
Abstract
Efficient computation of quality of service (QoS) during medical data processing through intelligent measurement methods is one of the mandatory requirements of the medial healthcare world. However, emergency medical services often involve transmission of critical data, thus having stringent requirements for network quality of service (QoS). This paper contributes in three distinct ways. First, it proposes the novel adaptive QoS computation algorithm (AQCA) for fair and efficient monitoring of the performance indicators, i.e., transmission power, duty cycle and route selection during medical data processing in healthcare applications. Second, framework of QoS computation in medical applications is proposed at physical, medium access control (MAC) and network layers. Third, QoS computation mechanism with proposed AQCA and quality of experience (QoE) is developed. Besides, proper examination of QoS computation for medical healthcare application is evaluated with 4–10 inches large-screen user terminal (UT) devices (for example, LCD panel size, resolution, etc.). These devices are based on high visualization, battery lifetime and power optimization for ECG service in emergency condition. These UT devices are used to achieve highest level of satisfaction in terms, i.e., less power drain, extended battery lifetime and optimal route selection. QoS parameters with estimation of QoE perception identify the degree of influence of each QoS parameters on the medical data processing is analyzed. The experimental results indicate that QoS is computed at physical, MAC and network layers with transmission power (− 15 dBm), delay (100 ms), jitter (40 ms), throughput (200 Bytes), duty cycle (10%) and route selection (optimal). Thus it can be said that proposed AQCA is the potential candidate for QoS computation than Baseline for medical healthcare applications.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In the current era of healthcare domain, there are emerging trends and practices to monitor and manage the patients with all facilities in short span of time. At the same time, quality of service (QoS) computation is one of the important ingredients of medical networks. In parallel with QoS quality of experience (QoE), i.e., user’s perception plays the vital role to examine the overall performance of biomedical applications during healthcare data processing. The emergency medical centers at medical hospitals promote health assessment, physical checkup, counseling, curative treatment and health education services to the elderly patients. For instance, elderly diabetic patients are monitored by a glucometer device at their homes. Glucometer is connected to an auto inject insulin pump; then, that portable meter is wirelessly connected to the smart phone and pumps to regulate delivery of rapid or short-acting insulin up to 24 h through a catheter positioned under the skin of the patient. This whole process can be watched and easily handled by physician and medical staff through clear and big images or video clips in smart phones. So, the requirement for pleasurable consumption of medical media content for elderly healthcare lies at the heart of this paper. The medical media is the video, text, audio, etc., but this research mainly considers the visual domain. Technological revolution in portable devices has widely encouraged their use in every corner of the industry and academia. So, media streaming is done over 5G networks through portable devices with large screen for big and better picture of the scene. Dimitrov [2] surveyed in detail that around 82% user’s rejection toward any service or product is due to bad and unsatisfactory performance according to the aspects. Thus, the more appropriate way is to integrate both network’s features, i.e., QoS and customer’s perception, i.e., QoE than to monitor and compute the overall performance of the healthcare applications during medical data processing in an efficient and adaptive manner. In the meantime due to increase in performance and decrease in price of miniaturized devices, multimedia is everywhere. Nearly most of the handheld devices have the potential to tackle, compute and manage the medical data processing. With the proliferation of sensor-based miniaturized devices and digital technologies, there is a quite huge and rapid advancement in the medical healthcare market with high quality of service and better user perception [1]. The medical media streaming service is considered as a critical topic of user-perceived quality of experience (QoE) guaranteed service, e.g., if a doctor examines the patients’ health status by observing at the medical data processing, i.e., ECG for the prompt response, high bit rate is required than a blood pressure report of normal patients. The bandwidth allocation in the distribution network will be entirely different for both emergency and normal patients to get achieve/perceive same QoE level. QoE measures the user’s synthetic feelings about the user terminal (UT) device, network, system and applications. The best way to popularize medical media applications is to raise user’s satisfaction during operation.
For medical health services, QoE is a standard, reflecting the gap between existent service and user’s expectations. People are always harsh and prudent for health-related services, so if they feel uncomfortable, definitely will give up and distrust the service given by medical monitoring system. Before designing m-health monitoring system for patients, it is very vital to consider the key components for increasing QoE level. For modeling and evaluation of the user-perceived QoE of the medical media, ECG services over heterogeneous networks through distinct UT devices is one of the challenging task.
Usually, several performance indicators such as transmission power drain, delay, jitter and throughput at physical layer; duty cycle at MAC layer; and route selection at network layer defines the QoS of the healthcare system during medical data processing. On the contrary, perception of users that can be measured in terms of the mean opinion score (MOS) is known as the QoE, which has strong connection in assessing the overall quality of the network with innovative tools, current trends and practices. QoE is influenced by QoS parameters, which highly depend on network elements. Key factors are throughput, jitter, delay, etc. The impact of each individual or combined entities leads to blocking, blurriness or even blackouts with different levels of quality degradation of media streaming. With the growth of QoE interest, medical media providers are looking for the innovative QoE management and controlling techniques when the expectations of elderly patients are not fully fulfilled. Network providers evaluate the patient’s satisfaction level by using QoS parameters on the basis of some prior analyzed values; then, control/manage the QoE to deduce associated QoS parameters (throughput, delay, jitter, etc.). QoE heavily depends on the performance of the UT devices (i.e., cell phones and PDA’s) in terms of energy consumption and entropy. UT affects QoE in two critical ways. First, owing to the powerful processing and storage capabilities during operation, higher QoE is experienced with more powerful devices at same network-level QoS. Second, in order to capitalize on the merits, users with more powerful devices may require the network to provide higher QoS. For example, as compared to the standard definition TV, high definition (HD) TV demands more QoS and less data loss during signal transmission. Moreover, QoE encompasses additional ingredients which are affecting the patient’s perception of media presentation quality for instance, content analysis and categorization of digital media including bio-signal processing, audio retrieval, text retrieval, image retrieval, video analysis, etc. We summarize these areas under multimedia information retrieval and more frequently its understanding. It is realized that they share some important properties for example: first, they exploit digital signals, and second, signals are summarized by signal processing [1]. Bio-signals, digital audio, digital images, digital video, etc., are data sources that have been investigated in signal processing since many years. In short, multimedia information retrieval aims at the imitation of the sensual pattern recognition capabilities of the human being.
All multimedia information retrieval disciplines are based on digital media, i.e., one or multi-dimensional data streams of samples perceived through human-like senses (e.g., audio recording, text reading) or more or less sophisticated capturing mechanisms (e.g., ECG electrodes) [1]. Naturally or artificially, the media understanding process has to find solution for a number of fundamental interpretation and engineering problems. Most media types provide one-dimensional channels and for bio-signals, the dimension is a timeline. One of the difficult tasks is to match/correlate measurable QoS parameters with subjective quantity for instance QoE. While there are several other techniques to measure the subjective quantities for example, mean opinion score (MOS) will be easy to merge both ingredients. Besides, the network requirements and user perception can be fulfilled during medical data, i.e., ECG processing in the healthcare platforms. However, very little is known about the formal methods to optimize the QoS mechanisms in line with the user’s QoE. One of the common problems in manufacturing of UT devices is to find a way for minimizing power consumption and maximizing information integrity (i.e., entropy). The network QoS parameters such as energy consumption, entropy, throughput, delay and jitter are assessed, integrated/mapped in the QoE model. The techniques to meet these challenges depend on the characteristics and capabilities of UT device (for example, LCD panel size, resolution, etc.) during medical media ECG service for elderly patients.
This contribution of this paper is threefold. First, after vast analysis that how the QoS is computed during ECG data processing, for this purpose an adaptive QoS computation algorithm (AQCA) is proposed and compared with other classical methods. Second, novel QoS computation framework is developed by considering the effect of performance indicators, e.g., transmission power, duty cycle and route selection at physical, MAC and network layers accordingly. Third, QoS computation mechanism by proposed AQCA is presented by taking into account the QoE of the end users in the medical healthcare during ECG data processing. Finally, degree of correlation between QoS and QoE for the appropriate QoS computation from user-centric aspect is analyzed in the entire system. To the best of author’s knowledge, this is the first step toward modeling and evaluation of QoS and its correlation with QoE for obtaining the highest perceived level of the end users with large-screen user terminal (UT) devices for big picture and better visualization.
The rest of the paper is divided into following sections. Section 2 reviews the related literature broadly. Section 3 proposes the novel QoS computation framework for intelligent healthcare applications. Experimental results and discussion are presented in Sect. 4. Finally, paper is concluded in Sect. 5.
2 Related work
The requirements of medical media services and QoS are stringent in many cases. The key challenge faced by most of the network operators is the inefficient tools to compute and optimize the QoS in association network and end user perspectives in medical healthcare applications. In the medical media services, people can build different kinds of applications based on bio-signal aggregation and managements in trunk network, sensor networks, long-haul wired networks and other small-scale communication transmission network. Establishing high-reliability network platform is the basis for the development of medical media services, and while providing a high quality of patient/physician experience is one of the main factors to get proper confidence and attention of medical market. From the perspective of the quality of the patient experience, it is very necessary to develop and consider communication network technology for medical media services. However, the subjectivity and complexity of the quality of the patient’s experience decides that objective judgment and distinction of various QoE indicators are very difficult, so currently people establish the mapping relationships between QoE and QoS and speculate QoE level by using the mapping models. The key to establish a good QoS assessment model is to determine the mapping relationship between QoE and key quality indicators (KQI) [3, 4]. The current network’s KPIs such as, delay, jitter, packet loss rate, etc., only reflect network performance and cannot exploit the true perception of the patients accurately. Patient-oriented philosophy requires integration of KPI indexes together to model and evaluate the quality of the patient’s experience. Communication system is influenced by many environmental and social (i.e., patients/physicians financial status) factors, which are assumed as fixed and dynamic in nature, respectively. Moreover, the measurable objective QoE indexes including bandwidth, delay, jitter, throughput, packet loss rate, memory, CPU usage, etc., are considered from the perspective of network layer, application layer and service layer. If these all factors are incorporated into the scope of the study, then it will be very hard to clarify the relationship between the QoE and KPI, because these factors affect each other and show complex relationship.
Many researchers have worked on QoS and QoE. Eidenberger [1] categorized the general media technologies and presented their complete understanding. Dimitrov [2] examined the relationship between medical IoT and big data in healthcare, but their work is not going to deal the issue of QoE optimization, modeling and its connection with QoS. Sodhro and Pirbhulal [5] designed the transmission power control-based energy saving mechanism in WBSN networks; their research also presents that how 5G changes the size of wearable sensor node for medical applications, but they do not focus at the QoE evaluation, modeling and optimization with respect to the QoS. Awobuluyi and Nightingale [6] developed a novel method for assessing QoS in different networks. Chihani and Laghari [7] proposed innovative mobile application for QoE measurement, but their research does not focus on QoS in medical services. Yaacoub and Dawy [8] developed the radio resource management-based method to assess QoE in LTE networks. Chen and Hwang [9] presented the machine learning-based QoE estimation approach during video streaming, but their research does not emphasize on adaptive QoS optimization, modeling and evaluation methods with state-of-the art framework. Wang and An [10] proposed vehicle-to-vehicle communication method for enhancing video quality. Yaacoub and Filali [11] presented adaptive video streaming algorithms for QoE. Sodhro and Zongwei [12] proposed the QoE model for m-health systems, but they did not discuss the mapping models and functions for QoS in medical services. Chen and Zhu [13] proposed multiple communication models for sensor nodes. Xu et al. [14] presented smoothing algorithm for optimizing m-QoS, but their research does not focus on the QoE in medical media services. Li et al. [15] developed physio-bank of real-time ECG database. Sodhro and Pirbhulal [16] presented subjective QoE assessment method through QoS in 3D-image. Goldberger and Amaral [17] presented detailed survey of QoE-aware wireless multimedia systems. [18], design QoE prioritization methods in wireless video transmission. Martini et al. [19] developed novel QoE model for video streaming service, but their research do not focus on mapping functions and evaluation methods for QoE. Sodhro and Pirbhulal [20] discussed different perspectives of QoS measurement in cloud mobile media systems. Authors in [21, 22] developed adaptive algorithms for energy and battery charge saving in medical networks during video and human vital sign signal transmission by using different QoS metrics. Wen et al. [23] proposed QoS optimization techniques based on the probability theory. Sodhro et al. [24] designed the on–off scheme for transmission between devices.
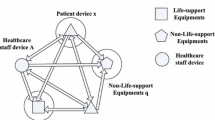
Xu and Zhao [25] presented QoS-based algorithm for different networks and communication in between them. Kang et al. [26] proposed the mathematics-based intelligent decision making technique for medical QoS optimization, but do not consider the concept of QoE its modeling, evaluation and interaction with QoS. Our research adopts their AHP algorithm for prioritizing the network QoS metrics. Dai et al. [27] introduced the QoE assessment model for multimedia services, but their research neglected the modeling, and evaluation of QoE and integrated QoS-QoE for medical media ECG service. Sodhro et al. [28] established the connection between network QoS and QoE for mobile video streaming using different codecs, while there is no discussion about the QoE optimization and its modeling, evaluation and priority setting for network metrics for medical applications. Kim et al. [29] proposed the energy management algorithm in WBSN, but they do not consider the QoE modeling and optimization and its trade-off with QoS. Pal et al. [30] designed the battery-friendly strategies with network and system QoS optimization such as transmission energy and battery charge, respectively, in wireless capsule endoscopy, while QoE evaluation and its correlation with QoS is over simplified. Sodhro et al. [31] developed the QoE model for multimedia IoT, but their research do not focus at the QoE evaluation and modeling in medical application and relation between QoS and QoE. In above all research works, the unified QoS, QoS-QoE modeling, evaluation and mapping indexes for medical media services are not seriously focused and one cannot evaluate QoE and correlate QoE-QoS effectively. Even with the use of old KPI evaluation indexes such as at the data link layer, network layer, physical layer to give the considerations of the QoE model to all aspects of patients, the establishment of the QoE-QoS model will be very complicated [32,33,34,35]. There is, however, something that can be best done at elderly patient’s side with large-screen UT device, especially when it comes to modeling, evaluation and correlation of QoE, QoE-QoS, respectively, for medical ECG service. For further details see Fig. 1. Researchers in [36,37,38,39,40] present the fog computing scheduling, real-time applications of image processing in IoT, but there is need to portray the QoS optimization. Authors in [41,42,43,44] discuss in details the emerging tools and techniques for the IoT-based platforms in different domains such as healthcare, business, industries, etc., but it is imperative to focus at the QoS in medical healthcare. Similarly, authors in [45,46,47,48] design the bio-signal analysis, heat rate monitoring, smart home and biofeedback-based healthcare examination, but in QoS optimization, monitoring is very vital for the medical applications.

QoS computation framework for medical data processing
As most of the previous researches just overlooked the QoS optimization during medical healthcare data processing, it is dire need to develop, discuss and design the state-of-the art QoS, QoS-QoE, methods, frameworks and tools for efficient evaluation of the entire medical platform.
3 Proposed adaptive QoS computation framework for medical data processing
In this proposed adaptive QoS computation framework for medical data processing, several key steps are taken for the efficient allocation of resources at the different layers. Firstly end user is connected to the four key steps for example, QoS monitoring, QoS examination, QoS optimization and QoS adaptation in association with network layers, i.e., physical (transmission power control, modulation level), MAC (duty cycle) and network (routing and path selection) accordingly. Besides, QoS is fairly computed while transmitting the sensitive healthcare data to the intended destination. Proposed framework’s main objective is to satisfy the end user’s (patients and physicians) requirements while transferring data to the intended destination.
3.1 Proposed adaptive QoS computation algorithm (AQCA)
Figure 2 reveals the numerous resources important for the effective and efficient computation of QoS in healthcare applications. In this subsection, an adaptive QoS computation algorithm (AQCA) is proposed to efficiently manage and monitor the QoS during medical data processing in the healthcare applications by adopting the key performance indicators at several open systems interconnection (OSI) layers. The QoS metrics for instance, throughput, delay, transmission power, duty cycle and networking, are taken into account for assessing the performance level of the entire system. In addition, the key purpose of the proposed AQCA is to compute the QoS in a fair and intelligent way to satisfy the user’s and system’s requirement. In this scenario, QoS has linear and strong ties with the user perception, i.e., QoEs. Hence, it is very vital to establish the trade-off between subjective entities and objectives ingredients (e.g., throughput, delay, jitter, transmission power, duty cycle and route selection) during medical data processing in the healthcare domain. Besides, it is mandatory to develop the state-of-the art QoS frameworks, tools and methods for computing the overall performance of the medical market from both the user and network aspects. Because it is well-known fact that QoS is the validated to the network performance to entirely characterize the system from different perspectives, while QoE is highly likely related to the user expectations, perceptions and their satisfaction level. So, after integrating both entities there will be mutual and collaborative interaction between network performance and end users satisfaction to meet the demands of incoming medical healthcare applications.
where TP and \(x\) define the transmission power and maximum payload size

Resource computation for QoS in medical healthcare applications
Description of the parameters is defined as follows: \(T_{\text{PHR}}\) = transmission time of PHY header; \(T_{\text{pre}}\) = transmission time of preamble; \(R_{\text{Data}}\) = data transmission rate; \(T_{\text{s}}\) = CSMA slot length; \(T_{{\rho {\text{SIFS}}}}\) = short inter-frame spacing time; \(T_{\text{CCA}}\) = clear channel assessment time; MHR = MAC header; \(FTR\) = MAC footer; \(T_{{I + {\text{ACK}}}}\) = immediate acknowledgement time slot; \(\tau\) = propagation delay
\(\overline{\text{CW}}\) is the average back-off time; \(T_{\text{Data}}\) is the transmission delay of the Physical Layer Protocol Data Unit (PPDU)
where \(T_{\text{ON}}\) active or wake up time duration of any node; \(T_{\text{OFF}}\) sleep time duration of any node
where \({\text{SoC}}\) is the state of the charge (SoC) to analyze the duty cycle
where M is the priority matrix and \({\text{Tot}}_{\text{QoS}}\) is the total QoS and its value is assumed as 1, as shown in Eqs. (9) and (10) for computing the QoS from impairment factors.
where \(X\), \(B_{\text{up}}\) are the satisfactory level of user (in terms of high visualization, longer and better service time, etc.) and upper bound of the QoS according to the type of the network (i.e., wired or wireless). As our experiment is conducted in the wireless, i.e., ZigBee and WiFi environment to determine \(B_{\text{up}}\). The S presents the service type, i.e., for normal patients (lowest priority) or emergency patients (highest priority). The L reveal the average length of the ECG data packets.
Many research works have been conducted on the correlation between QoE and QoS, but every method is different. The most important issue is that the IQX (interdependency between QoS and QoE) assumption associate QoS and QoE to minimize the performance and user perception degradation about network performance during medical data processing in healthcare.
Besides, the weight to the QoS parameters is assigned and prioritized according to the conventional methods without any logic which is very cumbersome way with less clearance. So, we prioritize the QoS components and allocate them weights by proposing intelligent decision making method known as adaptive QoS computation algorithm (AQCA), which is the beauty of our research. For further details, see Figs. 3 and 4.

Pseudo code of QoS computation in medical healthcare applications

Flowchart of the adaptive QoS computation algorithm in healthcare
3.2 QoS computation mechanism
Besides, proposed AQCA fairly allocates the resources during medical data processing and computes the QoS in an efficient manner. Correlation between widely used QoS and QoE entities has been presented, and suitable integrated solution is recommended for key QoS parameters such as transmission power, modulation level, throughput, delay, jitter at physical layer, duty cycle at MAC layer and route selection at network layer, consequently. For more details, see Fig. 5.

QoS computation using proposed AQCA during medical data processing
4 Experimental results and discussion
This section presents the extensive experimental analysis of the QoS at physical, MAC and network layers during medical data processing in the healthcare applications. The several performance ingredients are adopted such as, transmission power, duty cycle and route selection at physical, MAC and network layers accordingly. In this section, we present the detailed experimental test bed in the MATLAB by considering the real-time data sets of human biological signals from the world’s largest database title National Information Communication Technology Australia (NICTA) [28]. They key purpose of this entire setup is to provide the ease and comfort to the disable patients by building the edge-computing-based platform. To save the lives of old age and disable patients from more hardships with minimum resources, we developed the sensor network individually at their bodies which is easily accessible and ad hoc to carry easily at anywhere. In that situation, wireless channel is the main ingredient to be focused and hence the transmission power control to effectively monitor the smart healthcare. Due to less satisfactory performance of the conventional methods, we propose the novel adaptive QoS computation algorithm (AQCA) to adaptively allocate the wireless channel slot and the power level to the separate network of the disabled patients at their body and then compare with the Baseline method. In addition, performance of the proposed AQCA and Baseline methods is examined in terms of the several network indicators for instance, energy bit per noise ratio, bit error rate, received signal strength indicator (RSSI), data rate, energy drain, etc. Experimental results are extracted on the basis of the adaptive transmission power control mechanism and channel characteristic according to the human body shape. Energy bit per noise ratio and bit error rate values in decibel from 0 to 15 dB are considered.
It is observed that the performance of the modulations level methods for example, binary, quadrature shift keying and multiple-array quadrature modulation (M-QAM) is examined in terms of the \({{E_{b} } \mathord{\left/ {\vphantom {{E_{b} } {N_{0} }}} \right. \kern-0pt} {N_{0} }}\) and BER as depicted in Figs. 6, 7 and 8, respectively. We analyzed that there is a close coordination between simulation and theoretical results for BPSK (SimBER: 0.081, TheoBER: 0.078), QPSK (SimBER: 0.146, TheoBER:0.078) and QAM (SimBER: 0.144, TheoBER: 0.139) accordingly. It is further interpreted that as \({{E_{b} } \mathord{\left/ {\vphantom {{E_{b} } {N_{0} }}} \right. \kern-0pt} {N_{0} }}\) increases, BER gets higher.

Relationship between energy bit per noise ratio and bit error rate for BPSK

Relationship between energy bit per noise ratio and bit error rate for QPSK

Relationship between energy bit per noise ratio and bit error rate for QAM
In Fig. 9, it is analyzed that as the value of roll-off factor increases energy dissipation reduces. Besides, roll-off factor is the key ingredient to deal with the transceiver and power amplifier’s functionality in the short range and ad hoc networks. Due to small distance between sensor devices at the patient’s body, it is very important to extract the entire features of the wireless channel and hence the transmission power levels. Hence, it can be said that power drain and the distance are linearly coordinated.

Trade-off between modulation level and energy drain
Figure 10 reveals the relationship between the time and QoS computation for the proposed AQCA and the Baseline. It is analyzed that with the increase in the time QoS will be computed at high and low levels for the proposed AQCA and Baseline accordingly. Because of the resource-constrained and delay-sensitive nature of the healthcare sensor nodes, it is very necessary to properly establish the relationship between the channel characteristics and the power allocation. Also the dynamic features of the human body the developed separate networks at the patient’s body faces several challenges such as, packet loss, low quality of service, less RSSI and high power drain. So, proposed AQCA is the suitable candidate to handle most of the aforementioned challenges. In Fig. 11, we draw the trade-off between date rate and QoS computation during medical data processing proposed AQCA and Baseline for healthcare applications. It is examined that with the increase in the distance higher data rate is needed to perform the transmission process. In addition, it is examined that proposed AQCA needs more data rate for performing better and efficiently unlike Baseline, because later needs to transmit less information and exploits large energy drain. The trade-off between QoS and QoE in terms of performance indicator jitter is presented for proposed AQCA and Baseline in Fig. 12. We observed that less and high jitter occurred during medical data processing by Proposed AQCA and Baseline accordingly in the healthcare applications.

QoS computation with respect to time

Relationship between data rate and QoS computation in healthcare

Relation between QoS and jitter
Figure 13 reveals the relationship between QoS and QoE for the performance metric, i.e., throughput during the medical data processing for proposed AQCA and Baseline consequently in healthcare applications. It is examined that proposed AQCA has more throughput than the Baseline; thus, former is potential candidate for most of the emergency and critical applications.

Relation between QoS and throughput
In parallel with transmission power, duty cycle and route selection entities for examining the performance of the healthcare system in the presence of the adaptive and intelligent QoS computation technique, the delay, jitter and throughput are also the key role players. Due to the their emerging and unforgettable role since long time in analyzing the performance of most of the systems such as, wireless networks, wired networks, short range and long range networks etc. Their scope has been vitalized and extended in the healthcare domain; that is why by keeping this highly demanding aspect in the mind, we have taken into account these classical performance indicators for analyzing the status of the medical market.
In Fig. 14, we analyzed the throughput of the proposed AQCA and Baseline with trade-off between QoS and QoE during medical data processing. It is examined and observed that there is high and low throughput from proposed AQCA and Baseline, respectively, as a guideline for the future healthcare applications. Besides, throughput is the key performance factor for every network for characterizing the entire behavior of the system.

Relation between QoS and delay
5 Conclusion and future research
Medical data processing and transmission has become the potential solution for many emerging healthcare applications. However, efficient computation of QoS is very vital for landscape of the medical world by adaptively adjusting the network metrics for instance, transmission power drain, delay, jitter, throughput at physical layer; duty cycle at MAC layer; and suitable route selection at network layer accordingly. In addition, the integration of QoS with QoE is the challenging aspect to be handled carefully by adopting the sensor-based portable devices with large screen for the big and better picture of the incident. Medical healthcare market has been revolutionized with the dynamic boom in the emerging technologies for instance, wireless short range networks to embedded platform in this highly demanding era. Emergency patients are facilitated by adopting the fog computing-based adaptive power control and QoS management in the healthcare environment. Therefore, in this paper after vast analysis that how the QoS is computed during ECG data processing we first propose an adaptive QoS computation algorithm (AQCA) and compared with other classical methods. Second, novel QoS computation framework is developed by considering the effect of performance indicators, e.g., transmission power, duty cycle and route selection at physical, MAC and network layers accordingly. Third, QoS computation mechanism by proposed AQCA is presented by taking into account the QoE of the end users in the medical healthcare during ECG data processing. Finally, degree of correlation between QoS and QoE for the appropriate QoS computation from user-centric aspect is analyzed in the entire system. In near future, a correlation model between QoS impairment factors (i.e., throughput, delay and jitter) and QoE is built in order to assess the needs and expectations of medical staff. Besides, QoS-QoE correlation model will be developed for more network metrics and other objective factors for video transmission in medical health.
Change history
29 April 2024
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1007/s00521-024-09874-w
References
Eidenberger H (2012) Handbook of multimedia information retrieval: “the common methods of audio retrieval, biosignal processing, content-based image retrieval, face, text retrieval and video surveillance”. Austria
Dimitrov DV (2016) Medical internet of things and big data in healthcare. Healthc Inform Res 22(3):156–163
Reichl P, Egger S (2015) Towards a comprehensive framework for QoE and user behavior modeling. In: 7th international workshop on quality of multimedia experience
ITU-T G 107 (2015) The e-model, a computational model for use in transmission planning. Geneva
Sodhro AH, Pirbhulal S (2018) Power control algorithms for media transmission in remote healthcare systems. IEEE Access 6(1):1–8
Awobuluyi O, Nightingale J (2015) Video quality in 5G networks: context-aware QoE management in the SDN control plane. In: IEEE international conference on computer and IT
Chihani B, Laghari KR (2013) User-centric quality of experience measurement. In: International conference on mobile computing, applications and services. pp 33–46
Yaacoub E, Dawy Z (2014) Fair optimization of video streaming quality of experience in LTE networks using distributed antenna systems and RRM. J Appl Math 2014(2014):1–12
Chen X, Hwang J-N (2015) A near optimal QoE-driven power allocation scheme for scalable video transmissions over MIMO systems. IEEE J Sel Top Signal Process 9(1):76–88
Wang L, An N (2013) Power-aware wireless communication system design for body area networks. E Health Telecommun Syst Netw (ETSN) J 2(2):23–28
Yaacoub E, Filali F (2015) Enhancement of SVC video streaming over vehicular networks using cooperative LTE/802.11p Comm. IEEE J Sel Top Signal Process 9(1):37–49
Sodhro AH, Zongwei L (2018) Mobile edge computing based QoS optimization in medical healthcare applications. Int J Inf Manag (IJIM) 18:1–21
Chen C, Zhu X (2015) Rate adaptation and admission control for video transmission with subjective quality constraints. IEEE J Sel Top Signal Process 9(1):22–36
Xu D, He C, Li Y (2013) Improving quality of experience in M-health monitoring system. In: 35th annual international conference of the IEEE EMBS Osaka, Japan
Li Y, Qiao D, Xu Z, Xu D, Miao F (2012) Energy-model-based optimal communication systems design for wireless sensor networks. Int J Distrib Sens Netw 2012(2012):1–11
Sodhro AH, Pirbhulal S, Sodhro GH, Gurtov A, Muzammal M, Luo Z (2018) A joint transmission power control and duty-cycle approach for smart healthcare system. IEEE Sens J 99:1–8
Goldberger AL, Amaral LAN (2000) PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation 101(23):215–220
Doutre MC, Nasiopoulos P (2012) Rendering 3-D high dynamic range images: subjective evaluation of tone-mapping methods and preferred 3-D image attributes. IEEE J Sel Top Signal Process 6(5):597–610
Martini MG, Chen CW, Zhu X (2012) QoE-awarewireless multimedia systems. IEEE J Sel Areas Commun 30(7):53–56
Sodhro AH, Pirbhulal S (2018) Convergence of IoT and product lifecycle management in medical health care. Future Gener Comput Syst 86(2018):380–391
Ojanper T, Uitto M (2014) QoE-based management of medical video transmission in wireless networks. In: IEEE/IFIP network operations and management symposium
Laghari KUR, Pham TT, Nguyen H, Crespi N (2012) QoM: a new quality of experience framework for multimedia services. In: IEEE symposium on computers and communications (ISCC)
Wen Y, Zhu X, Rodrigues JJPC (2014) Cloud mobile media: reflections and outlook. IEEE Trans Multimedia 16(4):885–901
Sodhro AH, Pirbhulal S, Sodhro GH (2018) An energy-efficient algorithm for wearable electrocardiogram signal processing in ubiquitous 3 healthcare applications. MDPI Sens 8(3):923
Xu Y, Zhao X (2014) Robust power control for underlay cognitive radio networks under probabilistic quality of service and interference constraints. IET Commun 8(18):3333–3340
Kang J-W, Hussain A, Kim S-H et al (2015) Link scheduling schemes with on–off interference map for device to device communications. IET Commun 9(3):359–366
Dai Z, Liu J, Wang C et al (2015) QoS-based device to device communication schemes in heterogeneous wireless networks. IET Commun 9(3):335–341
Sodhro AH, Shaikh FK, Pirbhulal S, Lodro MM, Shah MA (2017) Medical-QoS based telemedicine service selection using analytic hierarchy process. In: Khan SU, Zomaya AY, Abbas A (eds) Handbook of large-scale distributed computing in smart healthcare. Springer, Cham, pp 589–609
Kim HJ et al (2014) QoE assessment model for multimedia streaming services using QoS parameters. J Multimedia Tools Appl 72(2014):2163–2175
Pal D, et al (2017) Effect of network QoS on user QoE for a mobile video streaming services using H.265/VP9 Codec. In: 8th international conference on advances in information technology (IAIT2016), vol 111(2017), pp 214–222
Sodhro AH, Sekahri A, Ouzrout Y (2018) Energy-efficiency comparison between data rate control and transmission power control algorithms for wireless body sensor networks. Int J Distrib Sens Netw (IJDSN) 14(1):1–18
Floris A et al (2016) Managing the quality of experience in the multimedia internet of things: a layered-based approach. MDPI Sens 16(12):1–21
Mahmud R, et al (2018) Cloud-fog interoperability in IoT-enabled healthcare solutions, ICDCN’18, January 4–7, pp 1–10
Li Y (2017) Edge computing-based access network selection for heterogeneous wireless networks. Networking and Internet Architecture [cs.NI]. Université Rennes 1
Jridi M et al (2018) SoC-based edge computing gateway in the context of the internet of multimedia things: experimental platform. J. Low Power Electron Appl 8(1):1
Rahbari D, et al (2018) Scheduling of fog networks with optimized knapsack by symbiotic organisms search. In: Proceeding of the 21st conference of FRUCT association. pp 1–6
Gomes SL, de Rebouças ES, Neto EC, Papa JP, de Albuquerque VHC (2017) Embedded real-time speed limit sign recognition using image processing and machine learning techniques. Neural Comput Appl 35(1):573–584
Sodhro AH, Pirphulal S, Sekhari A, Ouzrout Y (2018) Green media-aware medical IoT system. Multimedia Tools Appl. https://doi.org/10.1007/s11042-018-5634-0
de Albuquerque VHC (2018) Robust automated cardiac arrhythmia detection in ECG beat signals. Neural Comput Appl 29(3):679–693
Rebouças Filho PP, da Silva Barros AC, Ramalho GLB, Pereira CR, Papa JP, de Albuquerque VHC (2017) Automated recognition of lung diseases in CT images based on the optimum-path forest classifier. Neural Comput Appl 27(1):1–14
Rodrigues JJPC, Segundo DBDR (2018) Enabling technologies for the internet of health things. IEEE Access 6(2018):13129–13141
da Cruz MAA, Rodrigues JJPC, Al-Muhtadi J (2018) A reference model for internet of things middleware. IEEE Internet of Things J 5(2):871–883
Lakshmanaprabu SK, Shankar K, Khanna A, Gupta D (2018) Effective features to classify big data using social internet of things. IEEE Access 6(2018):24196–24204
Sodhro AH, Pirbhulal S, Sodhro GH (2018) ‘5G-based transmission power control mechanism in fog computing for IoT devices. MDPI Sustain 10(4):1–17
Moraes JL, Rocha MX, Vasconcelos GG, Vasconcelos Filho JE (2018) Advances in photopletysmography signal analysis for biomedical applications. Sensors 18(6):1–20
Hussein AF, Kumar A, Burbano-Fernandez M (2018) An automated remote cloud-based heart rate variability monitoring system. IEEE Access 6:1–10
Pirbhulal S, Zhang H, Alahi MEE, Ghayvat H, Mukhopadhyay SC, Zhang Y-T et al (2016) A novel secure IoT-based smart home automation system using a wireless sensor network. Sensors 17:69
Wanqing Wu, Pirbhulal S (2015) Assessment of biofeedback training for emotion management through wearable textile physiological monitoring system. IEEE Sens J 15(12):7087–7095
Acknowledgements
This work is partially supported by Natural Science Foundation of China 6171101169, National Key R&D Plan-Key Special Plan on Public Security Risk Mitigation/Response 2017YFC0804003, Technologies and Equipment Guangdong Education Bureau Fund 2017KTSCX166, the Science and Technology Innovation Committee Foundation of Shenzhen JCYJ20170817112037041, Science and Technology Innovation Committee Foundation of Shenzhen (Grant No. ZDSYS201703031748284). Also for this research, Andrei Gurtov was supported by the Center for Industrial Information Technology (CENIIT) Project 17.01. This work is supported in part by the HEC Pakistan under the START-UP RESEARCH GRANT PROGRAM (SRGP)#21-1465/SRGP/R&D/HEC/2016, and Sukkur IBA University, Sukkur, Sindh, Pakistan.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest between all authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been retracted. Please see the retraction notice for more detail:https://doi.org/10.1007/s00521-024-09874-w
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sodhro, A.H., Malokani, A.S., Sodhro, G.H. et al. RETRACTED ARTICLE: An adaptive QoS computation for medical data processing in intelligent healthcare applications. Neural Comput & Applic 32, 723–734 (2020). https://doi.org/10.1007/s00521-018-3931-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00521-018-3931-1