
Abstract
Background
Anti-gp210 and anti-centromere antibodies are different risk factors for the progression of primary biliary cirrhosis (PBC). In order to dissect the genetic basis for the production of these autoantibodies, as well as the development and progression of PBC in Japanese patients, we examined single nucleotide polymorphisms (SNPs) in cytotoxic T-lymphocyte antigen 4 (CTLA4) and solute carrier family 4 anion exchanger, member 2 (SLC4A2), which have been associated with the pathogenesis of PBC in Caucasian patients.
Methods
Four SNPs for both CTLA4 and SLC4A2 were genotyped, using the polymerase chain reaction–restriction fragment length polymorphism method and TaqMan assay, in 450 Japanese PBC patients and 371 sex-matched healthy controls.
Results
The CTLA4 rs231775, rs3087243, and rs231725 SNPs were significantly associated with PBC susceptibility. The CTLA4 rs231725 SNP was significantly associated with progression to late-stage disease. The CTLA-4 haplotype 1 (rs231775 G, rs231777 C, rs3087243 G, rs231725 A; GCGA) was a risk factor for PBC susceptibility but a protective factor for PBC progression. Conversely, the CTLA-4 haplotype 2 (ACAG) was a protective and risk factor, respectively, for PBC susceptibility and progression. In addition, the CTLA4 rs231777 SNP and haplotype 3 (ATGG) was significantly associated with anti-gp210 antibody production, while SLC4A2 haplotype 4 (rs2069443 A, rs2303933 G, rs2303937 A, rs2303941 T; AGAT) and haplotype 3 (AAGC) were significantly associated with PBC susceptibility and anti-centromere antibody production, respectively.
Conclusions
CTLA4 and SLC4A2 genetic polymorphisms are differentially associated with PBC development and progression, as well as anti-gp210 or anti-centromere antibody production, in Japanese PBC patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Primary biliary cirrhosis (PBC) is a chronic liver disease that leads to the destruction of intrahepatic bile ducts, progressive cholestasis, and eventually liver cirrhosis. Although the pathogenesis of PBC is still unknown, frequent familial clusters and a high concordance rate in monozygotic twins suggest that genetic backgrounds strongly influence PBC pathogenesis [1].
Many candidate gene association studies have been performed and several single nucleotide polymorphisms (SNPs) have been associated with PBC, including human leukocyte antigen (HLA), cytotoxic T-lymphocyte antigen 4 (CTLA4), solute carrier family 4 anion exchanger, member 2 (SLC4A2), tumor necrosis factor, and programmed cell death 1 and multidrug resistance protein 3 [2–13]. In addition to these genes, recent genome-wide association studies have revealed that IL12A, IL12RB2, IRF5-TNPO3, 17q12-21, and MMEL1 loci were associated with PBC susceptibility in Caucasians [14–16].
CTLA4 is predominantly expressed on activated and regulatory T cells, where it functions as a co-inhibitory molecule that interacts with B7.1 (CD80) and B7.2 (CD86) that are expressed on antigen-presenting cells. Many studies have shown that CTLA4 genetic polymorphisms are associated with disease susceptibility and severity in various autoimmune diseases, such as type I diabetes, rheumatoid arthritis, and Grave’s disease [17, 18]. However, studies on the association between PBC and CTLA4 genetic polymorphisms have yielded conflicting results among different ethnic groups, and only a limited number of studies have assessed autoantibody production [6, 8, 19–21].
SLC4A2, which is occasionally referred to as anion exchanger 2, is distributed in various tissues and functions as an Na+-independent Cl−/HCO3 − exchanger that regulates intracellular and transepithelial acid–base transport, including bicarbonate secretion into bile in cholangiocytes [22, 23]. SLC4A2 expression in liver biopsy sections, as well as in peripheral blood mononuclear cells, was significantly reduced in PBC patients compared to healthy subjects and patients with non-PBC liver diseases [24, 25]. In addition, the in vitro activity of SLC4A2 in cholangiocytes was lower in PBC patients as compared to healthy subjects or patients with non-PBC liver diseases [26]. These reports indicated that SLC4A2 might be involved in the pathogenesis of PBC. Indeed, SLC4A2 genetic polymorphisms were associated with anti-mitochondrial antibody (AMA) production and PBC progression during ursodeoxycholic acid (UDCA) treatment in Caucasian patients [11, 20].
We previously reported that anti-gp210 and anti-centromere antibodies were differentially associated with PBC progression; the presence of anti-gp210 antibodies is a strong risk factor for progression to hepatic failure, while a positive anti-centromere antibody status is a significant risk factor for progression to portal hypertension [27]. These results may imply that several different genetic polymorphisms are potentially involved in the production of these autoantibodies as well as PBC progression. However, aside from HLA studies, there are no data on genetic polymorphisms that are associated with the production of these autoantibodies [3].
In the present study, we dissected the genetic basis for the production of these autoantibodies, as well as PBC development and progression, by examining CTLA4 and SLC4A2 SNPs, which have been reportedly associated with disease susceptibility and progression, as well as AMA production, in Caucasian PBC patients [8, 9, 11–13, 20, 21].
Methods
Subjects
The study subjects included 450 PBC patients and 371 healthy controls, who were enrolled in two different PBC cohort studies that included the National Hospital Organization Study Group for Liver Disease in Japan (NHOSLJ) (cohort 1) and the Shinshu PBC Study Group in Japan (cohort 2). Patients were diagnosed with PBC based on the following three clinical criteria: (1) the presence of detectable AMA in the serum; (2) elevated liver enzymes, including alkaline phosphatase, at the initial diagnosis; and (3) compatible histological features according to Scheuer’s classification. Patients who had acute hepatitis, a chronic hepatitis virus B or C infection, alcoholic liver disease, and other chronic liver diseases were excluded from this study. The demographics and clinical data of the patients at the end of the observation period are shown in Table 1. The sex distribution and age of the healthy controls were as follows: female 310 (83.6%), median age 44 years, range 25–84 years. The study protocol was approved by the Committee for Ethical Issues dealing with the Human Genome and Gene Analysis at the Clinical Research Center in the National Hospital Organization (NHO) Nagasaki Medical Center and Shinshu University School of Medicine, and written informed consent was obtained from each subject.
Classification of clinical stages of PBC
PBC patients were classified into the following three different clinical stages based on the liver biopsy and/or clinical manifestations: clinical stage I, Scheuer’s stage 1 or 2 in the liver biopsy or unknown histological stage without any signs indicating portal hypertension or liver cirrhosis; clinical stage II, Scheuer’s stage 3 or 4 in the liver biopsy or any histological stage with signs of portal hypertension or liver cirrhosis but without persistent jaundice (total bilirubin <2 mg/dL); and clinical stage III, any Scheuer’s stage with persistent or progressive jaundice (total bilirubin ≥2 mg/dL).
Clinical stage I was defined as early-stage disease, whereas clinical stages II and III were defined as late-stage disease. Clinical stages I and II were also defined as a non-jaundice stage, whereas clinical stage III was defined as a jaundice stage. The observation period was defined as the time frame from the initial diagnosis until death, liver transplantation, death from non-liver associated diseases, or the end of the follow-up period, whichever came first. The demographics of the early- and late-stage patients at the end of the observation period are shown in Table 2.
Detection of autoantibodies
AMA and anti-centromere antibodies were detected using commercially available enzyme-linked immunosorbent assay kits (MBL, Nagoya, Japan). Anti-gp210 antibodies were detected as previously described [28]. These autoantibodies were assayed at least twice during the observation period, using serum samples obtained at different time points.
DNA preparation and genotyping
Genomic DNA was extracted from the peripheral whole blood of subjects using a NucleoSpin Blood Quick Pure (Macherey-Nagel, Düeren, Germany) according to the manufacturer’s protocol.
CTLA4 and SLC4A2 SNPs were analyzed by polymerase chain reaction–restriction fragment length polymorphism (PCR–RFLP) and TaqMan SNP Genotyping assays as previously described [6, 10]. All primers and probes for the TaqMan SNP Genotyping assays were purchased from Applied Biosystems (Foster City, CA, USA). The PCR primers and restriction enzymes for PCR–RFLP are shown in Supplementary Table 1 and were purchased from Sigma-Aldrich (St. Louis, MO, USA) and New England BioLabs (Ipswich, MA, USA), respectively.
Selection of SNPs and haplotypes
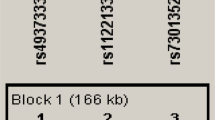
Only one tag SNP, CTLA4 rs231777 SNP, was selected based on the linkage disequilibrium and haplotype blocks of all the SNPs (>5% minor allele frequency) in CTLA4 chromosomal region 2q 33 containing the 2-kb up-stream region on the HapMap Japanese in Tokyo (JPT) data (http://www.hapmap.org) using the default setting of the iHap website. Other CTLA4 SNPs (>5% minor allele frequency), rs231775, rs3087243, and rs231725, which were reportedly associated with CTLA4 function, were also chosen. Four SLC4A2 tag SNPs (rs2069443, rs2303933, rs2303937, and rs2303941) were selected based on linkage disequilibrium and haplotype blocks from all SNPs (>5% minor allele frequency) in SLC4A2 chromosomal region 7q 35–36 containing the 5-kb up- and down-stream regions on the HapMap JPT data using the default setting of the Haploview 4.1 software program (Broad Institute, Cambridge, MA, USA).
Statistical analysis
The clinical characteristics were compared between the early and late stage using an unpaired Student’s t test, Mann–Whitney U test, and Fisher’s exact test. Hardy–Weinberg equilibrium was evaluated based on the χ2 test for goodness of fit. The associations between SNPs and disease susceptibility and progression, as well as autoantibody production, were examined using the χ2 test. Multiple testing in the allele and haplotype analyses was corrected using Bonferroni’s correction and permutation test (1000 simulations), respectively. These analyses were conducted with Statcel2 and SNPAlyze ver.7.0 software (Dynacom, Yokohama, Japan). Statistical significance was defined as P < 0.05.
Results
CTLA4 SNPs were significantly associated with PBC susceptibility in Japanese patients
First, we performed Hardy–Weinberg equilibrium tests to determine whether the CTLA4 and SLC4A2 SNPs genotyped in this study were associated with homogeneous genetic backgrounds. All CTLA4 and SLC4A2 SNPs were in Hardy–Weinberg equilibrium (Supplementary Table 2).
Subsequently, we analyzed the association between CTLA4 and SLC4A2 SNPs and PBC susceptibility. The frequencies of major alleles G, G, and A at CTLA4 rs231775, rs3087243, and rs231725 SNPs, respectively, were significantly increased in PBC patients compared to controls in cohort 1, cohort 2, and the combined cohort (Table 3). The frequency of the G allele at the SLC4A2 rs2303937 SNP was significantly decreased in PBC patients compared to controls in cohort 1, but not in cohort 2 or the combined cohort (Table 3).
CTLA4 SNPs were significantly associated with progression to late-stage disease
To determine the associations between the CTLA4 and SLC4A2 SNPs and PBC progression, we compared the frequencies of these SNPs between the early and late stages.
Although gender was not significantly different between early- and late-stage disease, PBC patients in the early stage tended to be significantly younger and have a shorter observation period than late-stage patients (Table 2). These results imply that a few patients in the early stage might progress to late-stage disease in the future.
The frequency of the A allele at the CTLA4 rs231725 SNP was significantly decreased in PBC patients with late-stage disease compared to those with early-stage disease in both cohort 1 and cohort 2 (Table 4). The significance of this SNP for progression to late-stage disease was markedly increased when cohort 1 and cohort 2 were combined, even after Bonferroni’s correction. The frequencies of G alleles at the CTLA4 rs231775 and rs3087243 SNPs were significantly decreased in late-stage patients compared to early-stage patients in the combined cohort; the significance disappeared after Bonferroni’s correction (Table 4).
On the other hand, there were no significant differences in the frequencies of all alleles at the SLC4A2 SNPs between early- and late-stage disease (Table 4). Furthermore, there were no significant differences in the frequencies of all tested CTLA4 and SLC4A2 alleles between patients in the non-jaundice stage and those in the jaundice stage (Supplementary Table 3).
CTLA4 and SLC4A2 SNPs were associated with anti-gp210 and anti-centromere antibody production, respectively
We next analyzed the associations between CTLA4 and SLC4A2 SNPs and the production of AMA and anti-gp210 and anti-centromere antibodies (Tables 5 and 6 and Supplementary Table 4). The frequency of the C allele at the CTLA4 rs231777 SNP was significantly decreased in anti-gp210 antibody-positive patients compared to anti-gp210 antibody-negative patients in cohort 1. Although this SNP was not significantly different between the two groups in cohort 2, this SNP was significantly different in the combined cohort, even after Bonferroni’s correction. Although the frequencies of the major alleles, the G allele at CTLA4 rs231775 SNP and the A allele at CTLA4 rs231725 SNP, were significantly decreased in anti-gp210 antibody-positive patients compared to anti-gp210 antibody-negative patients in the combined cohort, the significance disappeared after Bonferroni’s correction (Table 5).
The frequency of the G allele at the SLC4A2 rs2303937 SNP was significantly increased in anti-centromere antibody-positive patients compared to anti-centromere antibody-negative patients in the combined cohort, but the statistical significance disappeared after Bonferroni’s correction (Table 6).
On the other hand, there were no CTLA4 or SLC4A2 SNPs that were significantly associated with AMA production (Supplementary Table 4).
CTLA4 and SLC4A2 haplotypes were differentially associated with PBC development and progression to late-stage disease and anti-gp210 or anti-centromere antibody production
Haplotype analysis revealed that CTLA4 haplotype 1 (rs231775 G, rs231777 C, rs3087243 G, rs231725 A; GCGA) was significantly increased in PBC patients compared to controls, while CTLA4 haplotype 2 (ACAG) was significantly decreased in PBC patients compared to controls. Conversely, CTLA4 haplotype 1 and haplotype 2 were significantly decreased and increased, respectively, in PBC patients with late-stage disease compared to those with early-stage disease. In addition, CTLA4 haplotype 3 (ATGG) and haplotype 1 were significantly increased and decreased, respectively, in anti-gp210 antibody-positive patients compared to anti-gp210 antibody-negative patients (Table 7).
SLC4A2 haplotype 4 (rs2069443 A, rs2303933 G, rs2303937 A, rs2303941 T; AGAT) and haplotype 1 (AGGT) were significantly increased and decreased, respectively, in PBC patients compared to controls. Furthermore, SLC4A2 haplotype 3 (AAGC) was significantly increased in anti-centromere antibody-positive patients compared to anti-centromere antibody-negative patients (Table 8).
Discussion
A significant association between the CTLA4 rs231725 SNP and PBC susceptibility was first reported in the United States and was replicated in Canada by Juran et al. [7, 21]. A modest association between the CTLA4 rs231725 SNP and PBC susceptibility was also recently found in the combined Shinshu and Nagasaki cohort in the Japanese population [6]. The present study increased the number of controls and PBC patients in the Nagasaki cohort, and further confirmed that the CTLA4 rs231725 SNP is significantly associated with PBC susceptibility in the Japanese population. In addition, the CTLA4 rs3087243 and rs231775 SNPs were associated with PBC susceptibility in the present two different Japanese cohorts. These results are consistent with previous reports from the United Kingdom, China, Italy, France, and North America [4, 9, 11–13].
In the present haplotype analysis, CTLA4 haplotype 1 (rs231775 G, rs231777 C, rs3087243 G, rs231725 A; GCGA) was significantly associated with PBC susceptibility in the Japanese population, whereas CTLA4 haplotype 2 (ACAG) was associated with PBC resistance in Japanese patients. These results are consistent with the risk and protective haplotypes for PBC susceptibility previously reported from North America [12, 21]. A functional analysis of CTLA4 SNPs showed that the G allele at the CTLA4 rs231775 SNP resulted in a Thr-to-Ala amino acid substitution, leading to diminished CTLA4 expression on the cell surface [29]. Soluble CTLA4 mRNA is expressed at lower levels in healthy controls who have the G allele compared to those who have the A allele of the CTLA4 rs3087243 SNP [30]. CTLA4 SNP rs231725 might be associated with the expression of CTLA4 via the stability of its mRNA, since the CTLA4 rs231725 SNP is located at the 3′-flanking region of the CTLA4 gene. Thus, the functional alterations associated with these CTLA4 SNPs might similarly operate in PBC development in Japanese patients.
As for PBC progression, the CTLA4 rs231725 SNP was significantly associated with progression to late-stage disease. In addition, haplotype analyses revealed that CTLA4 haplotype 1 (rs231775 G, rs231777 C, rs3087243 G, rs231725 A; GCGA) was a risk factor for PBC susceptibility but was a protective factor for PBC progression. Conversely, CTLA4 haplotype 2 (ACAG) was a protective and risk factor, respectively, for PBC susceptibility and progression. Thus, the haplotype that confers PBC susceptibility confers resistance to PBC progression, and vice versa. These results might imply that PBC development and progression have different components of pathogenesis in terms of CTLA4 genetic polymorphisms. A previous report showed that a CTLA4 haplotype containing rs231775 G, rs231777 C, rs3087243 G, and rs231725 A was a risk factor for both susceptibility and progression to orthotopic liver transplantation (OLT) in Caucasian PBC patients [21]. However, there was no significant association between CTLA4 haplotypes and progression to hepatic failure and/or OLT in Japanese patients in the present study. Since the number of patients who progressed to hepatic failure and/or OLT was only 10% of the patients with late-stage disease in our cohort, further study is needed to dissect the association between CTLA4 SNPs and severe PBC progression.
SLC4A2-deficient mice exhibit PBC-like features characterized by portal inflammation with CD4+ and CD8+ T-lymphocyte infiltration, elevated alkaline phosphatase and alanine aminotransferase levels, and prevalence of AMA, indicating that functional alterations in SLC4A2 are involved in PBC pathogenesis in humans [31]. Indeed, genetic SLC4A2 polymorphisms were associated with AMA production and PBC progression in Caucasian PBC patients [11, 20]. In the present study, although SLC4A2 SNPs and haplotypes were not significantly associated with PBC progression, SLC4A2 haplotype 1 (rs2069443 A, rs2303933 G, rs2303937 G, rs2303941 T; AGGT) and haplotype 4 (AGAT) were significantly associated with PBC susceptibility. Further studies are required to confirm the associations between SLC4A2 SNPs and haplotypes and PBC susceptibility and progression among various ethnicities.
In cohort studies in the United States, the CTLA4 rs231775 G/G genotype and rs231725 A/A genotype tended to be more prevalent in AMA-positive PBC patients compared to AMA-negative PBC patients [8, 21]. Furthermore, a CTLA4 SNP haplotype was associated with AMA production [21]. In addition, the SLC4A2 rs2303929 and rs3793336 SNPs were associated with AMA production in Caucasian PBC patients [20]. These results indicate that genetic polymorphisms in both CTLA4 and SLCA42 are involved in autoantibody production in PBC patients. Although the CTLA4 and SLC4A2 SNPs were not significantly associated with AMA production in the present study in Japanese PBC patients, we found, for the first time, that the CTLA4 rs231777 and SLC4A2 rs2303937 SNPs were associated with anti-gp210 and anti-centromere antibody production, respectively. There were also significant associations between haplotypes carrying these risk alleles and anti-gp210 or anti-centromere antibody production. Moreover, the association of these SNPs with autoantibody production was still significant, even after a multivariate analysis, by taking into account the HLA-DRB1 polymorphisms in which HLA-DRB1*0405 and *0803 were significantly associated with anti-gp210 and anti-centromere antibody production, respectively (data not shown) [3].
Aberrant self-antigen expression and presentation during apoptosis are thought to be one mechanism that contributes to the breakdown of immunological tolerance. In fact, abnormal expression of pyruvate dehydrogenase E2 (PDC-E2), which is a major target antigen for AMA, was observed in the apical region of the biliary epithelium in PBC patients [32]. Apoptotic blebs containing intact PDC-E2 were found in biliary epithelial cells during apoptosis [33]. Aberrant gp210 expression was observed in biliary epithelial cells in the small bile ducts of PBC patients, and the degree of gp210 expression was positively correlated with PBC disease activity [34]. Therefore, it is possible that CTLA4 SNPs play an important role in the breakdown of immunological tolerance to the gp210 antigen that is aberrantly presented, although the localization of the gp210 antigen during apoptosis remains to be determined. On the other hand, SLC4A2 participates in lymphocyte activation by regulating intracellular pH homeostasis [35]. The characteristic features of PBC, including AMA production, were observed in SLC4A2-deficient mice. The expression of genes related to antigen presentation was also increased in cholangiocytes from SLC4A2-deficient mice [31]. Thus, alterations in these SLC4A2 functions, which are possibly associated with genetic polymorphisms in SLC4A2, might be involved in anti-centromere antibody production.
In conclusion, we confirmed that CTLA4 SNPs are associated with PBC susceptibility and progression in the Japanese population. Furthermore, we showed, for the first time, that CTLA4 and SLC4A2 SNPs are associated with anti-gp210 and anti-centromere antibody production, respectively. Since anti-gp210 and anti-centromere antibodies are different risk factors for the hepatic failure-type and portal hypertension-type of PBC progression, the results in the present study may imply that genetic CTLA4 and SLC4A2 polymorphisms are differentially involved in multiple steps of PBC pathogenesis.
References
Selmi C, Mayo MJ, Bach N, Ishibashi H, Invernizzi P, Gish RG, et al. Primary biliary cirrhosis in monozygotic and dizygotic twins: genetics, epigenetics, and environment. Gastroenterology. 2004;127:485–92.
Donaldson PT, Baragiotta A, Heneghan MA, Floreani A, Venturi C, Underhill JA, et al. HLA class II alleles, genotypes, haplotypes, and amino acids in primary biliary cirrhosis: a large-scale study. Hepatology. 2006;44:667–74.
Nakamura M, Yasunami M, Kondo H, Horie H, Aiba Y, Komori A, et al. Analysis of HLA-DRB1 polymorphisms in Japanese patients with primary biliary cirrhosis (PBC): the HLA-DRB1polymorphism determines the relative risk of antinuclear antibodies for disease progression in PBC. Hepatol Res. 2010;40:494–504.
Fan LY, Tu XQ, Cheng QB, Zhu Y, Feltens R, Pfeiffer T, et al. Cytotoxic T lymphocyte associated antigen-4 gene polymorphisms confer susceptibility to primary biliary cirrhosis and autoimmune hepatitis in Chinese population. World J Gastroenterol. 2004;10:3056–9.
Invernizzi P, Selmi C, Poli F, Frison S, Floreani A, Alvaro D, et al. Human leukocyte antigen polymorphisms in Italian primary biliary cirrhosis: a multicenter study of 664 patients and 1992 healthy controls. Hepatology. 2008;48:1906–12.
Joshita S, Umemura T, Yoshizawa K, Katsuyama Y, Tanaka E, Nakamura M, et al. Association analysis of cytotoxic T-lymphocyte antigen 4 gene polymorphisms with primary biliary cirrhosis in Japanese patients. J Hepatol. 2010;53:537–41.
Juran BD, Atkinson EJ, Larson JJ, Schlicht EM, Liu X, Heathcote EJ, et al. Carriage of a tumor necrosis factor polymorphism amplifies the cytotoxic T-lymphocyte antigen 4 attributed risk of primary biliary cirrhosis: evidence for a gene–gene interaction. Hepatology. 2010;52:223–9.
Juran BD, Atkinson EJ, Schlicht EM, Fridley BL, Petersen GM, Lazaridis KN. Interacting alleles of the coinhibitory immunoreceptor genes cytotoxic T-lymphocyte antigen 4 and programmed cell-death 1 influence risk and features of primary biliary cirrhosis. Hepatology. 2008;47:563–70.
Oertelt S, Kenny TP, Selmi C, Invernizzi P, Podda M, Gershwin ME. SNP analysis of genes implicated in T cell proliferation in primary biliary cirrhosis. Clin Dev Immunol. 2005;12:259–63.
Ohishi Y, Nakamura M, Iio N, Higa S, Inayoshi M, Aiba Y, et al. Single-nucleotide polymorphism analysis of the multidrug resistance protein 3 gene for the detection of clinical progression in Japanese patients with primary biliary cirrhosis. Hepatology. 2008;48:853–62.
Poupon R, Ping C, Chretien Y, Corpechot C, Chazouilleres O, Simon T, et al. Genetic factors of susceptibility and of severity in primary biliary cirrhosis. J Hepatol. 2008;49:1038–45.
Walker EJ, Hirschfield GM, Xu C, Lu Y, Liu X, Coltescu C, et al. CTLA4/ICOS gene variants and haplotypes are associated with rheumatoid arthritis and primary biliary cirrhosis in the Canadian population. Arthritis Rheum. 2009;60:931–7.
Agarwal K, Jones DE, Daly AK, James OF, Vaidya B, Pearce S, et al. CTLA-4 gene polymorphism confers susceptibility to primary biliary cirrhosis. J Hepatol. 2000;32:538–41.
Hirschfield GM, Liu X, Xu C, Lu Y, Xie G, Gu X, et al. Primary biliary cirrhosis associated with HLA, IL12A, and IL12RB2 variants. N Engl J Med. 2009;360:2544–55.
Hirschfield GM, Liu X, Han Y, Gorlov IP, Lu Y, Xu C, et al. Variants at IRF5-TNPO3, 17q12-21 and MMEL1 are associated with primary biliary cirrhosis. Nat Genet. 2010;42:655–7.
Liu X, Invernizzi P, Lu Y, Kosoy R, Bianchi I, Podda M, et al. Genome-wide meta-analyses identify three loci associated with primary biliary cirrhosis. Nat Genet. 2010;42:658–60.
Zenewicz LA, Abraham C, Flavell RA, Cho JH. Unraveling the genetics of autoimmunity. Cell. 2010;140:791–7.
Gregersen PK, Behrens TW. Genetics of autoimmune diseases—disorders of immune homeostasis. Nat Rev Genet. 2006;7:917–28.
Invernizzi P, Gershwin ME. The genetic basis of primary biliary cirrhosis: premises, not promises. Gastroenterology. 2008;135:1044–7.
Juran BD, Atkinson EJ, Larson JJ, Schlicht EM, Lazaridis KN. Common genetic variation and haplotypes of the anion exchanger SLC4A2 in primary biliary cirrhosis. Am J Gastroenterol. 2009;104:1406–11.
Juran BD, Atkinson EJ, Schlicht EM, Fridley BL, Lazaridis KN. Primary biliary cirrhosis is associated with a genetic variant in the 3′ flanking region of the CTLA4 gene. Gastroenterology. 2008;135:1200–6.
Medina JF, Lecanda J, Acin A, Ciesielczyk P, Prieto J. Tissue-specific N-terminal isoforms from overlapping alternate promoters of the human AE2 anion exchanger gene. Biochem Biophys Res Commun. 2000;267:228–35.
Alper SL. Molecular physiology and genetics of Na+-independent SLC4 anion exchangers. J Exp Biol. 2009;212:1672–83.
Medina JF, Martinez A, Vazquez JJ, Prieto J. Decreased anion exchanger 2 immunoreactivity in the liver of patients with primary biliary cirrhosis. Hepatology. 1997;25:12–7.
Prieto J, Qian C, Garcia N, Diez J, Medina JF. Abnormal expression of anion exchanger genes in primary biliary cirrhosis. Gastroenterology. 1993;105:572–8.
Melero S, Spirli C, Zsembery A, Medina JF, Joplin RE, Duner E, et al. Defective regulation of cholangiocyte Cl−/HCO3(−) and Na+/H+ exchanger activities in primary biliary cirrhosis. Hepatology. 2002;35:1513–21.
Nakamura M, Kondo H, Mori T, Komori A, Matsuyama M, Ito M, et al. Anti-gp210 and anti-centromere antibodies are different risk factors for the progression of primary biliary cirrhosis. Hepatology. 2007;45:118–27.
Nakamura M, Shimizu-Yoshida Y, Takii Y, Komori A, Yokoyama T, Ueki T, et al. Antibody titer to gp210-C terminal peptide as a clinical parameter for monitoring primary biliary cirrhosis. J Hepatol. 2005;42:386–92.
Anjos S, Nguyen A, Ounissi-Benkalha H, Tessier MC, Polychronakos C. A common autoimmunity predisposing signal peptide variant of the cytotoxic T-lymphocyte antigen 4 results in inefficient glycosylation of the susceptibility allele. J Biol Chem. 2002;277:46478–86.
Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, et al. Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature. 2003;423:506–11.
Salas JT, Banales JM, Sarvide S, Recalde S, Ferrer A, Uriarte I, et al. Ae2a,b-deficient mice develop antimitochondrial antibodies and other features resembling primary biliary cirrhosis. Gastroenterology. 2008;134:1482–93.
Tsuneyama K, Van de Water J, Leung PS, Cha S, Nakanuma Y, Kaplan M, et al. Abnormal expression of the E2 component of the pyruvate dehydrogenase complex on the luminal surface of biliary epithelium occurs before major histocompatibility complex class II and BB1/B7 expression. Hepatology. 1995;21:1031–7.
Lleo A, Selmi C, Invernizzi P, Podda M, Coppel RL, Mackay IR, et al. Apotopes and the biliary specificity of primary biliary cirrhosis. Hepatology. 2009;49:871–9.
Nakamura M, Takii Y, Ito M, Komori A, Yokoyama T, Shimizu-Yoshida Y, et al. Increased expression of nuclear envelope gp210 antigen in small bile ducts in primary biliary cirrhosis. J Autoimmun. 2006;26:138–45.
Lardner A. The effects of extracellular pH on immune function. J Leukoc Biol. 2001;69:522–30.
Acknowledgments
This study was supported by a grant to Minoru Nakamura from Health and Labour Sciences Research Grants for Research on Measures for Intractable Disease from the Ministry of Health, Labour and Welfare of Japan. The authors thank Drs. Akira Saito, Eiichi Takesaki, Tsutomu Yamashita, Masakazu Kobayashi, Hideo Nishimura, Haruhiro Yamashita, Hirotaka Kouno, Koichi Honda, Akinori Shirahige, Takeaki Sato, Keisuke Ario, Masahiko Takahashi, Tetsuo Yamamoto, Noboru Hirashima, Yukio Ohara, Hiroshi Mano, Michio Kato, Eiji Mita, Hironori Sakai, Satoru Tsuruta, Keiichi Hirata, and Jinya Ishida at NHOSLJ for providing serum samples and clinical information from patients with PBC; thanks to Drs. Seigo Abiru, Shinya Nagaoka, and Koji Yano at NHO Nagasaki Medical Center for patients’ care and technical assistance.
Conflict of interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
NHOSLJ: National Hospital Organization Study Group for Liver Disease in Japan.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Aiba, Y., Nakamura, M., Joshita, S. et al. Genetic polymorphisms in CTLA4 and SLC4A2 are differentially associated with the pathogenesis of primary biliary cirrhosis in Japanese patients. J Gastroenterol 46, 1203–1212 (2011). https://doi.org/10.1007/s00535-011-0417-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-011-0417-7