
Abstract
Background
Emergency surgery itself induces high risk for postoperative mortality and morbidities; however, it remains unknown which concomitant pathological conditions of emergency surgeries are causative factors of deteriorating outcomes. This study examined the causal factors of postoperative mortality and morbidity in cases of emergency surgery.
Methods
Patients undergoing emergency surgery from January to December 2007 were enrolled in this retrospective cohort study. Causal relationships were analyzed by stepwise multivariate logistic regression analysis between possible independent factors (sex, age, kind of surgical department, timing of surgery, duration of surgery, blood transfusion, deteriorated consciousness level, shock state, abnormal coagulate state, and history of hypertension, diabetes, ischemic heart disease, chronic obstructive pulmonary disease, renal failure, and anemia) and postoperative mortality or morbidities (failure of removal of tracheal tube after operation, tracheotomy, cerebral infarction, massive hemorrhage, severe hypotension, severe hypoxemia, and severe arrhythmia during or after surgery).
Results
Shock, deteriorated consciousness level, chronic obstructive lung disease, and ischemic heart disease were significant risk factors for mortality (OR 14.2, 7.9, 6.4, and 3.8, respectively), and deteriorated consciousness level, blood transfusion, shock, chronic obstructive lung disease, diabetes, cardiovascular surgery, and operation longer than 2 h were significant risk factors for morbidity (OR 19.1, 3.3, 3.0, 2.5, 2.4, 2.4, and 1.8, respectively).
Conclusion
State of shock, deteriorated consciousness level, chronic obstructive lung disease, ischemic heart disease, hemorrhage requiring blood transfusion, age over 80 years, cardiovascular surgery, surgeries at night, and surgeries of duration more than 2 h cause patients to be strongly susceptible to postoperative mortality or morbidity in emergency surgeries.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
We have to decide whether patients undergoing surgery are fit for the operation and undergoing anesthesia and to inform them of the risks of postoperative morbidity and mortality. For this purpose we can use a wide range of tools varying from complicated scores such as POSSUM [1] to a simple evaluation such as ASA physical status [2] or the surgeon’s gut feeling [3]. In elective surgeries, some reports emphasize the priority of POSSUM or its modulations to predict correctly postoperative morbidity and mortality [4], but others emphasize a simple evaluation [5, 6].
Emergency surgery is accompanied with inherent risks of mortality and morbidity. Some reports have shown the priority of POSSUM as well as its modulation to predict correctly postoperative mortality and morbidity in emergency surgeries [7]. However, no information is available concerning use of a simple evaluation to predict correctly postoperative mortality and morbidity in emergency surgeries. Also, it might be considered whether dependent preoperative factors or comorbidities known to deteriorate postoperative outcomes in elective surgeries also provoke deteriorated postoperative outcomes in emergency surgeries. POSSUM scoring as well as its modalities requires the original format to give information on postoperative risk estimation for healthcare providers, and we believe that they do not always think this scoring system is feasible. Determination of dependent risk factors for postoperative morbidity and mortality in emergency surgeries should contribute to reliable risk assessment to predict postoperative morbidity and mortality in emergency surgeries. Thus, this retrospective cohort study aimed to seek concrete pathophysiological factors acting as the risk factors for deteriorated postoperative mortality and morbidity in emergency surgeries.
Methods
We retrospectively analyzed a series of 562 patients undergoing emergency surgery from January to December 2007. This retrospective analysis was in accordance with the STROBE statement. All the emergency surgeries were categorized into minor (hernia, varicose vein, minor perianal, scrotal, transurethral resection of prostate, and excision of large subcutaneous lesion), moderate (open cholecystectomy, laparoscopic cholecystectomy, appendectomy, excision of lesion requiring grafting or minor excision, minor amputation, and thyroid lobectomy), major (laparotomy and small bowel resections, colonic resection or anterior resection, major amputation, nonaortic vascular surgery, cholecystectomy and exploration of bile duct, and total thyroidectomy), and major+ surgeries (abdominoperitoneal excision of rectum, aortic surgery, Whipple resection, and radical total gastrectomy) in response to the POSSUM scoring system (Table 1). Clinical variables including gender, age, preoperative comorbidity, kind of surgical department, timing of surgery, duration of surgery, and blood transfusion were reviewed from a database of the anesthetic charts. Preoperative comorbidity included a deteriorated consciousness level, shock state, abnormal coagulate state, and history of hypertension (HT), diabetes mellitus (DM), ischemic heart disease (IHD), chronic obstructive pulmonary disease (COPD), renal failure, and anemia.
Age was categorized to patients more than 80 years old. Deteriorated consciousness level was categorized to preoperative consciousness level of patients as clear or not clear. Shock state was defined as a preoperative systolic blood pressure less than 80 mmHg in the presence of inotropics. Abnormal preoperative coagulation state was defined as preoperative prescription of anticoagulants, low platelet count (<15 × 104/μl), or prolonged prothrombin time (prothrombin time-international normalized ratio >1.25). HT was defined as a clinical history of HT and/or preoperative prescription of antihypertensive agents. DM was defined as a clinical history of DM, preoperative prescription of anti-DM agents including insulin, and/or abnormal HbA1c (>6.5 %). IHD was defined as a clinical history of IHD or chest pain suggesting angina pectoris. COPD was defined as a clinical history of COPD or asthma requiring treatments including bronchodilators, inhaled steroids, or β-adrenergic drugs. Renal failure was defined as abnormal serum creatinine (>1.1 mg/dl). Anemia was defined as low hemoglobin level (male <13.5 g/dl, female <11.5 g/dl). Timing of surgery was categorized to surgeries in the daytime (from 8:50 a.m. to 5:29 p.m.) or at night (from 5:30 p.m. to 8:49 a.m.). Duration of surgery was categorized to within 120 min or more than 120 min. In our institution, blood transfusion was performed to keep hemoglobin more than 10 g/dl.
Outcomes were reviewed from the medical records. Postoperative mortality was defined as death within 28 days postoperatively. Postoperative morbidities included leaving an operation room with tracheal intubation, postoperative tracheotomy, cerebral infarction, massive hemorrhage requiring blood transfusion, prolonged hypotension for more than 1 h during the postoperative periods, severe hypoxemia (PaO2 less than 80 mmHg) with the aid of artificial ventilation, and any type of arrhythmia during postoperative periods. Massive hemorrhage, severe hypotension, severe hypoxemia, and severe arrhythmia were defined as hemorrhage, hypotension, hypoxemia, arrhythmia that were considered to follow an unexpected prognosis such as cardiac arrest, cerebral infarction, and myocardial infarction. Prolonged duration of hospital stay was defined as duration more than 28 days after surgery.
Stepwise multivariate logistic regression was performed to assess the influence of these variables as an independent risk factor for postoperative mortality and morbidity. A P value < 0.05 was considered significant. The statistical analyses were aided by SPSS Ver. 14 (SPSS, Chicago, IL, USA).
Results
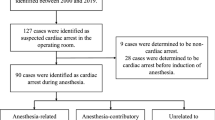
Data were obtained from all the enrolled patients. Table 2 showed the distributions of the four surgical severities, duration of surgeries, and specialized departments that performed surgeries, respectively. Eighty percent of the patients underwent moderate and major surgeries. Approximately 70 % of the patients experienced duration of surgery less than 2 h. The most common surgical type was abdominal surgery (40 %). Twenty-two patients (3.9 %) died within 28 days postoperatively; 78 patients (13.9 %) had postoperative complications; and 391 patients (30.4 %) were discharged within 28 days postoperatively.
The relationship between these factors and postoperative mortality is shown in Table 5. Shock, deteriorated consciousness level, COPD, and IHD were factors significantly different between survivor and death groups (OR 14.2, 7.9, 6.4, and 3.8, respectively).
The relationship between the factors and postoperative morbidities are shown in Table 6. Deteriorated consciousness level, blood transfusion, shock, COPD, DM, CV surgery, and operation lasting longer than 2 h were factors significantly different between discharge within 28 days and stay longer than 28 days (OR 19.1, 3.3, 3.0, 2.5, 2.4, 2.4, and 1.8, respectively).
Comparisons of preoperative factors of patients with and without postoperative comorbidity are shown in Table 7. Deteriorated consciousness level, CV surgery, blood transfusion, age over 80 years old, nighttime surgery, and operation lasting more than 2 h (OR 7.4, 6.2, 5.5, 3.2, 2.2, and 1.9, respectively) were significantly different factors between groups with no comorbidity and those with comorbidity.
Discussion
From the results in our study, shock state, deteriorated consciousness level, COPD, IHD, hemorrhage requiring blood transfusion, age more than 80 years old, cardiovascular surgery, surgeries at nighttime, and duration of surgeries more than 2 h were causative factors to caused postoperative mortality and morbidities in emergency surgeries. Also, cardiovascular surgery and DM were factors contributing to delay in discharge from the hospital. Because these pathological conditions were roughly defined to perform the retrospective cohort analysis, each factor certainly varied in severity. However, it should be said that preoperative acquisition of these roughly defined but dependent factors led us to estimate postoperative mortality and morbidities in emergency surgeries.
Regarding postoperative mortality, preoperative shock state, deteriorated consciousness level, IHD, and lung diseases are well-known risk factors in several kinds of elective surgery [8–15], being in good accordance with our findings that those factors revealed a strong relationship with postoperative mortality in emergency surgeries. In contrast, renal failure, DM, HT, and blood transfusion are also causative factors in postoperative mortality in several types of surgery [13, 16–18]. In our statistical criteria for the retrospective cohort study, these factors failed to associate with postoperative morbidities and mortality. A previous report has suggested that the combination of perioperative blood transfusion and subsequent development of postoperative infectious complications is associated with poor prognosis [19]. Our finding that blood transfusion prolonged hospital stay is in good agreement with this report. Further, there have been several reports showing that patient age is the most important predictor of mortality and morbidity in several kinds of surgery such as abdominal aortic aneurysm repair, peptic ulcer perforation, and chronic subdural hematomas [11, 20, 21]. The cutoff age of each report differs whether the operative risk is high [22]. In this study, we applied the cutoff age as >80 years old. Our study showed that age >80 years was the predictor not of mortality but of morbidity. Some reports have suggested that patient age is an independent factor and that reduced function of multiple organs and several preoperative comorbidities rather than age itself are associated with the deterioration in postoperative mortality and morbidity [23, 24]. Therefore, the patient’s age and age-related comorbidities might be an important factor predicting deteriorated postoperative morbidities in emergency surgeries.
Although cardiovascular surgery had a strong relationship with morbidity and the prolonged duration of hospital stay, it did not relate with mortality. A previous report has shown that the use of vasoactive drugs during operation relates with postoperative prognosis [25]. Therefore, our results strongly suggest that cardiovascular surgeries should be an important predictor to deteriorated postoperative morbidities even in emergency cardiovascular surgeries. Previous reports have suggested that night surgeries and admission to the intensive care unit at night does not associate with high mortality [26, 27]. Other reports have shown that fewer nursing staff at night in the intensive care unit is associated with postoperative pulmonary complications [28]. These findings suggest that the manpower at night in intensive care unit and wards is associated with morbidities but not with postoperative mortality. Our findings in emergency surgeries greatly supported that idea.
Preoperative assessment and subsequent management are one of the most important tasks assigned to surgeons and anesthesiologists. It is necessary to evaluate not only clinical and laboratory data but also disease severity by systemic perspectives [29]. ASA physical status is indeed one of the evaluation tools to predict postoperative mortality and morbidity, and Glance and colleagues [30] have shown that ASA physical status is a simple risk index for predicting 30-day mortality after noncardiac surgery. However, there has been no report showing dependent factors to predict postoperative morbidities. From our results, the factors including deteriorated consciousness level, shock state, IHD, COPO, and age >80 years old, all of which might count as high points in the POSSUM scoring system, seem to show strong relationships with postoperative outcome. Therefore, it should be said that the known predictors for deteriorated postoperative outcomes in elective surgeries are also useful predictors for these even in emergency surgeries.
This cohort study was based on the data of our institution but not on those of multicenter collaboration, and short-duration (70 % of less than 2 h) and moderate-major types of surgeries (80 %) were the characteristics of the analyzed population. Therefore, the results may differ from those with larger amounts of data or different populations such as those undergoing long and major types of surgeries. In addition, our results imply that the severity of surgery should be taken into the consideration for future studies to find more feasible, simpler, and more authentic risk evaluation for postoperative outcomes in emergency surgeries.
In conclusion, this retrospective cohort study showed that shock state, deteriorated consciousness level, COPD, IHD, hemorrhage requiring blood transfusion, age over 80 years, cardiovascular surgery, surgeries at night, and surgeries of duration more than 2 h are possible predicting factors of deteriorated postoperative mortality and morbidities in emergency surgeries.
References
Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78:355–60.
Gaston MS, Amin AK, Clayton RA, Brenkel IJ. Does a history of cardiac disease or hypertension increase mortality following primary elective total hip arthroplasty? Surgeon. 2007;5:260–5.
Markus PM, Martell J, Leister I, Horstmann O, Brinker J, Becker H. Predicting postoperative morbidity by clinical assessment. Br J Surg. 2005;92:101–6.
Campillo-Soto A, Flores-Pastor B, Soria-Aledo V, Candel-Arenas M, Andrés-García B, Martín-Lorenzo JG, Aguayo-Albasini JL. The POSSUM scoring system: an instrument for measuring quality in surgical patients. Cir Esp. 2006;80:395–9.
Sutton R, Bann S, Brooks M, Sarin S. The Surgical Risk Scale as an improved tool for risk-adjusted analysis in comparative surgical audit. Br J Surg. 2002;89:763–8.
Prause G, Ratzenhofer-Komenda B, Smolle-Juettner F, Krenn H, Pojer H, Toller W, Voit H, Offner A, Smolle J. Operations on patients deemed “unfit for operation and anaesthesia:” what are the consequences? Acta Anaesthesiol Scand. 1998;42:316–22.
Hobson SA, Sutton CD, Garcea G, Thomas WM. Prospective comparison of POSSUM and P-POSSUM with clinical assessment of mortality following emergency surgery. Acta Anaesthesiol Scand. 2007;51:94–100.
Sørensen LT, Malaki A, Wille-Jørgensen P, Kallehave F, Kjaergaard J, Hemmingsen U, Møller LN, Jørgensen T. Risk factors for mortality and postoperative complications after gastrointestinal surgery. J Gastrointest Surg. 2007;11:903–10.
Chavanon O, Costache V, Bach V, Kétata A, Durand M, Hacini R, Thony F, Blin D. Preoperative predictive factors for mortality in acute type A aortic dissection: an institutional report on 217 consecutives cases. Interact Cardiovasc Thorac Surg. 2007;6:43–6.
Lee CC, Chang IJ, Lai YC, Chen SY, Chen SC. Epidemiology and prognostic determinants of patients with bacteremic cholecystitis or cholangitis. Am J Gastroenterol. 2007;102:563–9.
Ramachandran R, Hegde T. Chronic subdural hematomas–causes of morbidity and mortality. Surg Neurol. 2007;67:367–72.
Treacy PJ, Reilly P, Brophy B. Emergency neurosurgery by general surgeons at a remote major hospital. ANZ J Surg. 2005;75:852–7.
Tao LS, Mackenzie CR, Charlson ME. Predictors of postoperative complications in the patient with diabetes mellitus. J Diabetes Complicat. 2008;22:24–8.
Mohammadi S, Dagenais F, Mathieu P, Kingma JG, Doyle D, Lopez S, Baillot R, Perron J, Charbonneau E, Dumont E, Metras J, Desaulniers D, Voisine P. Long-term impact of diabetes and its comorbidities in patients undergoing isolated primary coronary artery bypass graft surgery. Circulation. 2007;116:I220–5.
Greillier L, Thomas P, Loundou A, Doddoli C, Badier M, Auquier P, Barlési F. Pulmonary function tests as a predictor of quantitative and qualitative outcomes after thoracic surgery for lung cancer. Clin Lung Cancer. 2007;8:554–61.
Filsoufi F, Rahmanian PB, Castillo JG, Chikwe J, Carpentier A, Adams DH. Early and late outcomes of cardiac surgery in patients with moderate to severe preoperative renal dysfunction without dialysis. Interact Cardiovasc Thorac Surg. 2008;7:90–5.
Scott BH, Seifert FC, Grimson R. Blood transfusion is associated with increased resource utilisation, morbidity and mortality in cardiac surgery. Ann Card Anaesth. 2008;11:15–9.
Dionigi G, Rovera F, Boni L, Carrafiello G, Recaldini C, Mangini M, Laganà D, Bacuzzi A, Dionigi R. The impact of perioperative blood transfusion on clinical outcomes in colorectal surgery. Surg Oncol. 2007;16:S177–82.
Mynster T, Christensen IJ, Moesgaard F, Nielsen HJ. Effects of the combination of blood transfusion and postoperative infectious complications on prognosis after surgery for colorectal cancer. Danish RANX05 Colorectal Cancer Study Group. Br J Surg. 2000;87:1553–62.
Hirzalla O, Emous M, Ubbink DT, Legemate D. External validation of the Glasgow Aneurysm Score to predict outcome in elective open abdominal aortic aneurysm repair. J Vasc Surg. 2006;44:712–6.
Kocer B, Surmeli S, Solak C, Unal B, Bozkurt B, Yildirim O, Dolapci M, Cengiz O. Factors affecting mortality and morbidity in patients with peptic ulcer perforation. J Gastroenterol Hepatol. 2007;22:565–70.
Silberman S, Oren A, Klutstein MW, Merin O, Fink D, Bitran D. Surgery for ischemic mitral regurgitation: results and long-term follow-up. Harefuah. 2007;146:841–843, 911.
Açil T, Cölkesen Y, Türköz R, Sezgin AT, Baltali M, Gülcan O, Demircan S, Yildirir A, Ozin B, Müderrisoğlu H. Value of preoperative echocardiography in the prediction of postoperative atrial fibrillation following isolated coronary artery bypass grafting. Am J Cardiol. 2007;100:1383–6.
Bose AK, Aitchison JD, Dark JH. Aortic valve replacement in octogenarians. J Cardiothorac Surg. 2007;2:33.
Ford PN, Thomas I, Cook TM, Whitley E, Peden CJ. Determinants of outcome in critically ill octogenarians after surgery: an observational study. Br J Anaesth. 2007;99:824–9.
Carmody IC, Romero J, Velmahos GC. Day for night: should we staff a trauma center like a nightclub? Am Surg. 2002;68:1048–51.
Luyt CE, Combes A, Aegerter P, Guidet B, Trouillet JL, Gibert C, Chastre J. Mortality among patients admitted to intensive care units during weekday day shifts compared with “off” hours. Crit Care Med. 2007;35:3–11.
Dimick JB, Swoboda SM, Pronovost PJ, Lipsett PA. Effect of nurse-to-patient ratio in the intensive care unit on pulmonary complications and resource use after hepatectomy. Am J Crit Care. 2001;10:376–82.
Dzankic S, Pastor D, Gonzalez C, Leung JM. The prevalence and predictive value of abnormal preoperative laboratory tests in elderly surgical patients. Anesth Analg. 2001;93:249–50.
Glance LG, Lustik SJ, Hannan EL, Osler TM, Mukamel DB, Qian F, Dick AW. The Surgical Mortality Probability Model: derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann Surg. 2012;255:696–702.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Matsuyama, T., Iranami, H., Fujii, K. et al. Risk factors for postoperative mortality and morbidities in emergency surgeries. J Anesth 27, 838–843 (2013). https://doi.org/10.1007/s00540-013-1639-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-013-1639-z