensus being observed on this point), but also to the unequal presence in each study of factors presumed to possess prognostic value—such as the etiology of fracture, baseline vertebral height, the degree of kyphosis, the level treated, and the estimated age of the fracture—the importance of which remains unclear. Regarding safety, uncertainty also exists due at least in part to the methodological limitations of the studies. As an example, the studies made do not allow us to determine whether the risk of new vertebral fractures after kyphoplasty is associated with the etiology of VCFs; whether such risk is really similar to that of the general population of patients with VCFs; or whether there are other possible adverse effects of the technique over both the short and long term.
The literature shows a lack of consensus over the possible indications of BK and the appropriate timing of the technique. At present, possible candidates for the technique are patients with painful VCFs of osteoporotic or tumor origin and, in this latter group, particularrly those fractures secondary to multiple myeloma—since their characteristics facilitate tissue displacement to reduce the fracture and create the cement filler space. In other tumors it seems that the technical difficulties are greater [31], and the clinical experience gained is certainly much more limited. As to the selection of the best treatment level, there appears to be some agreement that the choice should be based on the results of the magnetic resonance imaging findings—specifically the presence of edema in the region of the fractured vertebra [55]. However, while some authors consider that the intervention is only indicated in patients with intractable pain refractory to medical management [27], or do not advise the technique in the case of simple osteoporotic fractures with minimal deformity [21], other investigators [10] define BK as the primary treatment of choice for osteoporotic fractures.
A lack of agreement is likewise observed regarding the best timing of the technique. Thus, while some authors do not recommend treatment of fractures estimated to be more than 3 months old [15, 21, 42], there are consistent data suggesting that chronic fractures are also amenable to BK, since the technique significantly reduces the pain and is at least partially able to restore vertebral height [4, 10, 25]. Given the natural course of VCFs [8], an early intervention in theory would afford better correction of the deformity and avoid increased vertebral collapse. However, this could result not only in the over-treatment of patients who would improve with conservative management, but could also pose a risk to their safety by subjecting them to an intervention not without risks and complications—and whose long-term efficacy has not been firmly established.
Regarding safety, and while acknowledging the important influence of patient age, fragility, and the number of existing comorbidities in the population amenable to treatment with BK, it seems possible to reduce the appearance of complications through the adequate selection of patients, the use of high-quality radiological techniques during insertion of the device, the injection of bone cement in an appropriate state of polymerization, and adequate surgeon training [24, 36, 54, 55]. This latter aspect is of particular importance, for although the procedure is percutaneous, it is also complex and—as reported in the literature—requires skill and experience. Consequently, an adequate learning curve must be observed to ensure satisfactory efficacy and safety performance.
Limitations of the review
The analysis of the literature on BK reveals a series of limitations that complicate extrapolation of the results to clinical practice. These limitations include a lack of direct comparisons with vertebroplasty with which to draw solid conclusions. On the other hand, many of the studies present methodological shortcomings, with known sources of bias—including poor description of the criteria used for patient selection and their lack of homogeneity due to the inclusion of fractures with different characteristics, etiologies, locations, and evolutive stages. Additional sources of bias include small sample size; scant description of concomitant treatments; the combination of kyphoplasty with other treatment measures (making it almost impossible to establish the differential contribution to the outcome of each technique); the lack of standard measures and the subjectivity of some of the outcome variables; the absence of masking in the assessment of the results; the variability and limited duration of follow-up; the lack of identification of losses and their causes; and poor quality in describing the results obtained [7, 35, 37, 49]. Such heterogeneity and limitations moreover make it impossible to establish a definitive estimate of the global effect of BK, since not all studies analyze the same variable of interest, and not all describe the results on a quantitative basis and in a comparable manner. On the other hand, many outcome variables are used, and their definition and the instruments used to evaluate them are often not standardized. Moreover, the variables are sometimes subjective or even inadequate due to recall bias. Another problem that cannot be entirely ruled out despite the efforts made is the possibility of publication bias.
Nevertheless, while we are aware of the aforementioned problems, in this review we decided not to limit the analytical setting to studies meeting strict methodological criteria, since this would imply ignoring the reality of the clinical implantation of the technique [3, 5]. Moreover, it was considered that the approach adopted could be useful not only for evaluating the real results of the technique but also for identifying little or incompletely analyzed aspects that could set the bases for new areas of methodologically appropriate research.
Conclusions
In synthesis, the available evidence reveals the efficacy and safety of BK in the treatment of painful VCFs secondary to osteoporosis or multiple myeloma. However, the uncertainty observed in the literature indicates that there is a particular need for prospective studies of good methodological quality to allow the following: (1) Precise determination of its efficacy in terms of both objective and subjective response, and specifically as regards the clinical repercussion and relevance of the increase in vertebral height and reduction in kyphotic deformity afforded by the technique. (2) Definition of the long-term efficacy of the procedure, and particularly of its influence upon the physiological, functional, and psychological complications secondary to VCFs. In this sense a specific point for evaluation is its impact upon lung function and patient survival. (3) The definition of the prognostic factors associated with response to treatment. (4) Precise determination of the short- and long-term adverse effects and morbidity-mortality associated with the procedure, and particularly of the rate of vertebral fractures adjacent to the treated segments. (5) Comparison between BK and conventional treatments and other percutaneous techniques to facilitate optimum therapeutic decision taking in patients with VCFs. (6) Determination of the costs of the procedure and the utilization of health care resources to assess its economic impact and cost-effectiveness.
References
Australian Safety and Efficacy Register of New Interventional Procedures—Surgical. ASERNIP-S (2003) Percutaneous Vertebroplasty. New and Emerging Techniques-Surgical
Belkoff SM, Mathis JM, Fenton DC, Scribner RM, Reiley ME, Talmadge K (2001) An ex vivo biomechanical evaluation of an inflatable bone tamp used in the treatment of compression fracture. Spine 26:151–156
Benson K, Hartz AJ (2000) A comparison of observational studies and randomized controlled trials. N Engl J Med 342:1878–1886
Berlemann U, Franz T, Orler R, Heini PF (2004) Kyphoplasty for treatment of osteoporotic vertebral fractures: a prospective non-randomized study. Eur Spine J 13:496–501
Black N (1996) Why we need observational studies to evaluate the effectiveness of health care. BMJ 312:1215–1218
Canadian Coordinating Office for Health Technologies Assessment (CCOHTA) (2002). Percutaneous vertebroplasty: a bone cement procedure for spinal pain relief. Issues Emerg Health Technol 31:1–4
Clarke M, Oxman AD (2003) Cochrane reviewer’s handbook 4.1.6 [updated January 2003]. The Cochrane library, number 1, Update Software, Oxford
Cortet B, Roches E, Logier R, Houvenagel E, Gaydier-Souquieres G, Puisieux F, Delcambre B (2002) Evaluation of spinal curvatures after a recent osteoporotic vertebral fracture. Joint Bone Spine 69:201–208
Coumans JVCE, Reinhardt MK, Lieberman IH (2003) Kyphoplasty for vertebral compression fractures: 1-year clinical outcomes from a prospective study. J Neurosurg 99:44–50
Crandall D, Slaughter D, Hankins PJ, Moore C, Jerman J (2004) Acute versus chronic vertebral compression fractures treated with kyphoplasty: early results. Spine J 4:418–424
Fourney DR, Schomer DF, Nader R, Chlan-Fourney J, Suki D, Ahrar K, Rhines LD, Gokaslan ZL (2003) Percutaneous vertebroplasty and kyphoplasty for painful vertebral body fractures in cancer patients. J Neurosurg 98:21–30
Fribourg D, Tang C, Parveen S, Delamartier R (2004) Incidence of subsequent vertebral fracture after Kyphoplasty. Spine 29:2270–2276
Gaitanis IN, Hadjipavlou AG, Katonis PG, Tzermiadianos MN, Pasku DS, Patwardhan A (2005) Balloon kyphoplasty for the treatment of pathological vertebral compressive fractures (Epub 2004 October 8). Eur Spine J 14:250–260
Garfin SR, Yuan HA, Reiley MA (2001) New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 26:1511–1515
Garfin SR (2003) Kyphon’s postmarketing study: Vertebral Body Compression Fracture Patient Registry. Final report. Kyphon Inc
Gavaghan DJ, Moore RA, McQuay HJ (2000) An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data. Pain 85:415–424
Grados F, Depriester C, Cayrolle G, Hardy N, Deramond H, Fardellone P (2000) Long-term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology 39:1410–1414
Grohs JG, Krepler P (2004) Minimal invasive stabilization of osteoporotic vertebral compression fractures. Methods and Preinterventional Diagnostics Radiologe 44:254–259
Hardouin P, Fayada P, Leclet H, Chopin D (2002) Kyphoplasty. Joint Bone Spine 69:256–261
Harrop JS, Prpa B, Reinhardt MK, Lieberman I (2004) Primary and secondary osteoporosis’ incidence of subsequent vertebral compression fractures after kyphoplasty. Spine 29:2120–2125
Heini PF, Orler R (2004) Kyphoplasty for treatment of osteoporotic vertebral fractures. Eur Spine J 13:184–192
Hillmeier J, Meeder PJ, Noldge G, Kock HJ, Da Fonseca K, Kasperk HC (2004) Augmentation von Wirbelkorperfrakturen mit einem neuen Calciumphosphat-Zement nach Ballon-Kyphoplastie. Orthopade 33:31–39
Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR (1999) Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 159:1215–1220
Kang JD, An H, Boden S, Phillips F, Foley K, Abdu W (2003) Cement augmentation of osteoporotic compression fractures and intraoperative navigation: summary statement. Spine 28:S62–S63
Kasperk HC, Hillmeier J, Noldge G, Grafe IA, DaFonseca K, Raupp D (2005) Treatment of painful vertebral fractures by kyphoplasty in patients with primary osteoporosis: a prospective cohort study (Epub 2004). J Bone Mineral Res 20:604–612
Komp M, Ruetten S, Godolias G (2004). Minimally invasive therapy for functionally unstable osteoporotic vertebral fracture by means of kyphoplasty: prospective comparative study of 19 surgically and 17 conservatively treated patients. J Miner Stoffwechs 11:13–15
Lane JM, Johnson CE, Khan SN, Girardi FP, Cammisa FP (2002) Minimally invasive options for the treatment of osteoporotic compression fractures. Orthop Clin North Am 33:431–438
Ledlie JT, Renfro M (2003) Balloon kyphoplasty: one-year outcomes in vertebral body height restoration, chronic pain, and activity levels. J Neurosurg 98:36–42
Levine SA, Perin LA, Hayes D (2000). An evidence based evaluation of percutaneous vertebroplasty. Manag Care 9:56–60
Lieberman IH, Dudeney S, Reinhardt M, Bell G (2001) Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine 26:1631–1638
Lieberman I, Reinhardt MK (2003) Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop S176–S186
Lindsay R, Silverman SL, Cooper C (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285:320–323
MacLean CH, Morton SC, Ofman JJ, Roth EA, Shekelle PG (2003) How useful are unpublished data from the Food and Drug Administration in meta-analysis? J Clin Epidemiol 56:44–51
Masala S, Cesaroni A, Sergiacomi G, Fiori R, Massari F, Manenti G, Nardi P, Simonetti G (2004) Percutaneous kyphoplasty: new treatment for painful vertebral body fractures. In Vivo 18:149–153
Moore RA, Gavaghan D, Tremer MR, Collins Sl, McQuay HJ (1998) Size is everything-large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 78:209–216
National Institute for Clinical Excellence (2003) Interventional procedure overview of Balloon Kyphoplasty for vertebral compression fractures. http://www.nice.org.uk/IP179overview
National Institute for Clinical Excellence (2004) Guide to the methods of Technology Appraisal. pp 1–40. http://www.nice.org.uk
Old JL, Calvert M (2004) Vertebral compression fractures in the elderly. Am Fam Physician 69:111–116
Papaioannou A, Watts NB, Kendler DL, Yuen CK, Adachi JD, Ferko N (2002) Diagnosis and management of vertebral fractures in elderly adults. Am J Med 113:220–228
Phillips FM (2003) Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 28:S45–S53
Phillips FM, Todd Wetzel F, Lieberman I, Campbell-Hupp M (2002) An in vivo comparison of the potential for extravertebral cement leak after vertebroplasty and kyphoplasty. Spine 27:2173–2178
Phillips FM, Ho E, Campbell-Hupp M, McNally T, Todd Wetzel F, Gupta P (2003) Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine 28:2260–2265
Rhyne A, Banit D, Laxer E, Odum S, Nussman D (2004) Kyphoplasty: report of eighty-two thoracolumbar osteoporotic vertebral fractures. J Orthop Trauma 18:294–298
Riggs BL, Melton LJ (1995) The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 17:S505–S511
Royle P, Waugh N (2003) Literature searching for clinical and cost-effectiveness studies used in health technology assessments reports carried out for the National Institute for Clinical Excellence appraisal system. Health Technol Assess 7(34):1–51
Schlaich C, Minne HW, Bruckner T (1998) Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int 8:261–267
Schwartz D (1981) Méthodes statistiques à l’usage des médecins et des biologistes. Flammarion Médecine-Science, Paris
Silverman SL (1992) The clinical consequences of vertebral compression fracture. Bone 13:S27–S31
Smith LA, Oldman AD, McQuay HJ, Moore RA (2000) Teasing apart quality and validity in systematic reviews: an example from acupuncture trials on chronic neck and back pain. Pain 86:119–132
Tamayo-Orozco J, Arzac-Palumbo P, Peon-Vidales H, Mota-Bolfeta R, Fuentes F (1997) Vertebral fractures associated with osteoporosis: patient management. Am J Med 103:S44–S50
Tang J, Liu JL (2000) Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol 53:477–484
The European Prospective Osteoporosis Study (EPOS) Group (2002) Incidence of vertebral fracture in Europe: Results from the European Prospective Osteoporosis Study (EPOS) J Bone Miner Res 17:716–724
Theodorou DJ, Theodorou SJ, Duncan TD, Garfin SR, Wong WH (2002) Percutaneous balloon kyphoplasty for the correction of spinal deformity in painful vertebral body compression fractures. Clin Imaging 26:1–5
Truumees E, Hilibrand A, Vaccaro AR (2004) Percutaneous vertebral augmentation. Spine J 4:218–229
Watts NB, Harris ST, Genant HK (2001) Treatment of painful osteoporotic vertebral fractures with percutaneous vertebroplasty or kyphoplasty. Osteoporos Int 12:429–437
Weisskopf M, Herlein S, Birnbaum K, Siebert C, Stanzel S, Wirtz DC (2003) Kyphoplastie - Ein neues minimalinvasives Verfahren zur Aufrichtung und Stabilisierung von Wirbelkorpern. [Kyphoplasty - a new minimally invasive treatment for repositioning and stabilising vertebral bodies]. Z Orthop Ihre Grenzgeb 141:406–411
Wilcox RK (2004) The biomechanics of Vertebroplasty: a review. Proc Inst Mech Eng [H ] 218:1–10
Wilhelm K, Stoffel M, Ringel F, Rao G, Rosseler L, Urbach H, Meyer B (2003) Ballon-Kyphoplastie zur Behandlung schmerzhafter osteoporotischer Wirbelkorperfrakturen - Technik und erste Ergebnisse. [Preliminary experience with balloon kyphoplasty for the treatment of painful osteoporotic compression fractures]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 175:1690–1696
Wong W, Reiley MA, Garfin S (2000) Vertebroplasty/kyphoplasty. J Women’s Imaging 2:117–121
Yuan HA, Brown CW, Phillips FM (2004) Osteoporotic spinal deformity: a biomechanical rationale for the clinical consequences and treatment of vertebral body compression fractures. J Spinal Disord Tech 17:236–242
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bouza, C., López, T., Magro, A. et al. Efficacy and safety of balloon kyphoplasty in the treatment of vertebral compression fractures: a systematic review. Eur Spine J 15, 1050–1067 (2006). https://doi.org/10.1007/s00586-005-0048-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-005-0048-x