
Abstract
Objectives
Advanced airway management in the prehospital setting is a serious issue in Japan because emergency medical technicians are not authorized to perform such management, whereas physicians—who are authorized to perform advanced airway management—do not usually engage in prehospital emergency medical activity. The purpose of this investigation was to investigate the success rate for endotracheal intubation (ETI) procedures and other methods of airway management employed by physicians in the prehospital setting in a single institution, as well as to examine the risk factors associated with difficult or failed endotracheal intubation (D/F ETI).
Methods
We performed a retrospective survey of patients treated in the prehospital setting by emergency physicians of the Hyogo Emergency Medical Center from 2004 to 2011. Patients were divided into two groups: a cardiopulmonary arrest (CPA) group and a non-CPA group. Data on cases of D/F ETI were obtained, and risk factors for these two groups were identified using univariate and statistical analysis.
Results
During the investigation period, ETI was attempted in the prehospital setting on 742 eligible patients; in 30 (4.04 %) of these cases, the attempts at ETI proved difficult or failed. Of those 30 patients, 13 patients received a surgical airway (attempts to provide a surgical airway failed in two patients), a blind ETI was performed in four, a video-assisted airway device was used in another four, and esophageal intubation was performed in four patients. Bag-valve ventilation alone was performed in one patient. The incidence of D/F ETI was higher in the non-CPA group than in the CPA group (6.27 vs. 2.63 %: p < 0.05). Facial or neck injury was a risk factor for D/F ETI in the prehospital setting in the CPA group (odds ratio 7.855; 95 % CI 1.754–36.293: p = 0.042). On the other hand, no risk factors for D/F ETI in the prehospital setting in the non-CPA group were identified.
Conclusion
The success rate for ETI performed by physicians in the prehospital setting at a single emergency medical center was high, and the incidence of D/F ETI was 4.31 %. The success rate for ETI in the CPA group was greater than that in the non-CPA group.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Airway management is often required for patients in the prehospital setting, and endotracheal intubation (ETI) is widely accepted as the “gold standard” for advanced airway management. Difficult airway management is a major concern for all emergency personnel engaged in prehospital activities. The success rate of ETI performed in the prehospital setting by physicians is reported to range from 96.8 to 100 % [1–4], which is higher than the corresponding rate achieved by nonphysicians [5–7]. In Japan, early and advanced medical intervention by physicians in the prehospital setting is considered when there is a critical airway problem to resolve, because physicians are able to perform various airway management techniques that nonphysicians are not authorized to attempt. Nevertheless, prehospital medical activities are not usually performed by physicians, and ETI is only performed by physicians in the prehospital setting at a few restricted institutions. As a result, there are no known reports on prehospital airway management performed by physicians in Japan.
The aim of this investigation was to investigate successful, difficult, and failed ETI (D/F ETI) procedures performed in the prehospital setting by physicians affiliated with a single emergency medical center in Japan. In addition, we analyzed the risk factors related to D/F ETI. This is the first report to focus on ETI performed in the prehospital setting by physicians in Japan.
Methods and subjects
Hyogo Medical Emergency Center (Kobe City, Hyogo Prefecture, Japan) has a prehospital medical service termed the “DC” (“Doctor Car") system, which is organized by a medical service team consisting of emergency physicians, nurses, emergency medical technicians, and drivers. In Japan, ETI can only be performed by emergency medical technicians on cardiopulmonary arrest patients following authorization by a physician. When emergency medical technicians in the prehospital setting determine that the patient is very critical and needs immediate medical treatment, including ETI, they request the DC prehospital medical service. Requesting the DC provides the option of more advanced medical interventions that are unacceptable for emergency medical technicians to perform, such as ETI on patients other than those who have suffered cardiopulmonary arrest, chest tube insertion, intravenous drug use, and ultrasonography. The background information for the case is recorded in a medical chart at Hyogo Medical Emergency Center, including the date, patient information (name, age, sex, past history, etc.), the names of the medical team members in the DC, location, the emergency medical service that requested the DC, the clinical course, assessment, and treatment of the patient, the pharmaceutical agent used in the prehospital setting, and the infusion volume used in the prehospital setting. This information is self-reported, and the diagnosis and condition are discussed later in a conference, when detailed information about the mission is added to the chart. All physicians that board the DC belong to the Hyogo Medical Emergency Center and are professionally engaged in emergency medicine and critical care.
Definition of difficult or failed endotracheal intubation (D/F ETI) in this investigation
For the present investigation, the definition of D/F ETI was standard orotracheal or nasotracheal intubation requiring multiple attempts (more than three trials) with a laryngoscope, the use of blind orotracheal or nasotracheal intubation (ETI performed without a clear view of the vocal cords) due to difficult laryngoscopy, the application of a video-assisted airway device (Airway Scope®, Pentax, Tokyo, Japan) or a supraglottic airway device due to difficult laryngoscopy, the implemention of surgical airway access (such as a tracheostomy or cricothyroidotomy) because a standard ETI was found to be difficult or impossible, esophageal intubation that was identified during transportation to or upon arrival at hospital, or bag-valve ventilation due to failed ETI.
Data collection
We retrospectively screened all patients over 18 years old who were treated in the prehospital setting using the DC charts from April 2004 to March 2011. We analyzed all cases in which the physicians attempted to intubate in the prehospital setting, and surveyed the usage of ETI and alternative airway management, cases of failed ETI, and complications. We also assessed risk factors related to D/F ETI in the prehospital setting. First, we divided the patients into two groups: cardiopulmonary arrest (CPA) and non-CPA patients. This was done because rapid sequence intubation is often necessary for non-CPA patients but is never necessary for CPA patients. Secondly, we assessed risk factors related to D/F ETI in the prehospital setting for these two groups. The risk factors were: (1) traumatic diagnosis, such as that caused by a traffic accident or crushing; (2) facial or neck injury; (3) intraoral hemorrhage, foreign body, vomitus; (4) rapid sequence intubation with muscle relaxants (this factor only applied to the non-cardiopulmonary arrest patient group).
Qualitative data are expressed as the number of patients and the corresponding percentage. Comparisons were performed using t tests and chi-squared tests. Explanatory variables are presented as odds ratios, with p values and 95 % confidence intervals. A p value of <0.05 was regarded as significant.
Results
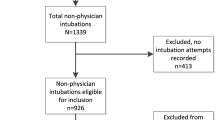
From April 2004 to March 2011, 3719 patients were treated in the prehospital setting by the DC team. Of those 3719 patients, ETI was attempted in 809 patients. Forty-nine patients were younger than 18 years old, the ages of twelve patients were unknown, the medical charts in the DC records were insufficient for three patients, and ETI was performed though permanent tracheal stoma in three patients. These 67 patients were excluded, meaning that 742 patients were finally eligible for this investigation. ETI was attempted in these 742 patients by total of 47 DC physicians (Fig. 1). Thirty of the 742 patients underwent D/F ETI (4.04 %). Among the 742 patients, there were 455 CPA patients and 287 non-CPA patients. The mean age of the CPA group was older than that of the non-CPA group, and the rate of traumatic diagnosis in the CPA group was much lower than the corresponding rate in the non-CPA group. The incidence of D/F ETI was significantly lower (2.63 %, 12/455) in the CPA group than in the non-CPA group (6.27 %, 18/287; p = 0.0143), as shown in Table 1. Among the 30 patients that underwent D/F ETI, 13 patients received a surgical airway (attempts to create such an airway in two patients failed), four underwent blind ETI, a video-assisted airway device was utilized in another four, esophageal intubation was realized in four patients, and bag-valve ventilation alone was performed in one patient (Table 2). Facial or neck injury was found to be a risk factor for D/F ETI in the CPA group, as shown in Table 3 (odds ratio 7.855; 95 % CI 1.754–36.293; p = 0.042). However, no risk factors were identified for D/F ETI in the non-CPA group (see Table 4).

Patient selection in this study
Discussion
ETI is often required as an advanced life support technique for critical and severely injured patients in the prehospital setting. Although ETI is standard practice in the prehospital setting in many countries, ETI by emergency medical technicians in Japan is only permitted in cases of cardiopulmonary arrest following authorization from a physician, and it is unusual for physicians to perform prehospital activities in Japan, except in some restricted institutions. Furthermore, the advanced airway management techniques available to emergency medical technicians are limited to supraglottic airway devices (laryngeal mask, esophageal–tracheal double-lumen airway) and orotracheal intubation with a standard laryngoscope. The greatest difference in the airway management techniques that can be implemented by physicians and emergency technicians in Japan is that physicians, but not emergency technicians, are able to perform various advanced airway management techniques for non-CPA patients using intravenous drugs. This state of affairs in Japanese emergency medical services means that advanced airway management for critical patients in the prehospital setting is not provided often enough, and it is expected that early intervention by physicians in the prehospital setting improves the outcome of critical patients. However, other than the present report, there are no known reports on airway management performed by physicians in the prehospital setting in Japan.
We found that the incidence of D/F ETI was 4.04 % (30/742), while 95.96 % (712/742) of the patients underwent ETI without difficulty. These results are quite similar to those in other reports [1–4], and the success rate of ETI in the prehospital setting by physicians in our investigation was as high as has been reported in other countries. All physicians who boarded the DC were professionally engaged in emergency medicine and critical care at the Hyogo Emergency Medical Center. They had experienced many cases with difficult airways in their routine clinical experience, and applied various approaches to those difficult airways. These factors may be associated with the high success rate of ETI observed in our investigation. The incidence of D/F ETI in the non-CPA group was higher than that in the CPA group in this investigation (p = 0.0143). Non-CPA patients have spontaneous respiration, trismus, clenched jaw, and muscle tightness, which often disturb direct laryngoscopy. On the other hand, unstable respiratory and circulatory conditions discourage the use of sedative agents, analgesic agents, and muscle relaxants to abate these symptoms. Therefore, ETI must be implemented in a more careful and complex manner for non-CPA patients than for CPA patients, which can make ETI in non-CPA patients more difficult and thus lower the incidence of ETI.
The surgical airway technique is recommended as an optional method in cases with difficult airway management according to guidelines for difficult airways [8, 9]. However, it is rarely performed in general. The incidence of the surgical airway technique was reported to be 0–10.9 % [2, 10, 11] in previous reports. We found that the incidence of the surgical airway technique was 1.75 % (13/742), which is within the range of values stated in those previous reports. The surgical airway technique aside, there are several noninvasive airway management techniques, and situations in which physicians must perform the surgical airway technique are extremely rare and limited. Therefore, the incidence of the surgical airway technique should be as low as seen in this investigation.
The availability of a video-assisted airway device in the prehospital setting has been reported [12, 13]. The alternative device used in the DC is the Airway Scope® video-assisted airway device, which is one of the alternative airway devices most frequently used in Japan for difficult airway cases. Although four difficult airway cases were successfully rescued using the video-assisted airway device, we could not draw any conclusions about the availability of a video-assisted airway device for difficult airways in the prehospital setting because it was only rarely used and because there is no established algorithm to follow when using this device. Another randomized prospective study will be necessary to prove the availability of a video-assisted airway device.
Previous investigations have found that the incidence of esophageal intubation by physicians in the prehospital setting is 6.7–12 % [11, 14]. In our investigation, esophageal intubation occured in 4 of 809 patients (0.5 %), a lower rate than stated in those previous reports. However, it is difficult to pinpoint the reason for the low incidence of esophageal intubation in our investigation because the patient characteristics, definition of esophageal intubation, and method used to detect esophageal intubation in our study were all different from those employed in the previous works. Moreover, our findings showed that esophageal intubation was an inevitable complication, and it was sometimes difficult to find esophageal intubation performed in the prehospital setting. The conditions needed to perform ETI are not always present in the prehospital setting; for example, there may be a noisy environment, a lack of illumination, limited time, and so on. Furthermore, the differential diagnosis of low oxygen saturation and abnormal ventilation is sometimes difficult under these conditions. Our results indicate the importance of avoiding and identifying esophageal intubation, as have previous reports.
Various risk factors related to ETI performed by physicians in the prehospital setting have been reported, including a short neck [1], face and neck injury [1, 15], trismus and clenched jaw [1, 16], obesity [1, 15, 16], history of ear, nose, or throat neoplasia or surgery [15], gag reflex [16], and operator status and position [15]. Face and neck injury was also a risk factor for D/F ETI in CPA patients in our investigation (2.4 vs. 16.5 %, odds ratio 7.855, CI 1.754–36.293, p < 0.042). Anatomical changes around the face and neck often disturb the intraoral view, making ETI difficult. Severe face and neck injury linked directly to CPA may worsen the conditions in which ETI is attempted, due to substantial anatomical changes. On the other hand, face, and neck injury in non-CPA patients was not a risk factor for D/F ETI. Face and neck injury that is not linked directly with CPA may cause only a slight or moderate anatomical change, and such slight or moderate changes may have little influence on ETI performed by a physician.
Although rapid sequence intubation with muscle relaxants has been shown to optimize situations requiring intubation [17, 18], and high success rates of ETI with rapid sequence intubation have been reported [19, 20], the use of muscle relaxants in ETI is still controversial. One reason to avoid using muscle relaxants is that diminishing spontaneous respiration may cause critical hypoxemia in the “can’t intubate, can’t ventilate” situation. In the non-CPA group of our investigation, rapid sequence intubation with muscle relaxants was administered to 117 patients, D/F ETI was encountered in eleven patients (9.4 %), and the incidence rate of D/F ETI without muscle relaxants was 8/170 (4.1 %). ETI with muscle relaxants was not identified as a risk factor for D/F ETI (odds ratio 2.416; 95 % CI 0.935–6.233, p = 0.07). However, this means that the use of muscle relaxants did not always improve the success rate of ETI. Our results suggest that the use of muscle relaxants does not always permit successful ETI, and that muscle relaxants should be administered following careful assessment.
Our investigation has several limitations. First, it was performed in a retrospective manner and only a single center was surveyed, so the results may not be applicable to all emergency prehospital units. In addition, we did not investigate the uniformity of the airway management algorithms used. The criteria for ETI and the airway management technique used in the prehospital setting were dependent on the physicians onboard the DC. Moreover, the backgrounds, careers, and subspecialties of the participating physicians were different. Physicians working at the Hyogo Emergency Medical Center include surgeons, orthopedists, cardiologists, anesthesiologists, and radiologists, which may have influenced the success rate of ETI and airway management technique used. Finally, the information on the patients was insufficient, especially in relation to obesity, which has been reported to be a risk factor for difficult intubation [1, 15, 16]. Exact body weight was not obtained at the first medical examination because it is difficult to measure the body weight of a critical patient upon arrival, and it is uncommon to measure the body weight of a patient who is not successfully resuscitated. If we had been able to consider obesity as a risk factor for D/F ETI, the results of our analysis might have been different.
In spite of these limitations, our findings showed a high success rate for ETI performed in the prehospital setting by physicians from a Japanese emergency medical center (which agrees with the results of previous reports), and that ETI tended to be more difficult in non-CPA than in CPA patients. Further studies and more investigations are needed to examine airway management by physicians in the prehospital setting.
References
Breckwoldt J, Klemstein S, Brunne B, Schnitzer L, Mochmann HC, Arntz HR. Difficult prehospital endotracheal intubation—predisposing factors in a physician based EMS. Resuscitation. 2011;82:1519–24.
Helm M, Hossfeld B, Schäfer S, Hoitz J, Lampl L. Factors influencing emergency intubation in the pre-hospital setting—a multicentre investigation in the German Helicopter Emergency Medical Service. Br J Anaesth. 2006;96:67–71.
Sollid SJ, Lossius HM, Søreide E. Pre-hospital intubation by anaesthesiologists in patients with severe trauma: an audit of a Norwegian helicopter emergency medical service. Scand J Trauma Resusc Emerg Med. 2010;14:18–30.
Warner KJ, Sharar SR, Copass MK, Bulger EM. Prehospital management of the difficult airway: a prospective cohort investigation. Emerg Med. 2009;36:257–65.
Wang HE, Mann NC, Mears G, Jacobson K, Yealy DM. Out-of-hospital airway management in the United States. Resuscitation. 2011;82:378–85.
Jones JH, Murphy MP, Dickson RL, Somerville GG, Brizendine EJ. Emergency physician-verified out-of-hospital intubation: miss rates by paramedics. Acad Emerg Med. 2004;11:707–9.
Jemmett ME, Kendal KM, Fourre MW, Burton JH. Unrecognized misplacement of endotracheal tubes in a mixed urban to rural emergency medical services setting. Acad Emerg Med. 2003;10:961–5.
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of difficult airway. Anesthesiology. 2003;98:1269–77.
Henderson JJ, Popat MT, Latto IP. Difficult Airway Society. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia. 2004;59:675–94.
Bair AE, Panacek EA, Wisner DH, Bales R, Sakles JC. Cricothyrotomy: a 5-year experience at one institution. J Emerg Med. 2003;24:151–6.
Cobas MA, De la Peña MA, Manning R, Candiotti K, Varon AJ. Prehospital intubations and mortality: a level 1 trauma center perspective. Anesth Analg. 2009;109:489–93.
Struck MF, Wittrock M, Nowak A. Prehospital Glidescope video laryngoscopy for difficult airway management in a helicopter rescue program with anaesthetists. Eur J Emerg Med. 2011;18:282–4.
Bjoernsen LP, Lindsay B. Video laryngoscopy in the prehospital setting. Prehosp Disaster Med. 2009;24:265–70.
Timmermann A, Russo SG, Eich C, Roessler M, Braun U, Rosenblatt WH, Quintel M. The out-of-hospital esophageal and endobronchial intubations performed by emergency physicians. Anesth Analg. 2007;104:619–23.
Combes X, Jabre P, Jbeili C, Leroux B, Bastuji-Garin S, Margenet A, Adnet F, Dhonneur G. Prehospital standardization of medical airway management: incidence and risk factors of difficult airway. Acad Emerg Med. 2006;13:828–34.
Wang HE, Kupas DF, Paris PM, Bates RR, Costantino JP, Yealy DM. Multivariate predictors of failed prehospital endotracheal intubation. Acad Emerg Med. 2003;10:717–24.
Davis DP, Ochs M, Hoyt DB, Bailey D, Marshall LK, Rosen P. Paramedic-administered neuromuscular blockade improves prehospital intubation success in severely head-injured patients. J Trauma. 2003;55:713–9.
Lieutaud T, Billard V, Khalaf H, Debaene B. Muscle relaxation and increasing doses of propofol improve intubating conditions. Can J Anaesth. 2003;50:121–6.
Fakhry SM, Scanlon JM, Robinson L, Askari R, Watenpaugh RL, Fata P, Hauda WE, Trask A. Prehospital rapid sequence intubation for head trauma: conditions for a successful program. J Trauma. 2006;60:997–1001.
Fullerton JN, Roberts KJ, Wyse M. Should non-anaesthetists perform pre-hospital rapid sequence induction? An observational investigation. Emerg Med J. 2011;28:428–31.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Kamiutsuri, K., Okutani, R. & Kozawa, S. Analysis of prehospital endotracheal intubation performed by emergency physicians: retrospective survey of a single emergency medical center in Japan. J Anesth 27, 374–379 (2013). https://doi.org/10.1007/s00540-012-1528-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-012-1528-x