
Abstract
Background
Accurately evaluating liver fibrosis in patients with non-alcoholic fatty liver disease (NAFLD) is important for identifying those who may develop complications. The aims of this study were (1) to measure serum Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+-M2BP) using the glycan sugar chain-based immunoassay and (2) to compare the results with clinical assessments of fibrosis.
Methods
Serum WFA+-M2BP values were retrospectively evaluated in 289 patients with NAFLD who had undergone liver biopsy. Histological findings were evaluated by three blinded, experienced liver-specific pathologists.
Results
For stages 0 (n = 35), 1 (n = 113), 2 (n = 49), 3 (n = 41), and 4 (n = 51) of liver fibrosis, the serum WFA+-M2BP cutoff indexes were 0.57, 0.70, 1.02, 1.57, and 2.96, respectively. Multivariate regression analysis showed that serum WFA+-M2BP values were associated with the stage of fibrosis (≥stage 2). The areas under the receiver operating characteristic curve (AUROC), sensitivity, and specificity of serum WFA+-M2BP were 0.876, 85.9, and 74.6 %, respectively, for severe fibrosis (≥stage 3) and were 0.879, 74.6, and 87.0 %, respectively, for cirrhosis. When compared with six non-invasive conventional markers, serum WFA+-M2BP had the greatest AUROC for diagnosing severe fibrosis and cirrhosis.
Conclusions
Serum WFA+-M2BP values are useful for assessing the stage of liver fibrosis in patients with NAFLD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is one of the most common liver diseases worldwide and is recognized as the hepatic manifestation of metabolic syndrome [1–3]. NAFLD can be classified as simple steatosis or non-alcoholic steatohepatitis (NASH), a progressive form of chronic liver disease (CLD), resulting in cirrhosis, hepatic failure, and hepatocellular carcinoma. Accurately evaluating liver fibrosis in NAFLD patients is important for identifying those who may progress to severe clinical conditions such as liver cirrhosis and hepatocellular carcinoma [4–7]. Liver biopsies are the gold standard for diagnosing NASH and associated liver fibrosis [8]. However, there is controversy surrounding the active use of liver biopsies for these purposes, because they have several drawbacks [9, 10]. A liver biopsy is highly costly and invasive with rare but potentially life-threatening complications [11]. In addition, sampling errors may occur, because a standard liver biopsy sample represents only 1/50,000 of the whole liver [12]. Furthermore, inter- and intra-observer variability also poses serious problems for the pathological diagnosis of NAFLD [13–17]. Accordingly, there is an urgent need for a non-invasive method for estimating the stage of liver fibrosis in NAFLD patients. Several methods using serum markers [18, 19], scoring systems [20–23], and imaging techniques, such as transient elastography [24–26], have been developed. Although each method has been reported as useful, few have been independently validated. Several problems also remain unaddressed, such as the methods’ complexities, reproducibilities, and costs for routine clinical use.
Recently, we developed a new glyco-marker for liver fibrosis using the glycan sugar chain-based immunoassay. The FastLec-Hepa system was used to determine the serum values of sweet-doughnut hyperglycosylated Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+-M2BP) for the assessment of liver fibrosis [27–29]. Toshima et al. [30] and Yamasaki et al. [31] reported that this assay offered a feasible means of assessing liver fibrosis in patients with CLD due to the hepatitis C virus (HCV). However, the progressive patterns of fibrosis may differ for CLD due to HCV and CLD due to NAFLD. Indeed, liver specimens from NAFLD patients show pericellular fibrosis around the central vein in the early stages, with gradual progression to fibrosis when central veins become connected to surrounding lobules. In contrast, central vein involvement in patients with CLD due to HCV is generally preceded by portal tract damage with pathological changes to the portal vein.
We investigated the clinical usefulness of serum WFA+-M2BP values in patients with well-characterized NAFLD. First, we confirmed the efficacy of serum WFA+-M2BP values for assessing the stage of fibrosis. Second, we compared the diagnostic performances of serum WFA+-M2BP and other non-invasive fibrosis markers and tests that are used to estimate the stage of liver fibrosis.
Methods
Patients
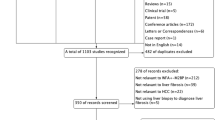
We retrospectively reviewed 325 NAFLD patients who underwent liver biopsy at Ehime University Hospital (Ehime, Japan), Ikeda Municipal Hospital (Osaka, Japan), Kawasaki Medical School Hospital (Okayama, Japan), or Sapporo Kosei General Hospital (Hokkaido, Japan). The exclusion criteria were as follows: a history of other liver diseases, including hepatitis B virus or HCV infection; administration of drugs that influence the activity of the disease, such as tamoxifen or a glucocorticoid; or a history of alcohol abuse (defined as ≥20 g of alcohol daily). Written informed consent was obtained from all patients who participated. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected by each institutional review committee’s a priori approval of this study.
Histological evaluation
Each NAFLD patient received a liver biopsy under laparoscopy or ultrasonography between July 2003 and September 2013. The biopsied liver samples were fixed in formalin and were embedded in paraffin according to the standard procedure at each institution. Slices (4 µm thick) were stained with hematoxylin and eosin (H&E), Azan-Mallory, silver, and Elastica van Gieson at Keio University. Liver samples <15 mm long were excluded, because the detection of liver fibrosis may be affected by sampling errors with such samples. A minimum of six portal tracts in the specimen was required for diagnosis. All liver samples were independently evaluated by three experienced liver-specialized pathologists (M.S., G.Y., and M.K.) who were blinded to the clinical data, and all evaluations were validated through discussion. The liver fibrosis stages were assessed according to Brunt’s criteria [32]. Significant and severe fibrosis was defined as ≥stage 2 and ≥stage 3, respectively. Thirty-six patients were excluded because of clinical and/or histological reasons; thus, 289 patients were included in the final analysis.
Clinical and biochemical data
Relevant clinical data were recorded, including the patient’s age, sex, weight, and height. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Venous blood samples were obtained in the morning after overnight fasting, either immediately before or no more than 2 months after liver biopsy. The blood samples were stored at −80 °C until analysis.
The biochemical variables were measured using a conventional automated analyzer at the respective hospitals. We analyzed the serum levels for the following: platelet count, prothrombin time, bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyltranspeptidase, albumin, cholesterol, triglyceride, fasting plasma glucose (FPG), ferritin, and hyaluronic acid. The AST-to-platelet ratio index (APRI) was calculated as follows: [AST (U/L)/UNL × 100]/platelet count. In this equation, UNL is the upper limit of the normal AST [33]. The FIB-4 index was calculated as follows: age (years) × AST (U/L)/platelet count (×109/L) × \(\sqrt {\text{ALT}}\) (U/L) [20]. The NAFLD fibrosis score was calculated as follows: −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × impaired fasting glycemia or diabetes (yes = 1; no = 0) + 0.99 × AST/ALT ratio − 0.013 × platelet (× 109/L) − 0.66 × albumin (g/dL) [21].
Serum Wisteria floribunda agglutinin-positive Mac-2 binding protein value
The WFA+-M2BP value in sera was measured by a WFA-antibody immunoassay using a chemiluminescence enzyme immunoassay machine (HISCL-2000i; Sysmex, Kobe, Japan), as previously reported [27, 28, 30, 31]. The measured values of WFA+-M2BP using the conjugated WFA were indexed with the obtained values using the following equation: cutoff index (COI) = ([WFA+-M2BP]sample − [WFA+-M2BP]NC) ÷ ([WFA+-M2BP]PC) − [WFA+-M2BP]NC). In this equation, [WFA+-M2BP]X denotes the [WFA + -M2BP] count of the serum sample ( X = sample), positive control ( X = PC), or negative control ( X = NC).
Statistical analysis
Quantitative values are presented as mean ± standard deviation, unless otherwise noted. The Steel–Dwass test was used for multiple comparisons of continuous variables among the different groups. Univariate and multivariate analyses were performed using a logistic regression model. Each cutoff value was determined from the receiver operating characteristic (ROC) curve analyses. The diagnostic performances of the markers were expressed as the diagnostic specificity, sensitivity, positive predictive value, negative predictive value, and area under the ROC (AUROC) curve. p values <0.05 were considered statistically significant. All statistical analyses were performed using JMP, version 11 software (SAS Institute, Tokyo, Japan).
Results
Cross-sectional association between Wisteria floribunda agglutinin-positive Mac-2 binding protein values and the fibrosis stage
The patients’ characteristics are summarized in Table 1. The mean age of the 289 patients (159 men and 130 women) was 54.8 ± 14.6 years old. Figure 1 shows the serum WFA+-M2BP values for each fibrosis stage. The serum WFA+-M2BP values measured by glycan-based immunoassay ranged from 0.12 to 11.06 (COI). The WFA+-M2BP value in patients with stages 0 (n = 35), 1 (n = 113), 2 (n = 49), 3 (n = 41), and 4 (n = 51) of fibrosis had COIs of 0.57, 0.70, 1.02, 1.57, and 2.96, respectively, demonstrating a stepwise increase with an increasing severity of liver fibrosis (Fig. 1). All pairs of groups differed significantly according to the Steel–Dwass test (stage 0 vs. stage 1, p = 0.012; stage 0 vs. stage 2, p < 0.001; stage 0 vs. stage 3, p < 0.001; stage 0 vs. stage 4, p < 0.001; stage 1 vs. stage 2, p = 0.002; stage 1 vs. stage 3, p < 0.001; stage 1 vs. stage 4, p < 0.001; stage 2 vs. stage 3, p = 0.014; stage 2 vs. stage 4, p < 0.001; and stage 3 vs. stage 4, p = 0.008).

The serum Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+-M2BP) values for each fibrosis stage. The top and bottom of each box represent the first and third quartiles, respectively, with the height of the box representing the interquartile range, covering 50 % of the values. The line across each box represents the median. The whiskers show the highest and lowest values. All pairs of groups are significantly different, as assessed using the Steel–Dwass test (p < 0.01). COI cutoff index
Comparisons of variables associated with the diagnosis of the fibrosis stage
The variables associated with each stage of liver fibrosis were assessed by univariate and multivariate analyses (Tables S1, 2).
Variables associated with the presence of fibrosis (≥stage 1)
According to univariate analysis, eight variables (age, BMI, platelet count, prothrombin time, AST, ALT, albumin, and the WFA+-M2BP value) were associated with the presence of fibrosis (Table S1). Multivariate analysis showed that the BMI [odds ratio (OR) 1.228, 95 % confidence interval (CI) 1.089–1.412], prothrombin time (OR 0.948; 95 % CI 0.914–0.982), and AST (OR 1.078; 95 % CI 1.023–1.144) were independently associated with the presence of fibrosis (Table 2).
Variables associated with the presence of significant fibrosis (≥stage 2)
Univariate analysis identified ten variables (sex, age, platelet count, prothrombin time, bilirubin, AST, albumin, cholesterol, FPG, and the WFA+-M2BP value) that were associated with the presence of significant fibrosis (Table S1). However, multivariate analysis showed that age (OR 1.049; 95 % CI 1.014–1.087), prothrombin time (OR 0.957; 95 % CI 0.925–0.986), AST (OR 1.036; 95 % CI 1.022–1.052), ALT (OR 1.036; 95 % CI 1.022–1.052), FPG (OR 1.013; 95 % CI 1.004–1.024), and the WFA+-M2BP value (OR 5.875; 95 % CI 2.339–16.369) were independently associated with the presence of significant fibrosis (Table 2).
Variables associated with the presence of severe fibrosis (≥stage 3)
According to univariate analysis, ten variables (sex, age, platelet count, prothrombin time, bilirubin, albumin, cholesterol, triglyceride, FPG, and the WFA+-M2BP value) were associated with the presence of severe fibrosis (Table S1). However, multivariate analysis showed that the platelet count (OR 0.864; 95 % CI 0.787–0.941), FPG (OR 1.014; 95 % CI 1.004–1.024), and the WFA+-M2BP value (OR 8.471; 95 % CI 3.562–22.725) were independently associated with the presence of severe fibrosis (Table 2).
Variables associated with the presence of cirrhosis (stage 4)
Univariate analysis identified 11 variables (sex, age, platelet count, prothrombin time, bilirubin, ALT, albumin, cholesterol, triglyceride, FPG, and the WFA+-M2BP value) that were associated with the presence of cirrhosis (Table S1). Multivariate analysis identified that the platelet count (OR 0.895; 95 % CI 0.814–0.978), prothrombin time (OR 0.963; 95 % CI 0.927–0.993), FPG (OR 1.012; 95 % CI 1.002–1.022), and the WFA+-M2BP value (OR 2.390; 95 % CI 1.462–4.423) were independently associated with the presence of cirrhosis (Table 2).
Diagnostic power of the Wisteria floribunda agglutinin-positive Mac-2 binding protein values for each fibrosis stage
The WFA+-M2BP ROC curves for diagnosing each fibrosis stage are presented in Fig. 2. The AUROC curve values (95 % CI) for the prediction of ≥stage 1, ≥stage 2, ≥stage 3, and stage 4 using the serum WFA+-M2BP values were 0.788 (0.736–0.833), 0.838 (0.790–0.879), 0.876 (0.832–0.911), and 0.879 (0.835–0.914), respectively (Table 3). The optimal cutoff values were 0.59 for ≥stage 1, 0.90 for ≥stage 2, 0.94 for ≥stage 3, and 1.46 for stage 4 (Table 3). The sensitivities for the prediction of ≥stage 1, ≥stage 2, ≥stage 3, and stage 4 were 74.8, 77.3, 85.9, and 72.6 %, respectively; whereas, the specificities were 74.3, 81.1, 74.6, and 87.0 %, respectively (Table 3).

The diagnostic capabilities of the serum Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+-M2BP) values for assessing the stage of liver fibrosis. The areas under the receiver operating characteristic curve of serum WFA+-M2BP for diagnosing liver fibrosis were as follows: a 0.788 for stage ≥1; b 0.838 for stage ≥2; c 0.876 for stage ≥3; and d 0.879 for stage 4
Comparisons of AUROC curve values for diagnosing the fibrosis stage
The AUROC curve values for diagnosing each fibrosis stage are shown in Table 4. Compared with the other surrogate markers and scoring systems, the serum WFA+-M2BP was the most useful marker for differentiating stages 0–2 from stages 3–4 and stages 0–3 from stage 4. The AUROC curve values for differentiating stages 0–1 from stages 2–4 were compatible with the serum WFA+-M2BP (0.838), hyaluronic acid (0.833), and the FIB-4 index (0.844).
Discussion
Clinically, it is very important to identify patients who have NASH with advanced fibrosis, because these patients have more liver-related complications and a greater mortality rate than patients who have NASH without liver fibrosis [4–7]. Although a liver biopsy is the gold standard for diagnosing and assessing the stages of fibrosis, research on noninvasive methods for assessing the fibrosis stages have rapidly evolved over the last decade [17–26]. In this study, we found that the serum WFA+-M2BP values measured using a glycan-based immunoassay provided a useful diagnostic factor for assessing the liver fibrosis stage in NAFLD patients (Fig. 1). The glycan-based immunoassay was previously developed as a simple system for automatically detecting unique fibrosis-related glycoalterations [27–31]. Moreover, the accuracy of the serum WFA+-M2BP values for diagnosing severe fibrosis and cirrhosis was superior to that offered by other surrogate markers and tests (Table 4).
M2BP is a secreted glycoprotein that is found in the serum of healthy individuals, but its concentration increases in patients with various cancers and viral infections, including HCV [34, 35]. This protein binds galectin-3, β-1 integrins, collagens, and fibronectin and has some relevance to cell–cell and cell–extracellular matrix adhesion [36, 37]. Therefore, it is reasonable to assume that M2BP reflects the progression of fibrosis in cases of CLD. Indeed, using proteome analysis, Cheung et al. [38] found that serum M2BP is a potential marker of fibrosis progression in HCV patients.
In this study, we found that the serum WFA+-M2BP value can be used to distinguish the fibrosis stages in NAFLD patients (Fig. 1; Tables S1, 2, 3). Recently, Kamada et al. [39] reported that the serum M2BP value (the whole M2BP protein measured by enzyme-linked immunosorbent assay) can be used for predicting the fibrosis stage in NAFLD patients. However, there are several differences between the present study and Kamada et al.’s study. In our study, the serum WFA+-M2BP value (the altered M2BP with fibrosis-related N-glycans measured by glycan-based immunoassay) increased stepwise with the increasing severity of liver fibrosis, whereas a stepwise increase was not found in Kamada et al.’s study. Further, our method can distinguish between the fibrosis stages more clearly, not only in patients with advanced fibrosis stage but also in those with earlier fibrosis stages of NAFLD (Fig. 1). In our previous study [27], we found that both the quantity and quality of M2BP were altered during the progression of fibrosis of CLD due to HCV. Since the N-glycosylation of M2BP was dramatically altered during the progression of liver fibrosis, we considered that the WFA+-M2BP reflects the fibrosis status more precisely than the whole M2BP protein. Further, the quantification of the WFA+-M2BP may offer a better marker for assessing the liver fibrosis stage than does the quantification of the M2BP protein. Currently, the N-glycan structures of WFA−-M2BP and WFA+-M2BP are being analyzed using mass spectrometry in our laboratory. Moreover, our system has been converted to a fully automated immunoassay analyzer for clinical use, featuring a measurement time of only 17 min, which has clear practical implications [27, 28, 30, 31].
Numerous non-invasive panels of the tests have been developed to assess the liver fibrosis stages [17–26]. In this study, the serum WFA+-M2BP values offered a superior AUROC curve for the diagnosis of severe fibrosis and cirrhosis compared with the FIB-4 index and five other markers and scoring systems (Table 4). In a study of a large Japanese cohort, the FIB-4 index was the most useful index for diagnosing patients with advanced fibrosis [40]. Although the American Association for the Study Liver Diseases’ guidelines [3] recommend the NAFLD fibrosis score [21] when deciding whether to perform a liver biopsy, the usefulness of this score remains questionable in Asian patients [40, 41]. Consistent with these studies, the NAFLD fibrosis score yielded lower AUROCs than the WFA+-M2BP values and the FIB-4 index for diagnosing fibrosis in our cohort (Table 4).
There are two main strengths of the present study’s cohort. First, the sample size (n = 289) was relatively large, and the patients’ clinical backgrounds were well characterized. Second, the pathological diagnoses were performed and validated by three experienced liver-specific pathologists. Currently, the definitive diagnosis of NAFLD and the distinction of its phenotypes rely on the pathologist’s interpretation of the liver biopsy [8]; therefore, an accurate and reproducible consensus regarding the pathological findings is necessary for diagnosing NAFLD. However, in practice, the interpretation of NAFLD’s histology varies substantially. In this study, we excluded patients whose liver samples were inadequate for histological evaluation (e.g., because of insufficient sample size). Moreover, the considerable rate of inter-observer variation is one of the major problems in the histological diagnosis of NAFLD [13–17]. Our strategy mainly focused on reducing this variation, and our study may provide a reliable cohort for identifying surrogate markers and for investigating the management of NAFLD patients.
This study also has several limitations. First, we investigated the usefulness of the serum WFA+-M2BP values in a cross-sectional study. Therefore, the use of the serum WFA+-M2BP values for monitoring natural history, predicting outcomes, and predicting responses to therapeutic interventions remain unknown. In fact, the prevalence of NAFLD is high among individuals with diabetes or dyslipidemia [1–3], and some patients have already managed their condition through lifestyle interventions and/or medication at the time of liver biopsy. Further prospective studies are necessary to address these issues. In addition, since the biochemical analyses were performed separately at the respective hospitals, any variations among each institution cannot be ruled out. Moreover, several selection biases may be present, because all the patients had been diagnosed and had received liver biopsies at hepatology centers, which may have caused referral bias. Therefore, validation studies are necessary in the general population.
In conclusion, the measurement of the serum WFA+-M2BP values using a glycan-based immunoassay provides an accurate and reliable method for assessing the liver fibrosis stage in NAFLD patients. This method appears quite promising as a means for evaluating the natural course of the disease, therapeutic effects, and the suitability of liver biopsies.
References
Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221–31.
Bhala N, Usherwood T, George J. Non-alcoholic fatty liver disease. BMJ. 2009;339:b2474.
Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55:2005–23.
Adams LA, Lymp JF, StSauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–21.
Hui JM, Kench JG, Chitturi S, et al. Long-term outcomes of cirrhosis in nonalcoholic steatohepatitis compared with hepatitis C. Hepatology. 2003;38:420–7.
Yasui K, Hashimoto E, Komorizono Y, et al. Characteristics of patients with nonalcoholic steatohepatitis who develop hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2011;9:428–33.
Bhala N, Angulo P, van der Poorten D, et al. The natural history of nonalcoholic fatty liver disease with advanced fibrosis or cirrhosis: an international collaborative study. Hepatology. 2011;54:1208–16.
Brunt EM. Pathology of nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2010;7:195–203.
Laurin J. Motion—all patients with NASH need to have a liver biopsy: arguments against the motion. Can J Gastroenterol. 2002;16:722–6.
Sumida Y, Nakajima A, Itoh Y. Limitations of liver biopsy and non-invasive diagnostic tests for the diagnosis of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J Gastroenterol. 2014;20:475–85.
Cadranel JF, Rufat P, Degos F. Practices of liver biopsy in France: results of a prospective nationwide survey. Hepatology. 2000;32:477–81.
Ratziu V, Charlotte F, Heurtier A, et al. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005;128:1898–906.
Younossi ZM, Gramlich T, Liu YC, et al. Nonalcoholic fatty liver disease: assessment of variability in pathologic interpretations. Mod Pathol. 1998;11:560–5.
Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–21.
Fukusato T, Fukushima J, Shiga J, et al. Interobserver variation in the histopathological assessment of nonalcoholic steatohepatitis. Hepatol Res. 2005;33:122–7.
Miyaoka H, Michitaka K, Tokumoto Y, et al. Laparoscopic features and interobserver variation of histological diagnosis in patients with non-alcoholic fatty liver disease. Dig Endosc. 2008;20:22–8.
Gawrieh S, Knoedler DM, Saeian K, et al. Effects of interventions on intra- and interobserver agreement on interpretation of nonalcoholic fatty liver disease histology. Ann Diagon Pathol. 2011;15:19–24.
Suzuki A, Angulo P, Lymp J, et al. Hyaluronic acid, an accurate serum marker for severe hepatic fibrosis in patients with non-alcoholic fatty liver disease. Liver Int. 2005;25:779–86.
Yoneda M, Mawatari H, Fujita K, et al. Type IV collagen 7 s domain is an independent clinical marker of the severity of fibrosis in patients with nonalcoholic steatohepatitis before the cirrhotic stage. J Gastroenterol. 2007;42:375–81.
Vallet-Pichard A, Mallet V, Nalpas B, et al. FIB-4: an inexpensive and accurate marker of fibrosis in HCV infection. Comparison with liver biopsy and fibrotest. Hepatology. 2007;46:32–6.
Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45:846–54.
Harrison SA, Oliver D, Arnold HL, et al. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut. 2008;57:1441–7.
Guha IN, Parkes J, Roderick P, et al. Noninvasive markers of fibrosis in nonalcoholic fatty liver disease: validating the European Liver Fibrosis Panel and exploring simple markers. Hepatology. 2008;47:455–60.
Wong VW, Vergniol J, Wong GL, et al. Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology. 2010;51:454–62.
Yoneda M, Suzuki K, Kato S, et al. Nonalcoholic fatty liver disease: US-based acoustic radiation force impulse elastography. Radiology. 2010;256:640–7.
Ochi H, Hirooka M, Koizumi Y, et al. Real-time tissue elastography for evaluation of hepatic fibrosis and portal hypertension in nonalcoholic fatty liver diseases. Hepatology. 2012;56:1271–8.
Kuno A, Ikehara Y, Tanaka Y, et al. A serum “sweet-doughnut” protein facilitates fibrosis evaluation and therapy assessment in patients with viral hepatitis. Sci Rep. 2013;3:1065.
Kuno A, Sato T, Shimazaki H, et al. Reconstruction of a robust glycodiagnostic agent supported by multiple lectin-assisted glycan profiling. Proteomics Clin Appl. 2013. doi:10.1002/prca.201300010.
Ito K, Kuno A, Ikehara Y, et al. LecT-Hepa, a glyco-marker derived from multiple lectins, as a predictor of liver fibrosis in chronic hepatitis C patients. Hepatology. 2012;56:1448–56.
Toshima T, Shirabe K, Ikegami T, et al. A novel serum marker, glycosylated Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA+ -M2BP), for assessing liver fibrosis. J Gastroenterol. 7 Mar 2014 (Epub ahead of print).
Yamasaki K, Tateyama M, Abiru S, et al. Elevated serum levels of Wisteria floribunda agglutinin-positive human Mac-2 binding protein predict the development of hepatocellular carcinoma in hepatitis C patients. Hepatology. 12 Jul 2014. doi: 10.1002/hep.27305. (Epub ahead of print).
Brunt EM, Janney CG, Di Bisceglie AM, et al. Nonalcoholic steatohepatitis: a proposal for grading and staging the histological lesions. Am J Gastroenterol. 1999;94:2467–74.
Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26.
Iacobelli S, Arnò E, D’Orazio A, et al. Detection of antigens recognized by a novel monoclonal antibody in tissue and serum from patients with breast cancer. Cancer Res. 1986;46:3005–10.
Artini M, Natoli C, Tinari N, et al. Elevated serum levels of 90 K/MAC-2 BP predict unresponsiveness to alpha-interferon therapy in chronic HCV hepatitis patients. J Hepatol. 1996;25:212–7.
Inohara H, Akahani S, Koths K, et al. Interactions between galectin-3 and Mac-2 binding protein mediate cell-cell adhesion. Cancer Res. 1996;56:4530–4.
Sasaki T, Brakebusch C, Engel J, et al. Mac-2 binding protein is a cell-adhesive protein of the extracellular matrix which self-assembles into ring-like structures and binds beta1 integrins, collagens and fibronectin. EMBO J. 1998;17:1606–13.
Cheung KJ, Tilleman K, Deforce D, et al. The HCV serum proteome: a search for fibrosis protein markers. J Viral Hepat. 2009;16:418–29.
Kamada Y, Fujii H, Fujii H, et al. Serum Mac-2 binding protein levels as a novel diagnostic biomarker for prediction of disease severity and nonalcoholic steatohepatitis. Proteomics Clin Appl. 14 June 2013. doi: 10.1002/prca.201200137. (Epub ahead of print).
Sumida Y, Yoneda M, Hyogo H, et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012;12:2.
Wong VW, Wong GL, Chim AM, et al. Validation of the NAFLD fibrosis score in a Chinese population with low prevalence of advanced fibrosis. Am J Gastroenterol. 2008;103:1682–8.
Acknowledgments
This study was supported by a Grant-in-Aid from the Ministry of Health, Labour, and Welfare of Japan. This research was performed by the Hepatitis Glyco-biomarker Study Group.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Abe, M., Miyake, T., Kuno, A. et al. Association between Wisteria floribunda agglutinin-positive Mac-2 binding protein and the fibrosis stage of non-alcoholic fatty liver disease. J Gastroenterol 50, 776–784 (2015). https://doi.org/10.1007/s00535-014-1007-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-014-1007-2