
Abstract
Background/purpose
The accurate preoperative evaluation of liver fibrosis stage is important in determining surgical procedures. Although percutaneous liver biopsy is the gold standard, it may cause undesirable complications, such as bleeding. This study aimed to evaluate the usefulness of real-time tissue elastography for the preoperative assessment of liver fibrosis stage.
Methods
We focused on a new mode of sonogram, real-time elastography, which can show tissue elasticity on images, and express the elasticity numerically. The elastic ratio of the liver for the intercostal muscle for each patient was calculated preoperatively, using the sonography device. The liver fibrosis stages were finally determined in the operative specimens from 41 patients. We examined the correlation between the elastic ratio and the histological fibrosis stage.
Results
The lower the elastic ratio, the more advanced was the liver fibrosis stage. There was a significant correlation between the elastic ratio and the histological fibrosis stage. The area under the receiver-operating characteristics curve for the diagnosis of significant liver fibrosis using this device was superior to those conventionally determined by blood parameters.
Conclusions
Real-time elastography is a promising sonography-based noninvasive method for the preoperative assessment of liver fibrosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Chronic infection with viral hepatitis is an important cause of liver cirrhosis and its sequelae [1–3]. A precise assessment of the degree of liver fibrosis is important for the estimation of prognosis, for surveillance, and for treatment decisions in patients with chronic viral hepatitis [4]. Moreover, as it is reported that the risk of liver failure is highest in patients with cirrhosis undergoing major hepatectomy [5–7], it is very important to assess preoperatively the liver fibrosis stage to prevent postoperative mortality. Currently, liver biopsy is the gold-standard method for assessing liver fibrosis [8, 9]. However, it is difficult to perform liver biopsy for all patients who need to be assessed repeatedly because of its invasiveness and potential risk. Moreover, its accuracy in assessing liver fibrosis is sometimes questionable, as reproducibility is poor due to sampling errors and, even in adequately sized specimens, diagnostic opinions often differ among pathologists. Therefore, many studies have focused on the evaluation of noninvasive methods for the assessment of liver fibrosis stage.
Real-time tissue elastography is a new method for the measurement of tissue elasticity, using a sonography machine (EUB-8500; Hitachi Medical Systems, Tokyo, Japan) [10, 11]. With this device, the echo signals are captured in real time while the probe slightly compresses or relaxes the body through freehand operation. The small compression plate is usually attached to an ultrasonic probe so that stable tissue compression is attained and the stress field is transmitted more uniformly; consequently, a good strain image is obtained. The strain of tissue is color-coded according to its magnitude and translucently superimposed on the conventional two-dimensional (2D) images. This simultaneous display enables us to understand the anatomical correspondence between the tissue elasticity image and the conventional B-mode image. On the color scale strain image, red indicates that tissue is soft and blue that it is hard. This device can rapidly calculate the relative hardness of tissue, and display this information as real-time color images [10, 11]. Friedrich-Rust et al. [12] examined the usefulness of this device in the evaluation of liver fibrosis, using data from 79 patients with chronic viral hepatitis of known fibrosis stage and 20 healthy volunteers. In the present study, we used operative liver specimens from 41 patients to finally determine the true liver fibrosis stage for each patient and investigated whether this new noninvasive diagnostic method is superior to other conventional ones using blood parameters in assessing the degree of liver fibrosis preoperatively.
Patients and methods
Patients
Between August 2005 and August 2008, 41 patients who underwent an intraoperative liver biopsy or a hepatectomy at Tokushima University Hospital were included in this study. Among these patients, 32 patients underwent a hepatectomy (11, hepatocellular carcinoma; 9, metastatic liver cancer; 7, cholangiocellular carcinoma; 5, others). In 7 patients, an intraoperative liver biopsy was obtained when a splenectomy was performed to alleviate hypersplenism due to liver cirrhosis. The other 2 patients underwent living-donor liver transplantation for hepatocellular carcinoma (HCC) and liver cirrhosis. The patients’ characteristics are summarized in Table 1. The present study was performed in accordance with the ethical guidelines of the Declaration of Helsinki.
Liver histology and determination of liver fibrosis stage
The liver specimens were fixed in formalin, embedded in paraffin, and stained with hematoxylin and eosin. The new Inuyama scoring system for chronic hepatitis proposed by the Japanese Liver Study Group in 1994 [13], which is similar to the classification of chronic hepatitis determined by the USA-European Liver Study Group [14], was used to assess the fibrosis stage, as follows; score 0, no fibrosis (F0); score 1, fibrous portal expansion (F1); score 2, bridging fibrosis (F2); score 3, bridging fibrosis with lobular degeneration (F3); and score 4, cirrhosis (F4).
Elastic ratio
Hepatic elasticity was measured using real-time tissue elastography (EUB-8500; Hitachi Medical Systems). The patients were examined in a supine position with their right arm elevated above their head. After examination in B-mode, the mode was switched to elastography, and the probe scanned vertically from the right intercostal space to observe the right hepatic lobe. In the evaluation of liver fibrosis, we calculated the elastic ratio of the liver for the intercostal muscle (Fig. 1). A higher elastic ratio indicates softer hepatic elasticity. None of the patients had liver tumors in the right lobe that might have interfered with the real-time elastography.

The elastic ratio was measured between the tissue compressibility of the intercostal muscle (A) and that of the liver (B). Red indicates that tissue is soft and blue that it is hard
Blood parameters
The following parameters were determined using blood samples: aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, platelets, hyaluronic acid (HA), type IV collagen, cholinesterase, indocyanine green retention rate at 15 min (ICG-R15), and the aspartate aminotransferase-to-platelet ratio index (APRI). The APRI index was calculated as follows: AST (per upper limit of normal; 33 IU/l) × 100/platelet count (109/l) [14].
Statistical analysis
All results were expressed as mean values ± SD. Comparisons among fibrosis stage groups were performed by the Kruskal–Wallis one-way analysis of variance (ANOVA) test. Correlations between each parameter and the histological fibrosis stage were also assessed using Spearman’s test. A P value of less than 0.05 was considered statistically significant.
The diagnostic performance of the elastic ratio, HA, type IV collagen, and APRI were assessed by receiver-operating characteristic (ROC) curves. An area under the curve of 1.0 is characteristic of an ideal test, whereas 0.5 indicates a test is of no diagnostic value. The diagnosis of significant fibrosis (F ≥ F3) was selected as the optimal liver stiffness cut off.
The statistical analyses were done using Stat View software (Abacus Concepts, Berkeley, CA, USA).
Results
Relationship between liver elastic ratio and liver fibrosis
The median liver elastic ratios in patients with F0 (n = 9), F1 (n = 6), F2 (n = 4), F3 (n = 7), and F4 (n = 15) were 1.56, 1.36, 1.03, 0.62, and 0.45, respectively. Figure 2a shows box plots of the elastic ratio for each fibrosis stage. There was a significant correlation between the fibrosis stage and the elastic ratio (Spearman’s test, P < 0.0001).

Box plots of a elastic ratio, b hyaluronic acid, c type IV collagen, and d aspartate aminotransferase-to-platelet ratio index (APRI) for each fibrosis stage. Top and bottom of boxes represent first and third quartiles, respectively. The length of the box represents interquartile range within which 50% of values are located. The thick line through each box represents the median. Error bars mark the minimum and maximum values (ranges). A significant correlation was found between liver fibrosis stage and elastic ratio (Spearman’s test, P < 0.0001), or hyaluronic acid (Spearman’s correlation coefficient, P < 0.001), or type IV collagen (Spearman’s test, P < 0.0008) or APRI (Spearman’s test, P < 0.0001)
Relationship between liver elastic ratio and blood parameters
Figure 2b–d shows box plots of HA level, type IV collagen level, and APRI in patients with various fibrosis stages. The median HA levels in patients with F0, F1, F2, F3, and F4 were 72.4, 82.7, 169.0, 134.1, and 306.3 ng/ml, respectively (Fig. 2b). There was a significant correlation between fibrosis stage and HA level (Spearman’s test; P < 0.001).
The median type IV collagen levels in patients with F0, F1, F2, F3, and F4 were 135.2, 222.8, 232.5, 173.4, and 289.0 ng/ml, respectively (Fig. 2c). There was a significant correlation between fibrosis stage and type IV collagen level (Spearman’s test, P = 0.0008).
The median APRI levels in patients with F0, F1, F2, F3, and F4 were 0.39, 0.53, 0.56, 0.88, and 1.76, respectively (Fig. 2d). There was a significant correlation between fibrosis stage and APRI (Spearman’s test; P < 0.0001).
Comparison of elastic ratio by real-time tissue elastography with HA and APRI
Figure 3 shows ROC curves for the diagnosis of fibrosis stages (F ≥ F3). The areas under the ROC curves, by elastic ratio, HA, type IV collagen, and APRI were 0.951, 0.822, 0.707, and 0.835, respectively. The area under the ROC curve by elastic ratio was superior to those stratified by other serum parameters.

Receiver-operating characteristic curves for diagnosis of liver fibrosis (F ≥ F3) by real-time elastography, hyaluronic acid, type IV collagen, and APRI. The area under the receiver-operating characteristic curve for the diagnosis of significant liver fibrosis or cirrhosis (F ≥ F3) using the EUB-8500 (Hitachi Medical Systems) device was superior to those for the blood parameters
With regard to the distribution of elastic ratio in relation to fibrosis stage, the cut off values were determined to be 1.18 for F ≥ F2, 0.75 for F ≥ F3, and 0.6 for F = F4 (Table 2). The sensitivity and specificity for the detection of significant fibrosis (F ≥ F3) were 95.5 and 89.4%, respectively. The positive predictive value and the negative predictive value were 91.3 and 94.4%, respectively.
Discussion
In patients with chronic viral hepatitis, the identification of significant fibrosis (F ≥ F3) is of special interest, because the presence of fibrosis is an important parameter for indications for antiviral treatment [12]. Evaluation of histopathological tissue obtained by liver biopsy has been the conventional gold standard for the evaluation of liver fibrosis [13, 15]. However, patients sometimes hesitate about undergoing a liver biopsy because of the pain associated with the procedure, the time it requires, and the economic burden. As a result, biopsy evaluation may be omitted and hematological data used instead. Because evaluation by hematological data has its limits, however, a noninvasive imaging diagnosis of liver fibrosis is warranted.
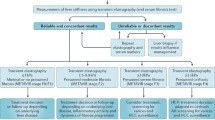
Transient elastography was recently developed for the noninvasive evaluation of liver elasticity, and its usefulness has been reported [15–17]. This technique involves the generation, by a probe, of audible external vibrations propagating through the liver. However, there are technical limitations that may prevent measurement in patients with a high level of obesity, or patients with severe hepatic atrophy. In the previous studies, it was difficult to evaluate liver elasticity in patients with ascites. However, real-time elastography enables us to evaluate liver elasticity even in patients with these unfavorable conditions, and it is easy to verify the position because the images are juxtaposed with B-mode reference images.
We found an excellent correlation between the elastic ratio obtained with real-time elastography and the liver fibrosis stage. Moreover, we assessed the performance of surrogate blood parameters of fibrosis, such as the HA level and APRI. These markers are known to be useful for the quantitative evaluation of liver fibrosis [18, 19]. Castera et al. [15] have reported that transient elastography is a simple and effective method for assessing liver fibrosis, with similar performance to APRI. Takeda et al. [20] reported that liver stiffness values were significantly correlated with the serum HA level and concentration of type IV collagen. In the present study, our data also showed highly significant correlations between liver fibrosis stage and fibrosis markers, such as HA, type IV collagen, and APRI.
ROC curves are an efficient way to display the relationship between sensitivity and specificity for a test with continuous variables. The ROC curves in the present study showed the superiority of the elastic ratio using real-time elastography to other conventional blood parameters such as HA and APRI in diagnosing liver fibrosis stage.
Our result showed that real-time elastography is a useful method to evaluate liver elasticity. In addition, the combination of real-time elastography with blood tests may further improve sensitivity and specificity for the noninvasive estimation of liver fibrosis.
References
El-Serag HB. Hepatocellular carcinoma and hepatitis C in the United States. Hepatology. 2002;36:74–83.
Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med. 2001;345:41–52.
Seeff LB. Natural history of chronic hepatitis C. Hepatology. 2002;36:35–46.
Seeff LB, Hoofnagle JH. National Institutes of Health Consensus Development Conference: management of hepatitis C: 2002. Hepatology. 2002;36:S1–2.
Nagashima I, Takada T, Okinaga K, Nagawa H. A scoring system for the assessment of the risk of mortality after partial hepatectomy in patients with chronic liver dysfunction. J Hepatobiliary Pancreat Surg. 2005;12:44–8.
Belghiti J, Ogata S. Assessment of hepatic reserve for the indication of hepatic resection. J Hepatobiliary Pancreat Surg. 2005;12:1–3.
Poon RT, Fan ST. Assessment of hepatic reserve for indication of hepatic resection: how I do it. J Hepatobiliary Pancreat Surg. 2005;12:31–7.
Dienstag JL. The role of liver biopsy in chronic hepatitis C. Hepatology. 2002;36:S152–60.
Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med. 2001;344:495–500.
Shiina T. Real time tissue elasticity imaging by the compound autocorrelation method. J Med Ultrason. 1999;26:57–66.
Murayama N. Development of real-time tissue elastography in EUB-8500. J Med Ultrason 2004;31:113.
Friedrich-Rust M, Ong MF, Herrmann E, Dries V, Samaras P, Zeuzem S, et al. Real-time elastography for noninvasive assessment of liver fibrosis in chronic viral hepatitis. Am J Roentgenol. 2007;188:758–64.
Ichida F, Omata M, Tsuji T, Ichida T, Inoue K, Uemura A. New Inuyama classification: new criteria for histological assessment of chronic hepatitis. Hepatol Commun. 1996;6:112–9.
Castéra L, Vergniol J, Foucher J, Le Bail B, Chanteloup E, Haaser M, et al. Prospective comparison of transient elastography, fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology. 2005;128:343–50.
Desmet VJ, Gerber M, Hoofnagle JH, Manns M, Scheuer PJ. Classification of chronic hepatitis: diagnosis, grading and staging. Hepatology. 1994;19:1513–20.
Harada N, Soejima Y, Taketomi A, Yoshizumi T, Ikegami T, Yamashita Y, et al. Assessment of graft fibrosis by transient elastography in patients with recurrent hepatitis C after living donor liver transplantation. Transplantation. 2007;85:69–74.
Fraquelli M, Rigamonti C. Diagnosis of cirrhosis by transient elastography: what is hidden behind misleading results. Hepatology. 2007;282:282–3.
Pereira TN, Lewindon PJ, Smith JL, Murphy TL, Lincoln DJ, Shepherd RW, et al. Serum markers of hepatic fibrogenesis in cystic fibrosis liver disease. J Hepatol. 2004;41:576–83.
Guéchot J, Laudat A, Loria A, Serfaty L, Poupon R, Giboudeau J. Diagnostic accuracy of hyaluronan and type III procollagen amino-terminal peptide serum assays as markers of liver fibrosis in chronic viral hepatitis C evaluated by ROC curve analysis. Clin Chem. 1996;42:558–63.
Takeda T, Yasuda T, Nakayama Y, Nakaya M, Kimura M, Yamashita M, et al. Usefulness of noninvasive transient elastography for assessment of liver fibrosis stage in chronic hepatitis C. World J Gastroenterol. 2006;12:7768–73.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Kanamoto, M., Shimada, M., Ikegami, T. et al. Real time elastography for noninvasive diagnosis of liver fibrosis. J Hepatobiliary Pancreat Surg 16, 463–467 (2009). https://doi.org/10.1007/s00534-009-0075-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00534-009-0075-9