
Abstract
Background
The Rome III diagnostic criteria had been used to diagnose functional gastrointestinal disorders (FGIDs) world wide, and functional bowel disorders (FBDs) including irritable bowel syndrome (IBS) have recently attracted the attention of Japanese physicians. However, there have been few reports on the prevalence of FBDs diagnosed by the Rome III diagnostic criteria.
Aims
The aim of this study was to determine the prevalence of FBDs diagnosed according to the diagnostic criteria of Rome III in Japan.
Patients and methods
All patients who were booked for colonoscopy were enrolled from eight institutions in Japan. This study was a prospective observational study in the period from April 2013 to December 2013. Patients filled out FGID questionnaires of Rome III when they were waiting for colonoscopy.
Results
Data for 1200 patients who underwent colonoscopy were analyzed. A total of 547 patients (45.6%) were diagnosed with FBDs. Out of those patients, 9.1% had IBS. According to the Rome III diagnostic criteria, 134 patients (11.2%) had functional bloating (FB), 73 (6.1%) had functional constipation (FC), 40 (3.3%) had functional diarrhea (FD), and 191 (15.9%) had unspecified functional bowel disorder (UFBD). Patients with FBDs had significantly higher rates of almost all symptoms (abdominal pain, hard or lumpy stools, loose or watery stools, and bloating) than those in the controls.
Conclusions
In Japan, the prevalence of FBDs and IBS is high, similar to that in the US. Many patients with FBDs have multiple symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rome III diagnostic criteria had been used to diagnose functional gastrointestinal disorders (FGIDs) worldwide since 2006 until 2016 [1]. FGIDs are chronic or recurrent gastrointestinal (GI) disorders that cannot be explained by structural abnormalities and have no objective findings. Guidelines for treatment of irritable bowel syndrome (IBS) and functional dyspepsia in Japan were published by the Japanese Society of Gastroenterology in 2014, and they have recently attracted the attention of Japanese doctors. In addition, functional bowel disorders (FBDs), which include IBS, functional bloating (FB), functional constipation (FC), functional diarrhea (FD) and unspecified functional bowel disorder (UFBD) are frequently encountered in a clinical situation [2]. In fact, IBS is one of the most frequent disorders in FGIDs, with a prevalence of 5–26% [3, 4]. Therefore, it appears that there are a huge number of people suffering from symptoms of IBS. However, the prevalence of IBS differs depending on gender, age, country and geographic area. For example, the number of female patients with IBS is 1.6-times larger than the number of male patients, the prevalence of IBS tends to decrease with advance of age and the prevalence of IBS in East South Asian countries is lower than that in South American countries [5]. The prevalence of IBS in Japan is similar to that in Western countries, but the prevalence in women and young people is higher [6,7,8].
However, there has been no report on the prevalence of FBDs diagnosed by the Rome III diagnostic criteria in Japan. The majority of doctors have in fact not used the FGID questionnaire in a clinical situation. A previous study showed that nearly 80% of doctors had no knowledge of symptom-based IBS criteria and that only 4% of doctors used the criteria in a clinical situation [3]. Therefore, it is necessary to diagnose FBDs according to the Rome III diagnostic criteria in clinical practice and to provide appropriate treatment for patients with FBDs.
To the best of our knowledge, this manuscript is the first report on the prevalence of FBDs with exclusion of organic diseases by using colonoscopic examination. There have been many reports on the prevalence of FBDs based on information obtained from the Internet, interviews, and letters [7, 9, 10]. Therefore, patients with inflammatory bowel disease (IBD), colitis, and advanced colon cancer might have been included in previous studies.
The aim of this study was to accurately determine the prevalence of FBDs classified by the Rome III diagnostic criteria after exclusion of organic disease by using colonoscopy (CS) in Japan.
Subjects and methods
Subjects
This study was a prospective observational study from eight institutions in Japan between April 2013 and December 2013 and was conducted with the approval of the Ethics Committee of Hokkaido University (approval number: 012-0405).
Diagnosis of FBDs
We used FGID questionnaires of Rome III that were formally translated and validated in Japanese to diagnose FBDs and to collect necessary information before CS in all subjects. The subjects were diagnosed as having FBDs on the basis of symptoms recorded in the questionnaires. FBDs and IBS subtypes were defined using the Rome III criteria. The FBDs included IBS, FB, FC, FD, and UFBD. Functional abdominal pain syndrome (FAPS) is different category from FBDs, but in the present study, it was diagnosed. IBS subtypes divided into IBS with diarrhea (IBS-D), IBS with constipation (IBS-C), mixed IBS (IBS-M), and unsubtyped IBS (IBS-U). Stool form was assessed using the Bristol scale.
Endoscopy and exclusion criteria
Consecutive cases that were booked for CS were enrolled in this study. Patients who disagreed with this study and received emergency endoscopy and patients with serious complications (such as advanced cancer, endocrinological disease, neurological disease, liver cirrhosis, and renal disease requiring hemodialysis) were excluded before CS. Subjects filled out FGID questionnaires in the Japanese version of Rome III while they were waiting for CS. The results of the questionnaires were fed into automatic diagnostic software, and classification was performed for each category. Colonoscopists who were blind to the diagnostic results performed CS to diagnose organic disease. Patients with IBD, pregnant women, patients having undergone intestinal resection, and patients with colitis including infections, microscopic colitis, and collagenous colitis or advanced colon cancer were excluded from this study.
The relationship between each FBD and lower abdominal symptoms
Frequency of symptoms in each category of FBDs was investigated. The symptoms were abdominal pain, hard or lumpy stools, loose or watery stools and bloating, with stool form being assessed by the Bristol scale. The frequency of abdominal pain and bloating was divided into ≧ 1 day and < 1 day per week, and a frequency of ≧ 1 day per week was defined as positive. The frequency of hard or lumpy stools and loose or watery stools was divided into ≧ 50% and < 50% of bowel movements, and ≧ 50% was defined as positive. Each category of FBDs diagnosed by using Rome III was compared with that of non-FBDs as a control.
Statistical analysis
Data are expressed as mean ± SD. Parameters were compared between the groups by Pearson’s Chi-square test and the Mann–Whitney test. Differences were considered statistically significant at a probability (p) level < 0.05.
Results
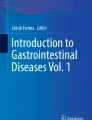
A total of 1324 patients who underwent colonoscopy were registered, but 124 patients were excluded because of intestinal resection (n = 56), colitis (n = 38), IBD (n = 11), advanced colon cancer (n = 9), pregnancy (n = 0), and input omission (n = 10). Data for 1200 cases were used for analysis (Fig. 1). The reasons for endoscopic examination were screening (n = 355), follow-up (n = 354), fecal occult blood (n = 228), bowel movement disturbance (n = 103), hematochezia (n = 74), abdominal pain (n = 57), and others (n = 71). The patients included 706 men (58.8%) and 494 women (41.2%) (Table 1). The mean age of the patients was 60.5 years. Surprisingly, 547 patients (45.6%) were diagnosed with FBDs, and 109 of those patients (9.1%) had IBS. Based on the Rome III criteria, 134 patients (11.2%) had FB, 73 (6.1%) had FC, 40 (3.3%) had FD, 191 (15.9%) had UFBD and 3 (0.3%) had FAPS. Patients with FBDs other than FD were significantly younger than the controls, and FB was significantly more frequent in females. Of the subjects fulfilling the IBS criteria, 24 (22.0%) had IBS-C, 35 (32.1%) had IBS-D, 24 (22.0%) had IBS-M, and 26 (23.9%) had IBS-U (Table 2). Patients with IBS-M were the youngest in all subtypes of IBS, and the majority had IBS-D (22 males and 13 females). The majority of males had IBS-D, and the majority of females had IBS-C.

Study flow chart
A total of 207 patients (17.3%) were positive for abdominal pain, and the most common in each category of FBDs was IBS (75 patients) (Table 3). A total of 178 patients (14.8%) were positive for hard or lumpy stools. However, the majority was non-FBDs (69 patients). A total of 102 patients (8.5%) were positive for loose or watery stools and the majority of those patients had IBS (37 patients) or FD (29 patients). A total of 197 patients (16.4%) had bloating, and the majority of those patients had FB (82 patients). The rates of patients in each category of FBDs (IBS, FB, FC and FD) were characteristic in each symptom (Fig. 2).

Rates of patients with FBDs with each symptom. The rates of patients in each category of FBDs (IBS, FB, FC, and FD) with each symptom are shown. The symptoms were abdominal pain, hard or lumpy stools, loose or watery stools and bloating, and stool form was assessed using the Bristol scale. The frequency of abdominal pain and bloating was divided into ≧ 1 and < 1 day per week, and a frequency of ≧ 1 day per week was defined as positive. The frequency of hard or lumpy stools and loose or watery stools was divided into ≧ 50 and < 50% of bowel movements, and ≧ 50% was defined as positive
Patients with IBS or FB had significantly higher rates of all symptoms (abdominal pain, hard or lumpy stools, loose or watery stools, and bloating) than those in the control (Fig. 3). Especially, patients with IBS were very high rates of all symptoms (Table 4). The symptom of loose or watery stools was excluded in FC and the symptom of abdominal pain was excluded in FD because those categories were defined not to include these symptoms. Patients with FC had significantly higher rates of all symptoms except loose or watery stools, and the rate of bloating was higher than that of hard or lumpy stools. Patients with FD had significantly higher rates in loose or watery stools and bloating.

Frequency of symptoms in each category of FBDs. Each category of FBDs diagnosed by using the Rome III was compared with that of non-FBDs as a control. Odds ratio and 95% CI are reported. The symptoms were abdominal pain, hard or lumpy stools, loose or watery stools and bloating. The frequency of abdominal pain and bloating was divided into ≧ 1 and < 1 day per week, and a frequency of ≧ 1 day per week was defined as positive. The frequency of hard or lumpy stools and loose or watery stools was divided into ≧ 50 and < 50% of bowel movements, and ≧ 50% was defined as positive
Discussion
In the present study, we investigated the prevalence of FBDs classified by the Rome III diagnostic criteria in Japan. We found that (1) the prevalence of FBDs was 45.6% and the prevalence of IBS was 9.1% and (2) many patients with FBDs had multiple symptoms.
This study showed the prevalence of FBDs is very high (45.6%) in Japan (Table 1). Actually, the prevalence of FGIDs other than IBS in a general population has been investigated in some studies. However, to our knowledge, the prevalence of FBDs, including FB, FC, FD, and UFBD, diagnosed by the Rome III criteria was investigated in only three studies [4, 11, 12]. Furthermore, there has been no report on the prevalence of FBDs diagnosed by the Rome III criteria in North America or Europe. Drossman et al. reported the prevalence of FBDs (44.0%) diagnosed by using the Rome I criteria in 1993 [13]. Our results are similar to results reported in China (41.6%) [12], but are different from previous studies in Taiwan (22.0%) [4] and Iran (10.9%) [11] by using the Rome III criteria. In addition, the present study is the first study on the prevalence of FBDs with exclusion of organic disease by using colonoscopic examination. There have been many studies in which the prevalence of FBDs was investigated by using information from the Internet, interviews, and letters [7, 9, 10]. Furthermore, patients with inflammatory bowel disease (IBD), colitis, or advanced colon cancer might have been included in previous studies. Therefore, our study is of great interest, because IBD, colitis, and advanced colon cancer were completely excluded by endoscopic examination.
The prevalence of IBS in the present study was high (9.1%). Previous studies showed that the prevalence of IBS was high in the US (11.1–13.1%) [10] and in Japan (13.1–14.2%) [7, 9, 14, 15] but in East Asia, for example, in China (5.9%) [12], Taiwan (4.4%) [4], and Hong Kong (5.4%) [16]. Lovell et al. reported that the prevalence of IBS depended on gender, age, residential area (e.g., 2% in France, 7% in South-East Asia, 10% in the US and 21% in South America) and occupation [5]. The prevalence of IBS in present study (9.1%) was a little lower than previous reports in Japan (13.1–14.2%); this is possibly the reason why patients with inflammatory bowel disease, colitis, and advanced colon cancer might have been included in previous studies. The prevalence in the present study was not similar to the prevalence reported in East Asia (China, Taiwan and Hong Kong), a region that is close to Japan with a similar race, but the prevalence was similar to that in the US. These results support previous reports, though the reason is not certain.
In the present study, there were 109 subjects with IBS, and of the subjects fulfilling the IBS criteria, 24 (22.0%) had IBS-C, 35 (32.1%) had IBS-D, 24 (22.0%) had IBS-M, and 26 (23.9%) had IBS-U (Table 2). In previous studies, IBS-D was more predominant than IBS-C [7, 14, 16,17,18,19,20], and the subtype prevalence of IBS was characterized by male predominance in IBS-D and female predominance in IBS-C [6, 21]. In the present study, the majority of the patients had IBS-D, with the majority of males having IBS-D and the majority of females having IBS-C. Therefore, though there was no significant difference in the numbers of female and male subjects in any IBS subgroup; our results support the previous reports.
Lovell et al. reported that the prevalence of IBS among women was 1.6-times higher than that among men [5], and Thompson et al. showed that the prevalence of FBDs was higher in women in Canada by using the Rome II criteria [22]. Other studies also showed a higher prevalence of IBS and FC among women. Actually, the prevalence of FBDs, diagnosed by the Rome III criteria, was investigated in only three studies [4, 11, 12]. Those three studies showed female predominance of FC, and Long et al. reported female predominance for both FC and FB. In the present study, we found that the prevalence of FB was higher in females, in agreement with previous reports.
A total of 207 patients (17.3%) felt abdominal pain at a frequency of more than 1 day per week, and 75 of those patients had IBS (Fig. 2 and Table 3). In other words, about one-third of the subjects who felt abdominal pain at a frequency of more than 1 day per week were diagnosed as having IBS. On the other hand, 178 patients (14.8%) had hard or lumpy stools, but about one-third of those patients were diagnosed with non-FBDs. Additionally, 102 patients (8.5%) had loose or watery stools and the majority of those patients had IBS (37 patients) or FD (29 patients). There were 197 patients (16.4%) with bloating and, surprisingly, 82 of those patients had FB and 53 had IBS. In other words, almost all patients who felt bloating at a frequency of more than 1 day per week were diagnosed as having FBDs.
In the present study, patients with IBS, FB, and FC were significantly higher rates of all symptoms (abdominal pain, hard or lumpy stools, loose or watery stools, and bloating) than those in the control (Fig. 3 and Table 4). Each category of FBDs had not only one characteristic symptom (e.g., IBS: abdominal pain, FB: abdominal bloating, FC: hard or lumpy stools and FD: loose or watery stools) but also multiple symptoms. Especially, this study showed that all categories of FBDs had many patients who felt bloating at a frequency of more than 1 day per week.
There are some limitations in the present study. One limitation of our study is selection bias, because the subjects were selected only from subjects who underwent CS. Actually, of those with IBS who see physicians, most are seen in the primary care sector with mild symptoms that are relatively easy to manage. Thompson WG et al. reported that the severity of IBS (especially abdominal pain or diarrhea) and psychological disturbance in IBS patients determined health care-seeking behaviors [23, 24]. Surprisingly, the prevalence of IBS by using Rome III criteria was 2.4% at general hospital in Japan. On the other hand, that was 40.2% at primary clinics and tertiary care settings in Korea [25]. In the present study, reasons for endoscopic examination were screening (n = 355), follow-up (n = 354), and fecal occult blood (n = 228); therefore, 927 patients (77.3%) were the subjects who had few symptoms. However, when we evaluate the prevalence of FBDs including IBS, we should consider the background characteristics of the analyzed subjects.
Next, in the present study, patients with serious complications (such as advanced cancer, endocrinological disease, neurological disease, liver cirrhosis, and renal disease requiring hemodialysis) were excluded before CS, but it was not possible to be excluded perfectly. In fact, Drossman et al. reported that other diseases might coexist, and it was necessary to be excluded [1]. The criteria of functional dyspepsia excluded endocrinological disease and neurological disease by the Rome III diagnostic criteria. On the other hand, the criteria of FBDs did not obviously exclude them. Longstreth et al. showed that previous diagnostic criteria presumed the absence of a structural or biochemical disorder; however, research will likely confirm that functional gut disorders manifest such findings [2, 26]. They reported that neurotransmitters and endocrine substances were related to the pathophysiology of IBS.
Next, the subjects potentially included microscopic colitis, which induces diarrhea, to be excluded. Malicz et al. showed that the incidence of reporting distinct endoscopic findings in microscopic colitis has risen with the advent of high-definition (HD) colonoscopies [27]. We excluded cases that included microscopic colitis; however, we did not diagnose all microscopic colitis by endoscopy. On the other hand, our study is the only study in which the prevalence of FBDs was investigated with exclusion of organic diseases by using CS, and the results showed that patients with FBDs were younger, and that the prevalence of FB was higher in females. In conclusion, this study showed that the prevalence of FBDs and IBS are high in Japan, and that there are many patients who are suffering from various symptoms. It is necessary to diagnose FBDs based on the FGID questionnaire in clinical practice and to provide appropriate treatment for patients with FBDs.
Abbreviations
- CS:
-
Colonoscopy
- FAPS:
-
Functional abdominal pain syndrome
- FB:
-
Functional bloating
- FBDs:
-
Functional bowel disorders
- FC:
-
Functional constipation
- FD:
-
Functional diarrhea
- FGIDs:
-
Functional gastrointestinal disorders
- IBD:
-
Inflammatory bowel disease
- IBS:
-
Irritable bowel syndrome
- UFBD:
-
Unspecified functional bowel disorder
References
Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology. 2006;130:1377–90.
Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480–91.
Jellema P, van der Windt DA, Schellevis FG, et al. Systematic review: accuracy of symptom-based criteria for diagnosis of irritable bowel syndrome in primary care. Aliment Pharmacol Ther. 2009;30:695–706.
Chang FY, Chen PH, Wu TC, et al. Prevalence of functional gastrointestinal disorders in Taiwan: questionnaire-based survey for adults based on the Rome III criteria. Asia Pac J Clin Nutr. 2012;21:594–600.
Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(712–721):e714.
Kanazawa M, Endo Y, Whitehead WE, et al. Patients and nonconsulters with irritable bowel syndrome reporting a parental history of bowel problems have more impaired psychological distress. Dig Dis Sci. 2004;49:1046–53.
Kubo M, Fujiwara Y, Shiba M, et al. Differences between risk factors among irritable bowel syndrome subtypes in Japanese adults. Neurogastroenterol Motil. 2011;23:249–54.
Kumano H, Kaiya H, Yoshiuchi K, et al. Comorbidity of irritable bowel syndrome, panic disorder, and agoraphobia in a Japanese representative sample. Am J Gastroenterol. 2004;99:370–6.
Miwa H. Life style in persons with functional gastrointestinal disorders—large-scale internet survey of lifestyle in Japan. Neurogastroenterol Motil. 2012;24(464–471):e217.
Jung HK, Halder S, McNally M, et al. Overlap of gastro-oesophageal reflux disease and irritable bowel syndrome: prevalence and risk factors in the general population. Aliment Pharmacol Ther. 2007;26:453–61.
Sorouri M, Pourhoseingholi MA, Vahedi M, et al. Functional bowel disorders in Iranian population using Rome III criteria. Saudi J Gastroenterol. 2010;16:154–60.
Long Y, Huang Z, Deng Y, et al. Prevalence and risk factors for functional bowel disorders in South China: a population based study using the Rome III criteria. Neurogastroenterol Motil. 2017;29:e12897
Drossman DA, Li Z, Andruzzi E, Temple RD, et al. US householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993;38:1569–80.
Miwa H. Prevalence of irritable bowel syndrome in Japan: internet survey using Rome III criteria. Patient Prefer Adherence. 2008;2:143–7.
Kaji M, Fujiwara Y, Shiba M, et al. Prevalence of overlaps between GERD, FD and IBS and impact on health-related quality of life. J Gastroenterol Hepatol. 2010;25:1151–6.
Lee S, Wu J, Ma YL, et al. Irritable bowel syndrome is strongly associated with generalized anxiety disorder: a community study. Aliment Pharmacol Ther. 2009;30:643–51.
Makharia GK, Verma AK, Amarchand R, et al. Prevalence of irritable bowel syndrome: a community-based study from northern India. J Neurogastroenterol Motil. 2011;17:82–7.
Krogsgaard LR, Engsbro AL, Bytzer P. The epidemiology of irritable bowel syndrome in Denmark. A population-based survey in adults ≤ 50 years of age. Scand J Gastroenterol. 2013;48:523–9.
Lin S, Mooney PD, Kurien M, et al. Prevalence, investigational pathways and diagnostic outcomes in differing irritable bowel syndrome subtypes. Eur J Gastroenterol Hepatol. 2014;26:1176–80.
Perveen I, Rahman MM, Saha M, et al. Prevalence of irritable bowel syndrome and functional dyspepsia, overlapping symptoms, and associated factors in a general population of Bangladesh. Indian J Gastroenterol. 2014;33:265–73.
Adeyemo MA, Spiegel BM, Chang L. Meta-analysis: do irritable bowel syndrome symptoms vary between men and women? Aliment Pharmacol Ther. 2010;32:738–55.
Thompson WG, Irvine EJ, Pare P, et al. Functional gastrointestinal disorders in Canada: first population-based survey using Rome II criteria with suggestions for improving the questionnaire. Dig Dis Sci. 2002;47:225–35.
Drossman DA, McKee DC, Sandler RS, et al. Psychosocial factors in the irritable bowel syndrome. A multivariate study of patients and nonpatients with irritable bowel syndrome. Gastroenterology. 1988;95:701–8.
Talley NJ, Boyce PM, Jones M. Predictors of health care seeking for irritable bowel syndrome: a population-based study. Gut. 1997;41:394–8.
Nakajima S, Takahashi K, Sato J, et al. Spectra of functional gastrointestinal disorders diagnosed by Rome III integrative questionnaire in a Japanese outpatient office and the impact of overlapping. J Gastroenterol Hepatol. 2010;25(Suppl 1):S138–43.
Fukudo S, Kaneko H, Akiho H, et al. Evidence-based clinical practice guidelines for irritable bowel syndrome. J Gastroenterol. 2015;50:11–30.
Marlicz W, Skonieczna-Zydecka K, Yung DE, et al. Endoscopic findings and colonic perforation in microscopic colitis: a systematic review. Dig Liver Dis. 2017;49:1073–85.
Acknowledgements
We wish to thank Dr. Uehara and Dr. Hokari for participation this study. Mototsugu Kato has served in speaking and teaching commitments for Eisai Co., Ltd., Daiichi Sankyo Company, Ltd., Takeda Pharmaceutical Co. Ltd., Otsuka Pharmaceutical Co., Ltd. and AstraZeneca and has received scholarship grants from Eisai Co., Ltd., Takeda Pharmaceutical Co. Ltd., Daiichi Sankyo Company, Ltd., AstraZeneca and Astellas Pharma Inc. Sakamoto received a research grant from Daiichi-Sankyo, Gilead Sciences, and MSD, and received lecture fees from Bristol-Myers-Squibb, Gilead Sciences, MSD, Otsuka Pharmaceutical, and AbbVie.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Ono, M., Kato, M., Miyamoto, S. et al. Multicenter observational study on functional bowel disorders diagnosed using Rome III diagnostic criteria in Japan. J Gastroenterol 53, 916–923 (2018). https://doi.org/10.1007/s00535-017-1428-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-017-1428-9