
Abstract
Pancreatic cancer remains one of the most difficult malignancies to treat. Significant developments in our understanding of pancreatic cancer biology have occurred over the past decade. One of the key advances has been the formulation of the cancer stem cell model of tumor growth and subsequent experimental proof of pancreatic cancer stem cell existence. Cancer stem cells contribute to pancreatic tumor growth and progression and are at least partially responsible for the relative resistance of the tumor to systemic chemotherapy and radiation. Significant questions remain about how the mutational profile of the tumor, the tumor microenvironment, and normal pancreatic developmental pathways contribute to pancreatic cancer stem cell biology. Answers to these questions will likely yield new therapeutic approaches for this deadly disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pancreatic ductal adenocarcinoma (PDA) remains one of the deadliest malignancies in the world. Approximately 250,000 people are diagnosed with the disease worldwide each year and about the same number die from it. These statistics have not significantly changed over the past several decades. It is diagnosed late in its progression because of its ability to grow and metastasize without any significant symptoms. Surgical resection is the only known curative therapy. Unfortunately more than 80% of patients presenting to the clinic are ineligible for such a procedure. The successfully resected patient population still only has an aggregate 20% 5-year survival rate with the best adjuvant systemic therapy. This is partly due to the significant chemotherapy and radiation resistance of the tumor.
One of the key concepts of tumor biology that has begun to gain wide acceptance in the past decade is the presence of cancer stem cells in many malignancies. Cancer stem cells (CSCs) are functionally analogous to somatic stem cells present in adult tissues. They have the ability to undergo symmetric and asymmetric cell division and thereby can self-renew as well as give rise to “differentiated” tumor cell progeny that forms the bulk of the tumor (reviewed in [1]). CSCs have also been found to be resistant to chemotherapy and radiation and are considered to be responsible for the lack of tumor response to these therapies or for tumor recurrence after completion of adjuvant therapy.
In this review, we will discuss the two main models of tumor growth, the clonal evolution and the cancer stem cell model. We review how CSCs have been defined and analyzed and how the two models of cancer progression can potentially be combined to form a more unified view of tumor biology. We also discuss how the presence of CSCs relates to the therapeutic resistance of pancreatic cancer and discuss some of the underlying molecular mechanisms for this resistance such as the epithelial–mesenchymal transition (EMT). We also survey the early efforts at targeting pancreatic CSCs as part of a comprehensive strategy to treat this dismal disease.
Models of tumor cell heterogeneity
Experimental observations of functional heterogeneity in tumor cells have been known for decades. Variations have been observed in cell population growth rates, ability to form new tumors, ability to metastasize, and resistance to systemic chemoradiotherapy [2]. Understanding the ability of distinct cell populations within tumors to support long-term tumor growth and formation of new tumors is key as we attempt to define if all tumor cells or only specific subpopulations should be targeted with our therapies. An influential review in 2001 described the clonal evolution and cancer stem cell models of tumor development as alternatives, which could explain the observed functional heterogeneity within tumor cell populations [1]. The clonal evolution model posited that most tumor cells are capable of supporting tumor growth, given the right environment. The cancer stem cell model predicted that although genetic diversity existed within the tumor, only a defined subpopulation of tumor cells with a distinct phenotype would reproducibly support tumor growth and have the ability to form new tumors. Subsequent work in hematological malignancies and solid tumors has led to further refinements of these two main models [2].
The key question of whether functionally distinct cells are phenotypically distinguishable from the bulk tumor was first approached in models of acute myeloid leukemia (AML). Seminal work by Dick et al. [3] identified a CD34+/CD38− subpopulation of human AML cells that was capable of long-term reconstitution and formation of several subtypes of AML in immunocompromised SCID mice. Follow-up work further suggested that in fact primitive human hematopoietic stem cells or progenitor cells were the target of leukemic transformation [4].
Support for the cancer stem cell model in solid malignancies did not appear until 2003, when Michael Clarke et al. [5] defined the CD44+/CD24− subpopulation of human breast cancer cells as the tumor-initiating cells using the NOD/SCID xenograft model. Multiple subsequent publications rapidly began to define similar subsets of CSCs in other solid malignancies including brain [6, 7], colon [8–10], and head and neck cancers [11].
First experimental observations of pancreatic CSCs were published in 2007 by our group [12] followed by a report by Heeschen et al. [13]. Our work utilized 10 primary human pancreatic cancer xenografts to define the CD44+/CD24+/ESA+ subpopulation of tumor cells as the CSCs. Dr. Heeschen’s group focused on the CD133+ stem cell marker and defined the CD133+ subpopulation as the CSCs from 11 primary human cancer samples and pancreatic cancer cell lines. Analysis of phenotypic overlap between these two cell subsets revealed 10–40% of CD44+/CD24+/ESA+ cells were also CD133+ [13]. Analysis of the CD133+ CSCs also led to the isolation of a CXCR4-expressing subpopulation, which was solely responsible for metastatic dissemination in an orthotopic injection mouse model of PDA. This suggested that CSCs are not only responsible for primary tumor growth, but may also drive subsequent metastatic spread.
Additional markers that may enrich for pancreatic CSCs have since been defined. Aldehyde dehydrogenase (ALDH1A1) has been used as a marker of CSCs in other malignancies. Recent work has demonstrated that ALDH+ cells, as tested by the ALDEFLUOR assay, are also enriched for pancreatic tumor-initiating cells [14, 15]. We have also recently defined a key role for c-Met, the hepatocyte growth factor (HGF) receptor, in pancreatic CSC biology [16]. An interesting observation remains that there is often only a partial overlap between the cell subpopulations as defined by the different marker combinations. In fact one of the confounding factors in the cancer stem cell field has been the use of disparate marker profiles by various groups. It is currently unclear if the partially overlapping subpopulations of cells represent distinct functional subsets of pancreatic CSCs or if the lack of overlap is simply due to different sorting techniques and staining methods used by the individual laboratories. Standardization of protocols and reagents and publication of full analysis and gating strategies will help to minimize technical reasons for the variability seen between different publications [17]. Functional validation in xenograft assays should serve as the gold standard to verify that true tumorigenic cells have been isolated, as in vitro analyses using established cell lines do not necessarily identify cancer stem cells [18].
Cancer stem cells and the genetic heterogeneity of tumors
Fearon and Vogelstein [19] published a genetic progression model of colorectal tumorigenesis. The direct implication of the study was that accumulation of genetic mutations in an irreversible fashion accompanies the progression of normal tissue through dysplasia to frank carcinoma. Detailed pathological analysis of human pancreatic cancer samples has revealed similar histologic progression from normal pancreas through pancreatic intraepithelial neoplasia (PanINs) to full-blown PDA [20]. Along with the histological changes, detailed genetic analyses established a specific temporal accumulation of specific genetic mutations most commonly seen in pancreatic cancers. Kras mutations are seen in more than 95% of pancreatic cancers and can be isolated from the lowest stage PanINs, whereas mutations or loss of the tumor suppressor genes p16/Ink4a, p53, and DPC4/Smad4 occurs later during the neoplastic progression. As genome sequencing technologies have drastically improved, more comprehensive analysis of individual pancreatic cancer genomes has been performed. This has revealed a significant heterogeneity between individual human tumors in terms of the full mutational complement and also identified an average of 64 mutations per tumor in a set of 24 primary human PDAs [21]. Despite the genetic heterogeneity of the tumors studied, the authors were able to identify common pathways affected by the genomic changes, which will require further biological validation in the future. Recent detailed analysis of different anatomical regions within the primary tumors and associated metastases demonstrated that metastatic lesions could be genetically traced to different subclones arising in distinct areas of the primary tumor [22, 23]. The overall implication from these genomic studies is that multiple genetic subclones are constantly evolving and competing in parallel within the primary tumor and that different subclones may independently give rise to metastatic lesions.
It is important to attempt to reconcile the genetic evidence supporting the clonal evolution model with the experimental studies of cancer stem cells. Recent work has begun to describe the genetic profiles of cancer stem cells in two distinct models of acute lymphocytic leukemia (ALL). Using copy number alteration analysis through single nucleotide polymorphism (SNP) arrays, Dick et al. [24] demonstrated genetically diverse leukemia-initiating cells in BCR-ABL1-driven ALL. Leukemic stem cells from the dominant genetic clone often also formed the dominant clone in recipient mice. However, in certain instances the minor subclone CSCs outcompeted the original clone and gave rise to a new dominant clone in the recipient animals. This increased aggressiveness was associated with specific genetic changes in the neoplastic cells such as the loss of CDKN2. This data suggests that genetic subclones may define different populations of CSCs with varying biologic aggressiveness. Greaves et al. [25] made similar observations about the leukemia-initiating cells in ETV6-RUNX1-driven ALL using multi-epitope, high-resolution fluorescence in situ hybridization analysis. This work reveals the same underlying genetic heterogeneity in CSCs that is seen in the bulk tumors. We currently do not understand how the genetic diversity of primary PDA correlates with the presence of pancreatic CSCs and how this relates to the biological aggressiveness of the various subclones of the tumor. This question will be exceedingly difficult to answer in primary human tumors, but use of animal models of pancreatic cancer may shed light upon this issue.
Genetically engineered mouse models of cancer have also been used to isolate and study CSCs. For example, multiple murine models of breast cancer exist based on overexpression of Wnt-1, neu, or loss of p53. CSC subpopulations have now been described in all three of these models [26–28]. It is interesting to note that the one study that analyzed the models concurrently was unable to find a common cell surface phenotype for the CSC subpopulation for all three models, although some overlap was noted on the basis of CD61/β3 integrin expression [27]. A recent study utilizing three genetically distinct mouse models of lung adenocarcinoma also demonstrated that tumors of different genetic backgrounds contained CSCs with disparate cell surface marker phenotypes [29]. Over the past decade new mouse models of pancreatic cancer have been described that recapitulate the pathology of the human disease [30–32]. These models rely on the introduction of the mutated Kras allele in the presence or absence of mutations in other tumor suppressors normally found in human PDA. It will be interesting to delineate the CSC populations in the tumors arising in these mice and to elucidate the relationship between specific genomic alterations and the functionality of CSCs. It is also noteworthy that in many instances, the CSC markers from murine models do not necessarily correspond to the markers determined from primary human tumor studies, highlighting potentially important differences between human biology and the corresponding genetically engineered mouse model systems.
One of the key assumptions underlying the cancer stem cell model is that the CSCs exist at the top of a developmental hierarchy and populate the tumor with descendant CSCs and more “differentiated” tumor cells via asymmetrical cell division. Another assumption implicit in the cancer stem cell model has been that no conversion occurs from the non-stem cancer cells to a cancer stem cell state. However, recent evidence has begun to point to the existence of significant functional plasticity in the stem and non-stem cancer cell populations. For example, signals from the tumor microenvironment, including HGF, can drive the conversion of colon cancer cells into a cancer stem cell state through enhancement of β-catenin signaling [33]. Two recent papers highlight the ability of normal breast epithelial cells and “differentiated” breast cancer cells to spontaneously transition into more stem-like states with enhanced ability to recapitulate breast gland development and enhanced tumorigenicity [34, 35]. Recent work in breast cancer cell lines has also led to the development of a model of stochastic transitions between the breast luminal, basal, and stem-like cells [36]. The mechanisms underlying the spontaneous conversion of non-stem cells to cancer stem cells are mostly unknown, but in breast cancer cells, IL-6 signaling seems to play a role [35]. These results agree with a recent paper highlighting the role of IL-6/JAK2/STAT3 signaling in the maintenance of CD44+/CD24− cancer stem cells in human breast carcinomas [37]. Of note, the IL-6/STAT3 signaling axis has been directly implicated in both human and murine PDA initiation and progression [38, 39]. It is unclear if IL-6 signaling contributes to pancreatic CSC biology and this forms an excellent question to address experimentally in the future. The other implication of the studies above is that the original model of cellular functional hierarchy based on normal stem cell biology may not necessarily apply in the case of CSCs [34–36]. Here the additional plasticity of the tumor subpopulations allows for potential interconversion between stem and non-stem cell states, which may be regulated by multiple factors including the tumor microenvironment.
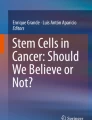
It will be important to reconcile the genetic evidence for the clonal selection model with the evidence of functional heterogeneity supporting the cancer stem cell model. At this point the evidence in some cancer types seems to suggest a model where multiple genetic subclones contain varying proportions of CSCs with distinct genetic backgrounds (Fig. 1). This can potentially explain the presence of dominant and minor clones and why cancers often relapse after systemic therapy. As cancer stem cells have been shown to be more resistant to chemoradiation than the rest of the tumor cell population, this selective pressure would automatically select the genetic clones that contain a higher proportion of cancer stem cells and thereby have higher potential for reconstituting tumor growth once the therapeutic regimen is finished. It will be necessary to better delineate the relationship of the genetic background of the tumor to the frequency and functionality of the cancer stem cell subpopulation in human PDA to design better therapeutic approaches in the future.

Cancer stem cells within genetic subclones of a pancreatic tumor. Recent data suggest a common model of tumorigenesis with facets of clonal selection and cancer stem cell biology. The pancreatic tumor is composed of distinct genetic clones, each of which contains its own population of cancer stem cells that drive the clone’s proliferation. The cancer stem cells maintain the capacity for self-renewal and for generation of non-stem cell progeny by asymmetric division. A possibility for generation of cancer stem cells from bulk tumor cells is not excluded given recent evidence from multiple breast cancer models (see text)
Developmental pathway dysregulation in PDA
Experimental work over the past decade has begun to delineate the contribution of reactivated developmental signaling pathways in pancreatic cancer initiation and progression [40]. For example, we have begun to appreciate that the neoplastic pancreas upregulates Hedgehog signaling proteins and that these are crucial to pancreatic cancer progression [41, 42]. Hedgehog ligands activate intracellular signaling by binding to the canonical cell surface receptor patched (Ptch) in the primary cilium. Ptch then moves out of the primary cilium allowing smoothened (Smo) to enter the structure and activate the Gli family of transcription factors, which play a key role in carcinogenesis and stem cell modulation [43]. The adult pancreas does not normally express Hedgehog ligands. In contrast, the neoplastic epithelium secretes the Hedgehog ligands, which subsequently activate the canonical signaling pathway in tumor stromal cells [44–46]. Recent work using genetically engineered mouse models has shown that disruption of the Hedgehog signaling pathway leads to increased vascularity of the tumors and allows for better chemotherapeutic delivery to the neoplastic tissues [47].
Hedgehog signaling has also been shown to be involved in pancreatic CSC function. In our original work, we demonstrated that the CD44+/CD24+/ESA+ CSC population has marked upregulation of expression of Sonic hedgehog (Shh) [12]. On the basis of this data, one might hypothesize that the CSC population is responsible for driving the neoplastic stroma generation. In a separate study, blocking of Shh signaling with cyclopamine led to a decrease in the proportion of CD133+ CSCs found in pancreatic cancer cell lines, decrease in the metastatic potential of tumor cells, and in conjunction with gemcitabine and rapamycin led to a decrease in overall in vivo tumorigenicity [48]. This data intimately implicates Hh signaling in the biology of pancreatic cancer and multiple clinical trials utilizing Hh inhibitors are now underway to test their efficacy in treating pancreatic cancer. It still remains unclear if Hh signaling directly supports CSC survival or indirectly stimulates signals from the tumor microenvironment that support the cancer stem cell niche.
Wnt/β-catenin signaling is intimately involved in many developmental and neoplastic processes. Expression of β-catenin increases progressively in PanINs and PDA and its localization changes from the classical membranous distribution to increased cytoplasmic and nuclear localization with tumor progression [49]. Upregulation of β-catenin and the downstream transcription factor Tcf4 was observed in transgenic murine models of PDA and multiple Wnt ligands and signaling components were expressed in pancreatic cancer cell lines [50]. We have also shown previously that overexpression of ataxia-telangiectasia group D (ATDC, also known as TRIM29), which is found in the majority of human PDA, leads to the stabilization of β-catenin protein levels by Disheveled-mediated inhibition of glycogen synthase kinase-3β (GSK-3β), which normally phosphorylates β-catenin leading to its degradation [51]. Stabilization of β-catenin and corresponding increased intracellular protein levels correlate with increased proliferation of pancreatic cancer cells.
Direct involvement of β-catenin signaling in pancreatic CSC biology has not been formally demonstrated yet, but evidence from other malignancies suggests that this pathway may play a key role in CSC biology. Disruption of β-catenin led to a significant decrease of CD34+ skin CSCs in murine models of squamous cell carcinoma, which correlated with established tumor regression [52]. β-Catenin signaling also plays a key role in colon cancer and in hematopoietic stem cell biology [53]. Medema et al. [33] demonstrated that myofibroblasts secreting HGF induce β-catenin signaling in adjacent colon cancer cells and thereby promote their in vitro clonogenicity and in vivo tumorigenicity. These findings are interesting in the light of our recent work highlighting the role of c-Met, the HGF receptor, in pancreatic CSC biology [16]. It will be important to delineate more precisely how Wnt/β-catenin signaling contributes to the function of pancreatic CSCs.
Cancer stem cells, EMT, and therapeutic resistance
Multiple studies from diverse systems have now demonstrated that standard chemotherapy and radiation often select for the underlying CSC subsets in the treated tumors. Rich et al. [54] analyzed the responses of glioma CD133+ stem cells to radiotherapy and determined that the CSCs were more resistant to irradiation by more efficient upregulation of the DNA damage response. Work utilizing colon CSCs demonstrated they are preferentially resistant to standard chemotherapy in an IL-4-dependent manner [55]. Analysis of the CD44+/ESA+ colon CSC subset revealed it to be enriched in tumors after chemotherapy. Inhibition of ALDH1A1, an enzymatic marker of stem cells in many systems, resensitized the colon CSCs to chemotherapy [56]. In breast cancers, standard chemotherapy regimens increased the proportion of CD44+/CD24− breast CSCs in matched breast cancer biopsies before and after chemotherapy [57]. In this system, addition of lapatinib, a Her2/neu inhibitor, led to an abrogation of this CSC frequency increase. These results suggest that standard systemic therapy often either selects for or induces the formation of CSCs and that targeted molecular therapy may allow us to target this resistant subpopulation of cancer cells.
A key functional transition that appears to play a role in cancer stem cell therapeutic resistance is the epithelial–mesenchymal transition (EMT). Weinberg et al. [58] demonstrated that inducing EMT in breast cancer cells also forces the cells to transition into the CD44+/CD24− breast CSC state. Recent gene expression profiling analysis of human and murine pancreatic cancer cell samples revealed three distinct tumor types: classical epithelial, quasimesenchymal, and endocrine-like type [59]. Presence of the quasimesenchymal signature correlated with poor patient prognosis and differential sensitivity to EGF-based therapy. The quasimesenchymal signature included significant downregulation of E-cadherin and upregulation of Twist1, a transcription factor important for EMT. In other published experiments, siRNA-based inhibition of Zeb1, another EMT transcription factor, in Panc-1 cells led to a decrease of primary xenograft tumor size, number of metastases, and tumorsphere-forming ability [60]. Poorly differentiated human cancers also express high levels of Zeb1. Further analysis revealed that Zeb1 inhibits the expression of the miRNA-200 cluster and thereby promotes EMT and stemness in pancreatic cancer cells. Direct inhibition of Zeb1 led to reversion to an epithelial phenotype and increased sensitivity to gemcitabine and cisplatin [60, 61]. In a study by Shah et al. [62] generation of gemcitabine-resistant subclones of established pancreatic cancer cell lines resulted in the loss of E-cadherin and higher levels of nuclear β-catenin and Twist. Gemcitabine resistance correlated with an increased proportion of CD44+/CD24+/ESA+ cells in the cell lines. Together, this data implicates both the EMT and cancer stem cell phenotypes in the chemoresistance seen in pancreatic cancer. How the process of EMT relates to the generation and maintenance of the CSC phenotype in PDA remains unclear. Novel therapeutic approaches may potentially be designed that interfere with the maintenance of both of these states to effectively treat pancreatic cancer in the future.
Therapeutic targeting of cancer stem cells
Early forays into CSC-targeted therapies have been made. One particular pathway that may serve as a good therapeutic target is the PI3K/Akt/mTOR pathway. This signaling pathway has been previously implicated in the maintenance of breast, prostate, and leukemic stem cells [63–65]. Additionally, perivascular medulloblastoma stem cells exhibit resistance to radiation therapy and require Akt activity for their survival [66]. Rapamycin targets the mTOR pathway and has been demonstrated to have efficacy against pancreatic and leukemic stem cells [48, 64]. Leukemic stem cells require mTOR for survival unlike normal hematopoietic stem cells and rapamycin therapy leads to leukemic stem cell depletion [64, 67]. Rapamycin therapy of human pancreatic cancer xenografts leads to pancreatic CSC depletion and this becomes even more pronounced when it is combined with gemcitabine and cyclopamine, a Smoothened inhibitor that abrogates Hedgehog signaling [48]. These early results support the idea that specific targeted therapies preferentially affecting the CSC population may be found.
We have recently discovered that expression of c-Met, the HGF receptor, identifies pancreatic CSCs along with high levels of CD44 [16]. In our work, we also demonstrated that using XL184, a c-Met inhibitor, led to depletion of the pancreatic CSCs and decreased tumorsphere-forming capacity and in vivo tumorigenicity of the treated cells. c-Met inhibition was synergistic with standard gemcitabine chemotherapy in our preclinical primary human PDA orthotopic xenograft models [16]. These approaches reveal the possibility of development of CSC-targeted therapies that can potentially be used alongside standard chemotherapeutic regimens to specifically eliminate the CSC subpopulations and further reduce tumor recurrence. One caveat to this approach is the emerging data about tumor cell functional plasticity discussed earlier in this review. It will be important to verify that the chemotherapies do not eradicate existing CSCs that could then simply be replaced from a surviving pool of bulk cancer cells. It is likely that the most efficacious therapeutic strategies in the future will combine targeting of both the CSC and non-stem cell compartments to achieve the fullest effect.
Conclusions
Pancreatic cancer remains an extremely difficult clinical problem. Despite this we have begun to make headway in the past decade in our understanding of the underlying biology, which has resulted in the development of new therapeutic approaches currently being tested in clinical trials. Our insight into the genetic basis of PDA initiation and progression has allowed us for the first time to develop animal models of the disease which closely recapitulate the human pathological process. The parallel emergence of the cancer stem cell field over the past 20 years has led to the isolation of these functionally important cells in primary human pancreatic tumors. We should strive to combine these newly developed tools and insights to better delineate how the underlying genetic diversity of the pancreatic tumor leads to functional cell heterogeneity culminating in the generation and maintenance of pancreatic CSCs. This information should yield new therapeutic approaches for this disease.
Studies have begun to define the contribution of dysregulated developmental pathways to pancreatic tumor initiation and growth. These basic biological studies have now led to preclinical testing of Hedgehog, Wnt, and Notch inhibitors in genetically engineered mouse models and primary human tumor xenograft models of PDA. Based on the promising results in these preclinical models, multiple clinical trials are now taking place utilizing these agents as single therapy or in combination with standard chemotherapy. It is not yet completely clear how these pathways interact together in the tumor microenvironment and tumor epithelium to drive the process of tumorigenesis through cancer stem cell generation and maintenance. It is conceivable that delineating these mechanisms will allow us to better tailor the multi-agent chemotherapy that is needed to treat pancreatic cancer.
The key aspect of cancer stem cell biology that is therapeutically relevant is CSC resistance to current systemic therapy. We still have very little understanding of the underlying molecular mechanisms of this resistance. On the basis of the preliminary studies with rapamycin and XL184, the c-Met inhibitor, it is possible that clinically relevant molecularly targeted therapy against pancreatic cancer stem cells can exist. How these therapies break the resistance mechanisms seen in previous work remains an important question for further study. We remain hopeful that meaningful clinical improvement for our patients will result from these future experiments.
References
Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells. Nature. 2001;414:105–11.
Dick JE. Stem cell concepts renew cancer research. Blood. 2008;112:4793–807.
Lapidot T, Sirard C, Vormoor J, Murdoch B, Hoang T, Caceres-Cortes J, et al. A cell initiating human acute myeloid leukaemia after transplantation into SCID mice. Nature. 1994;367:645–8.
Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3:730–7.
Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci USA. 2003;100:3983–8.
Singh SK, Clarke ID, Terasaki M, Bonn VE, Hawkins C, Squire J, et al. Identification of a cancer stem cell in human brain tumors. Cancer Res. 2003;63:5821–8.
Singh SK, Hawkins C, Clarke ID, Squire JA, Bayani J, Hide T, et al. Identification of human brain tumour initiating cells. Nature. 2004;432:396–401.
Dalerba P, Dylla SJ, Park IK, Liu R, Wang X, Cho RW, et al. Phenotypic characterization of human colorectal cancer stem cells. Proc Natl Acad Sci USA. 2007;104:10158–63.
O’Brien CA, Pollett A, Gallinger S, Dick JE. A human colon cancer cell capable of initiating tumour growth in immunodeficient mice. Nature. 2007;445:106–10.
Ricci-Vitiani L, Lombardi DG, Pilozzi E, Biffoni M, Todaro M, Peschle C, et al. Identification and expansion of human colon-cancer-initiating cells. Nature. 2007;445:111–5.
Prince ME, Sivanandan R, Kaczorowski A, Wolf GT, Kaplan MJ, Dalerba P, et al. Identification of a subpopulation of cells with cancer stem cell properties in head and neck squamous cell carcinoma. Proc Natl Acad Sci USA. 2007;104:973–8.
Li C, Heidt DG, Dalerba P, Burant CF, Zhang L, Adsay V, et al. Identification of pancreatic cancer stem cells. Cancer Res. 2007;67:1030–7.
Hermann PC, Huber SL, Herrler T, Aicher A, Ellwart JW, Guba M, et al. Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell. 2007;1:313–23.
Kim MP, Fleming JB, Wang H, Abbruzzese JL, Choi W, Kopetz S, et al. ALDH activity selectively defines an enhanced tumor-initiating cell population relative to CD133 expression in human pancreatic adenocarcinoma. PLoS One. 2011;6:e20636.
Rasheed ZA, Yang J, Wang Q, Kowalski J, Freed I, Murter C, et al. Prognostic significance of tumorigenic cells with mesenchymal features in pancreatic adenocarcinoma. J Natl Cancer Inst. 2010;102:340–51.
Li C, Wu JJ, Hynes M, Dosch J, Sarkar B, Welling TH, et al. c-Met is a Marker of pancreatic cancer stem cells and therapeutic target. Gastroenterology. 2011. doi:10.1053/j.gastro.2011.08.009.
Alexander CM, Puchalski J, Klos KS, Badders N, Ailles L, Kim CF, et al. Separating stem cells by flow cytometry: reducing variability for solid tissues. Cell Stem Cell. 2009;5:579–83.
Pastrana E, Silva-Vargas V, Doetsch F. Eyes wide open: a critical review of sphere-formation as an assay for stem cells. Cell Stem Cell. 2011;8:486–98.
Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–67.
Hruban RH, Goggins M, Parsons J, Kern SE. Progression model for pancreatic cancer. Clin Cancer Res. 2000;6:2969–72.
Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, et al. Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science. 2008;321:1801–6.
Campbell PJ, Yachida S, Mudie LJ, Stephens PJ, Pleasance ED, Stebbings LA, et al. The patterns and dynamics of genomic instability in metastatic pancreatic cancer. Nature. 2010;467:1109–13.
Yachida S, Jones S, Bozic I, Antal T, Leary R, Fu B, et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature. 2010;467:1114–7.
Notta F, Mullighan CG, Wang JC, Poeppl A, Doulatov S, Phillips LA, et al. Evolution of human BCR-ABL1 lymphoblastic leukaemia-initiating cells. Nature. 2011;469:362–7.
Anderson K, Lutz C, van Delft FW, Bateman CM, Guo Y, Colman SM, et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature. 2011;469:356–61.
Cho RW, Wang X, Diehn M, Shedden K, Chen GY, Sherlock G, et al. Isolation and molecular characterization of cancer stem cells in MMTV-Wnt-1 murine breast tumors. Stem Cells. 2008;26:364–71.
Vaillant F, Asselin-Labat ML, Shackleton M, Forrest NC, Lindeman GJ, Visvader JE. The mammary progenitor marker CD61/beta3 integrin identifies cancer stem cells in mouse models of mammary tumorigenesis. Cancer Res. 2008;68:7711–7.
Zhang M, Behbod F, Atkinson RL, Landis MD, Kittrell F, Edwards D, et al. Identification of tumor-initiating cells in a p53-null mouse model of breast cancer. Cancer Res. 2008;68:4674–82.
Curtis SJ, Sinkevicius KW, Li D, Lau AN, Roach RR, Zamponi R, et al. Primary tumor genotype is an important determinant in identification of lung cancer propagating cells. Cell Stem Cell. 2010;7:127–33.
Aguirre AJ, Bardeesy N, Sinha M, Lopez L, Tuveson DA, Horner J, et al. Activated Kras and Ink4a/Arf deficiency cooperate to produce metastatic pancreatic ductal adenocarcinoma. Genes Dev. 2003;17:3112–26.
Hingorani SR, Petricoin EF, Maitra A, Rajapakse V, King C, Jacobetz MA, et al. Preinvasive and invasive ductal pancreatic cancer and its early detection in the mouse. Cancer Cell. 2003;4:437–50.
Hingorani SR, Wang L, Multani AS, Combs C, Deramaudt TB, Hruban RH, et al. Trp53R172H and KrasG12D cooperate to promote chromosomal instability and widely metastatic pancreatic ductal adenocarcinoma in mice. Cancer Cell. 2005;7:469–83.
Vermeulen L, De Sousa EMF, van der Heijden M, Cameron K, de Jong JH, Borovski T, et al. Wnt activity defines colon cancer stem cells and is regulated by the microenvironment. Nat Cell Biol. 2010;12:468–76.
Chaffer CL, Brueckmann I, Scheel C, Kaestli AJ, Wiggins PA, Rodrigues LO, et al. Normal and neoplastic nonstem cells can spontaneously convert to a stem-like state. Proc Natl Acad Sci USA. 2011;108:7950–5.
Iliopoulos D, Hirsch HA, Wang G, Struhl K. Inducible formation of breast cancer stem cells and their dynamic equilibrium with non-stem cancer cells via IL6 secretion. Proc Natl Acad Sci USA. 2011;108:1397–402.
Gupta PB, Fillmore CM, Jiang G, Shapira SD, Tao K, Kuperwasser C, et al. Stochastic state transitions give rise to phenotypic equilibrium in populations of cancer cells. Cell. 2011;146:633–44.
Marotta LL, Almendro V, Marusyk A, Shipitsin M, Schemme J, Walker SR, et al. The JAK2/STAT3 signaling pathway is required for growth of CD44CD24 stem cell-like breast cancer cells in human tumors. J Clin Invest. 2011;121:2723–35.
Fukuda A, Wang SC, Morris JP 4th, Folias AE, Liou A, Kim GE, et al. Stat3 and MMP7 contribute to pancreatic ductal adenocarcinoma initiation and progression. Cancer Cell. 2011;19:441–55.
Lesina M, Kurkowski MU, Ludes K, Rose-John S, Treiber M, Kloppel G, et al. Stat3/Socs3 activation by IL-6 transsignaling promotes progression of pancreatic intraepithelial neoplasia and development of pancreatic cancer. Cancer Cell. 2011;19:456–69.
Morris JP 4th, Wang SC, Hebrok M. KRAS, Hedgehog, Wnt and the twisted developmental biology of pancreatic ductal adenocarcinoma. Nat Rev Cancer. 2010;10:683–95.
Berman DM, Karhadkar SS, Maitra A, Montes De Oca R, Gerstenblith MR, Briggs K, et al. Widespread requirement for Hedgehog ligand stimulation in growth of digestive tract tumours. Nature. 2003;425:846–51.
Thayer SP, di Magliano MP, Heiser PW, Nielsen CM, Roberts DJ, Lauwers GY, et al. Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature. 2003;425:851–6.
Ruiz i Altaba A, Mas C, Stecca B. The Gli code: an information nexus regulating cell fate, stemness and cancer. Trends Cell Biol. 2007;17:438–47.
Tian H, Callahan CA, DuPree KJ, Darbonne WC, Ahn CP, Scales SJ, et al. Hedgehog signaling is restricted to the stromal compartment during pancreatic carcinogenesis. Proc Natl Acad Sci USA. 2009;106:4254–9.
Walter K, Omura N, Hong SM, Griffith M, Vincent A, Borges M, et al. Overexpression of smoothened activates the sonic hedgehog signaling pathway in pancreatic cancer-associated fibroblasts. Clin Cancer Res. 2010;16:1781–9.
Yauch RL, Gould SE, Scales SJ, Tang T, Tian H, Ahn CP, et al. A paracrine requirement for hedgehog signalling in cancer. Nature. 2008;455:406–10.
Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D, Honess D, et al. Inhibition of Hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science. 2009;324:1457–61.
Mueller MT, Hermann PC, Witthauer J, Rubio-Viqueira B, Leicht SF, Huber S, et al. Combined targeted treatment to eliminate tumorigenic cancer stem cells in human pancreatic cancer. Gastroenterology. 2009;137:1102–13.
Al-Aynati MM, Radulovich N, Riddell RH, Tsao MS. Epithelial-cadherin and beta-catenin expression changes in pancreatic intraepithelial neoplasia. Clin Cancer Res. 2004;10:1235–40.
Pasca di Magliano M, Biankin AV, Heiser PW, Cano DA, Gutierrez PJ, Deramaudt T, et al. Common activation of canonical Wnt signaling in pancreatic adenocarcinoma. PLoS One. 2007;2:e1155.
Wang L, Heidt DG, Lee CJ, Yang H, Logsdon CD, Zhang L, et al. Oncogenic function of ATDC in pancreatic cancer through Wnt pathway activation and beta-catenin stabilization. Cancer Cell. 2009;15:207–19.
Malanchi I, Peinado H, Kassen D, Hussenet T, Metzger D, Chambon P, et al. Cutaneous cancer stem cell maintenance is dependent on beta-catenin signalling. Nature. 2008;452:650–3.
Reya T, Clevers H. Wnt signalling in stem cells and cancer. Nature. 2005;434:843–50.
Bao S, Wu Q, McLendon RE, Hao Y, Shi Q, Hjelmeland AB, et al. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature. 2006;444:756–60.
Todaro M, Alea MP, Di Stefano AB, Cammareri P, Vermeulen L, Iovino F, et al. Colon cancer stem cells dictate tumor growth and resist cell death by production of interleukin-4. Cell Stem Cell. 2007;1:389–402.
Dylla SJ, Beviglia L, Park IK, Chartier C, Raval J, Ngan L, et al. Colorectal cancer stem cells are enriched in xenogeneic tumors following chemotherapy. PLoS One. 2008;3:e2428.
Li X, Lewis MT, Huang J, Gutierrez C, Osborne CK, Wu MF, et al. Intrinsic resistance of tumorigenic breast cancer cells to chemotherapy. J Natl Cancer Inst. 2008;100:672–9.
Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A, Zhou AY, et al. The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell. 2008;133:704–15.
Collisson EA, Sadanandam A, Olson P, Gibb WJ, Truitt M, Gu S, et al. Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat Med. 2011;17:500–3.
Wellner U, Schubert J, Burk UC, Schmalhofer O, Zhu F, Sonntag A, et al. The EMT-activator ZEB1 promotes tumorigenicity by repressing stemness-inhibiting microRNAs. Nat Cell Biol. 2009;11:1487–95.
Arumugam T, Ramachandran V, Fournier KF, Wang H, Marquis L, Abbruzzese JL, et al. Epithelial to mesenchymal transition contributes to drug resistance in pancreatic cancer. Cancer Res. 2009;69:5820–8.
Shah AN, Summy JM, Zhang J, Park SI, Parikh NU, Gallick GE. Development and characterization of gemcitabine-resistant pancreatic tumor cells. Ann Surg Oncol. 2007;14:3629–37.
Dubrovska A, Kim S, Salamone RJ, Walker JR, Maira SM, Garcia-Echeverria C, et al. The role of PTEN/Akt/PI3K signaling in the maintenance and viability of prostate cancer stem-like cell populations. Proc Natl Acad Sci USA. 2009;106:268–73.
Lee JY, Nakada D, Yilmaz OH, Tothova Z, Joseph NM, Lim MS, et al. mTOR activation induces tumor suppressors that inhibit leukemogenesis and deplete hematopoietic stem cells after Pten deletion. Cell Stem Cell. 2010;7:593–605.
Zhou J, Wulfkuhle J, Zhang H, Gu P, Yang Y, Deng J, et al. Activation of the PTEN/mTOR/STAT3 pathway in breast cancer stem-like cells is required for viability and maintenance. Proc Natl Acad Sci USA. 2007;104:16158–63.
Hambardzumyan D, Becher OJ, Rosenblum MK, Pandolfi PP, Manova-Todorova K, Holland EC. PI3K pathway regulates survival of cancer stem cells residing in the perivascular niche following radiation in medulloblastoma in vivo. Genes Dev. 2008;22:436–48.
Yilmaz OH, Valdez R, Theisen BK, Guo W, Ferguson DO, Wu H, et al. Pten dependence distinguishes haematopoietic stem cells from leukaemia-initiating cells. Nature. 2006;441:475–82.
Acknowledgments
The authors wish to express their gratitude to the Japanese Society of Gastroenterology for the opportunity to publish this work. Our work was supported by funding from the Department of Defense, the American College of Surgeons, the Lustgarten Foundation, the Pardee Foundation, the Program for Organogenesis at the University of Michigan, and from the Randy Pausch Family AACR-Pancreatic Cancer Action Network Innovation Award.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bednar, F., Simeone, D.M. Pancreatic cancer stem cell biology and its therapeutic implications. J Gastroenterol 46, 1345–1352 (2011). https://doi.org/10.1007/s00535-011-0494-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-011-0494-7