
Abstract
Increase in body mass index value is a serious health problem across the world. Humans with high body mass index value have the higher probability of getting the cardiovascular disease and high blood pressure. The proposed work is concerned in predicting the probability of CVD and high blood pressure in India. The disease has been predicted with body mass index value; from the health reports of India, the pervasiveness of CVD and HBP is identified. The demographic health survey 2016 of India is used in this work. Bayesian model is used to find the pervasiveness of CVD and HBP based on the gender and the place of living. Out of 432 articles studied, 34 articles suggested the pervasiveness of CVD and HBP. Pervasiveness of CVD increased (95% of interval) rapidly between 1992 and 2016 from 3.0% (0.3–5.7) to 16.4% (9.4–16.2) for men, and from 5.2% (2.3–8.6) to 15.4% (3.3–18.6) for women. Pervasiveness of high blood pressure increased rapidly between 1992 and 2016 from 11.0% (8.6–17.4) to 21.4% (19.4–23.6) for men and from 14.0% (4.3–16.7) to 20.4% (5.6–25.6) for women. The pervasiveness of CVD in 2030 is predicted as 24.6% (13.6–37.8), and pervasiveness of high blood pressure is predicted to be 21.7% (19.6–27.8). The annual average of pervasiveness of CVD is high for women in village areas, and pervasiveness of high blood pressure is found high for men in city regions. The cutoff point for pervasiveness of CVD for overall population is 23.02 kg/m2.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The pervasiveness of cardiovascular disease and high blood pressure has been increasing rapidly in India, whereas the cardiovascular disease and high blood pressure are serious health concerns [1,2,3]. The cardiovascular disease is identified as a serious health issue, and it may damage the heart and can cause death [4]. In developing nations, around one-third of the people have high blood pressure and one in five has cardiovascular disease [5]. Obesity is considered as one of the modifiable diseases that causes cardiovascular disease, and the government is predicting the obese people through body mass index. The cardiovascular disease and blood pressure are considered as non-communicable diseases [6,7,8,9]. In case of non-communicable disease, the prediction of cardiovascular disease and blood pressure is done through the body mass index value; this could help the government and health organizations to take necessary actions [10]. The pervasiveness of cardiovascular disease and high blood pressure seems increasing rapidly in India. In a recent study, it has been said that the incidence of cardiovascular disease is 9.0% and high blood pressure is 26.7% in adults [11, 12]. The connection between the CVD and BMI is not clear [13, 14] because of the population-based data. Several studies have undergone to know the relationship between BMI (underweight, normal weight, and overweight) [15] and the risk of cardiovascular disease or high blood pressure [16]; from all these works, it’s unclear whether CVD or HBP increases based on the BMI categories [17]. Befitting optimal cut-point for the body mass index is very useful in predicting the risk groups that causes the cardiovascular and blood pressure diseases [18, 19]. The current method for predicting the disease is based on the international cut-point value considering Asian and European population, and it may fail in case of African population because their fat percentage is more compared to the Asian and European [20, 21]. So country-specific cutoff point has to be obtained to predict the heart disease before it occurs. The country’s wealth or economic statuses also induce in high BMI percentage, and very few works say about this issue. Finally, the pervasiveness of cardiovascular disease and high blood pressure in various studies is reported in India [22,23,24,25]. The proposed method finds the relationship between BMI and CVD or HBP and also finds a befitting cutoff point to predict the disease.
2 Related works
The present works are based on the body mass index value, which is calculated as weight divided by height meter square [26]. The height and weight of children and adults are influenced by many factors such as diet, disease, and infections. The BMI is a way of indicating the health by calculating the height and weight [27]. The risk of cardiovascular disease and high blood pressure is underrated, and with the help of promotion it can be changed [28]. Since the fat percentage differs from one nation to another, it’s necessary for studying pervasiveness of disease in each country separately (Holland et al. 2011 [29]). From the study, it’s found that Philippines people have higher risk of high blood pressure when compared to the others [30].
In another study of 98,943 patients, the risk of cardiovascular disease and high blood pressure is high in American women when compared to Asian men (Zhao et al. 2015 [31, 32]). The increased risk of cardiovascular disease and blood pressure in American women is because of overweight and obesity (Holland et al. 2015 [33]). The threshold value of determining the body mass index value of Americans has not been established (Ancheta et al. 2014). The current value of determining the overweight category is 26.7% and obesity category is 34.7% (Cornnor et al. 2006 [34]). The Asians have the high metabolic syndrome, and their threshold rate is lower in determining the CVD and blood pressure [35] (Table 1).
Lower body mass index is suggested for American women because of the increased metabolic rates in women (Banda et al. 2015 [36]). Among all other countries, the Filipinos have separate living styles, culture, and generic patterns [37]. The body mass index is the important term in determining the obesity and overweight categories [38]. The waist circumference and waist-to -height ratio give more accurate results in predicting the disease when compared to body mass index value [39]. According to the International Heart Disease Foundation, the threshold value for women is 31.5%. However, the lower threshold value has to be applied for Filipino women when compared to the other nations [40].
The medicinal work has been performed in order to find the relationship between the body mass index value and obesity, cardiovascular disease, cholesterol, stroke, heart attack, and ischemic heart disease [41]. The current method for predicting disease is based on the international cut-point value considering Asian and European populations, and it may fail in case of African population because their fat percentage is more compared to the Asian and European [42, 43]. So country-specific cutoff point has to be obtained to predict the heart disease before it occurs [44, 45]. The country’s wealth or economic statuses also induce in high BMI percentage, and very few works say about this issue. Finally, the pervasiveness of cardiovascular disease and high blood pressure in various studies is reported in India [45,46,47]. The proposed method finds the relationship between BMI and CVD or HBP and also finds a befitting cutoff point to predict the disease (Tables 2 and 3).
The disease caused by high BMI value is seen in 32% of adults. The body mass index is also calculated based on age, gender, place of living, marital status, education, and income rate. The cardiovascular disease is higher in case of rural women of about 34%, and in case of high blood pressure based on the body mass index values they categorize weight into underweight, normal, overweight, and obesity.
The mean body mass index value for male is 23.4% and for women is 26.5%. High body mass index value is found in age-group of ≥ 30. The countries with no medical data are avoided from finding the body mass index values. The prevalence of disease can be predicted by calculating the mean body mass index value of male and female.
3 Methods
3.1 Data sources
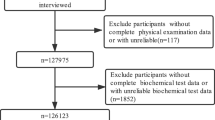
Data were searched using two methods. First, PubMed was searched from its inception to August 2016, using keywords such as cardiovascular disease, blood pressure, fasting blood glucose, and India. Search was done based on proof related to the disease, which helped to find the prevalence of disease based on the place of living and status. Secondly, the search was done using Demographic Health Survey of India (DHSI), which it uses three-cluster sampling method to get the data from 8934 members of over 30 years. The overall rate of response is 90.25%; for additional information, refer to the DHL website [21].
3.2 Recognition of CVD and HBP
High blood pressure values are classified into systolic and diastolic blood pressure based on the glucose level: ≥ 140 mg and ≥ 90 mg, respectively. A body mass index mean value ≥ 30% predicts the incidence of cardiovascular disease.
3.3 Discombobulate variables
With respect to age and gender, some additional characteristics are collected. The first characteristic is qualification like no education, primary education, and secondary education. The second characteristic is place of living (city, village). The third characteristic is marital status (unmarried, newly married). The fourth one is economic or income status (poorest, poor, middle class, and rich). Finally, location-based characteristic is also collected (northeast, central, west, and southeast).
4 Results
4.1 Prediction of CVD and HBP
From the various studies, the record of 435 works has been collected, by leaving the title and related works done. In total, 53 records have been taken, out of which 12 have been left out because of the information stated in appendix. Based on 43 articles, it shows the prevalence of CVD and HBP. On which, 38 articles predict the cardiovascular disease and high blood pressure in the humans.
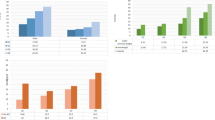
Figure 1 represents the prevalence of cardiovascular disease and blood pressure from 1992 to 2016, which shows that there is an increasing trend. The prevalence of CVD increases to 7% in women and 6% in case of men. Likewise, the high blood pressure increases to 2% in women and 7% in men. The increase in the prevalence of cardiovascular disease and blood pressure in men is higher in 2011 and 2015. While considering the place of living, the prevalence of the disease is higher in city people compared to the people living in villages. In women, the prevalence of disease is predicted to increase to 15.7% (0.8–18.9) in 2021 compared to 3.0% (0.3–5.7) in 1992. In men, it increases from 5.2% (3.3–7.2) to 18.7% (0.2–21.4). By the year 2030, the prevalence of cardiovascular disease is predicted to be 22.23% in women and 34.6% in men with 24.45% overall. For the high blood pressure, the prevalence is predicted to reach 32% in women and 36.7% in men with 34.5% overall.

Prevalence of CVD and HBP during 1992–2030
The predicted prevalence varies based on the place of living, i.e., the prevalence of high blood pressure increases rapidly in city areas.
The CVD is found high in women in rural areas, and in 2010 it increased more than men.
4.2 Cardiovascular disease and high blood pressure by BMI levels
Survey data based on the BMI values are represented in Table 4. People with high BMI are said to have systolic, diastolic blood pressure, and fasting blood glucose. The people with high BMI are said to live in city areas; they are educated and they are all high in economic status. The adults in city areas are said to have the incidence of 12% of cardiovascular disease and 25% of high blood pressure. Figure 2 shows modified age and gender BMI values based on 8 categories such as place of living, marital status, educational qualification, and economic status. The mean of high blood pressure is modified for less than ≥ 20 kg/m2, and this value goes high when the value of BMI also increases. The prevalence of cardiovascular disease and high blood pressure seems to increase after > 20 mg/m2.

Age- and gender-modified mean and the prevalence of characteristics of body mass index
4.3 Association of BMI with CVD and HBP
The prevalence of CVD and HBP is represented in Table 5. For the cardiovascular disease, the BMI levels are 23.4–25.6 at the lower case. The CVD is found in people with BMI values ranging 14.7–16.6, 16.7–19.2, and 19.3–21.3. The OR values are 0.34 (0.23–0.41), 0.47 (0.35–0.51), and 0.61 (0.54–0.73). In case of higher odds the values are 23.4–24.7 and 24.8–29.6, and the OR values are 1.01 (0.7–1.6) and 3.4 (2.8–4.2). For high blood pressure, the prevalence lies between the body mass index and high blood pressure. In case of high blood pressure, BMI values are adjusted according to the values, whose category lies in the range 23.4–26.7. The lower case of values is found between (0.13 and 0.23) > 15 mg and higher values are found in (1.78–7.36) > 30 mg (Table 6).
4.4 Optimal cut-point for CVD and HBP
The optimal cut-point values for cardiovascular disease and high blood pressure are represented in Table 7. The results show that the age- and gender-adjusted optimal cut-point for cardiovascular disease and high blood pressure in Indians is modified to 20 mg and it gets maximum value and distance. The optimal body mass index cut-point for cardiovascular disease is 20.02 kg/m2 for men with specificity of 57.4% and sensitivity of 57.3% in men and 23.03 kg/m2 for women with specificity of 66.5% and sensitivity of 57.5%. The body mass index varies in place of living, educational status, and marital status, for example, 21.6% for age 35–39 years and 23.4% for age above 50 years. The area under the ROC curve is 0.64 for women and 0.65 for men. By which BMI is used to find the prevalence of cardiovascular disease and high blood pressure. Due to the small change in optimal points, the cut-point is 22.0 kg/m2 for men and 23.0% kg/m2 for women.
5 Discussion
The current study involves 65 published articles from 32 studies from the year 1992, and population survey was conducted in 2011 from the continuous studies. The prevalence of cardiovascular disease and high blood pressure is predicted to be 25 and 34%. The rate of BMI is larger for women in village areas, and for men it’s large in city areas. The rate of cardiovascular increases as the body mass index increases. In case of type 2 cardiovascular diseases, the optimal cut-point for men is 23.0 and 24.0 kg/m2 in female. The first step to find the prevalence of cardiovascular disease and high blood pressure is done manually. On population-based data, the prevalence of cardiovascular disease and high blood pressure is found to be 11 and 26%.
The prevalence of cardiovascular disease and high blood pressure was found in Bangladesh (11%), China (10%), and Korea (8%) [32,33,34,35,36,37]; the prevalence of high blood pressure was found in India (25%), China (24%), and Korea (26%). The cardiovascular disease and high blood pressure vary on different parameters such as place of living, educational status, economic status, and marital status. The prevalence of cardiovascular disease increased to 13% in women and 12% in men in the year 2015 and predicted to be 24% in women and 34% in men by the year 2030.
From the previous reports, it’s predicted that body mass value greater than 22.5% kg/m2 is considered as dangerous for cardiovascular disease and high blood pressure. The optimal cutoff point for cardiovascular disease is 22.0% kg/m2 for men and 23.0% kg/m2 for women. The previous study stated that the optimal cut-point for cardiovascular disease for women is 21% and for men it is 22%. The difference in value of our proposed model data and previous reports is because of their place of living and their sample size. Our data are similar to the data of other countries like China with overall prevalence of 24%, Indonesia with 22%, and Vietnam with 21% [35]. The present model has many advantages since it has considered the place of living, marital status, educational qualification and the economic status of the participants and it also has large data size.
The optimal cutoff point analysis suggests that anything beyond 22.5 kg/m2 is risky, and body mass index value increases when the risk increases. These reports do not have attributes like smoking habits, drinking, physical activities, and waist circumference, so the model can’t be used for regression model in predicting the risk between body mass index and cardiovascular disease.
6 Conclusion
The findings of the present study show that the prevalence of cardiovascular disease and high blood pressure increases rapidly in women present in village areas and in case of men it increases in city areas. The BMI more than 22.5% kg/m2 can lead to the cardiovascular disease and high blood pressure. The optimal cutoff point for men is 22.0% kg/m2 and for women is 23% kg/m2. From the reports, if the body mass index increases, then there is an increase in rate of cardiovascular disease and high blood pressure in India that can be prevented.
Change history
17 July 2024
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1007/s00521-024-10080-x
References
NCD Risk Factor Collaboration (NCD-RF) (2016) Worldwide trends in diabetes since 1980: a pooled analysis of 751 population based studies with 4.4 million participants. Lancet 387:1513–1530
NCD Risk Factor Collaboration (NCD-RF) (2016) Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 387:1377–1396
Balan EV, Priyan MK, Gokulnath C, Devi GU (2015) Fuzzy based intrusion detection systems in MANET. Procedia Comput Sci 50:109–114
Lim SS, Vos T, Flaxman AD et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: asystematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2224–2260
Devi GU, Balan EV, Priyan MK, Gokulnath C (2015) Mutual authentication scheme for IoT application. Indian J Sci Technol 8(26). https://doi.org/10.17485/ijst/2015/v8i26/80996
Biswas T, Islam A, Rawal LB, Islam SM (2016) Increasing prevalence of diabetes in Bangladesh: a scoping review. Public Health 138:4–11
Tuan NT, Adair LS, Suchindran CM, He K, Popkin BM (2009) The association between body mass index and hypertension is different between East and Southeast Asians. Am J Clin Nutr 89:1905–1912
Priyan MK, Devi GU (2017) Energy efficient node selection algorithm based on node performance index and random waypoint mobility model in internet of vehicles. Clust Comput 1–15. https://doi.org/10.1007/s10586-017-0998-x
Huxley R, James WP, Barzi F et al (2008) Ethnic comparisons of the cross-sectional relationships between measures of body size with diabetes and hypertension. Obes Rev 9:53–61
Devi GU, Priyan MK, Balan EV, Nath CG, Chandrasekhar M (2015) Detection of DDoS attack using optimized hop count filtering technique. Indian J Sci Technol 8(26). https://doi.org/10.17485/ijst/2015/v8i26/83981
Chowdhury MAB, Uddin MJ, Haque MR, Ibrahimou B (2016) Hypertension among adults in Bangladesh: evidence from a national cross-sectional survey. BMC Cardiovasc Disord 16:1
Rahman MS, Akter S, Abe SK et al (2015) Awareness, treatment, and control of diabetes in Bangladesh: a nationwide population-based study. PLoS ONE 10:e0118365
Gokulnath C, Priyan MK, Balan EV, Prabha KR, Jeyanthi R (2015) Preservation of privacy in data mining by using PCA based perturbation technique. In: International conference on smart technologies and management for computing, communication, controls, energy and materials (ICSTM), IEEE, pp 202–206
Zaman MM, Choudhury SR, Ahmed J, Talukder MH, Rahman AH (2016) Blood glucose and cholesterol levels in adult population of Bangladesh: results from STEPS 2006 survey. Indian Heart J 68(1):52–56
Jayawardena R, Ranasinghe P, Byrne NM, Soares MJ, Katulanda P, Hills AP (2012) Prevalence and trends of the diabetes epidemic in South Asia: a systematic review and metaanalysis. BMC Public Health 12:380
Hoque ME, Long KZ, Niessen LW, Al Mamun A (2015) Rapid shift toward overweight from double burden of underweight and overweight among Bangladeshi women: systematic review and pooled analysis. Nutr Rev 73:438–447
Balan EV, Priyan MK, Devi GU (2015) Hybrid architecture with misuse and anomaly detection techniques for wireless networks. In: International conference on communications and signal processing (ICCSP), IEEE, pp 185–189
Sundaramoorthy S, Shantharajah SP (2014) An improved ant colony algorithm for effective mining of frequent items. J Web Eng 13(3–4):263–276
Kumar PM, Gandhi UD (2017) A novel three-tier internet of things architecture with machine learning algorithm for early detection of heart diseases. Comput Electr Eng 65:222–235. https://doi.org/10.1016/j.compeleceng.2017.09.001
Suriya S, Deepalakshmi R, Kannan SS, Shantharajah SP (2012) Enhanced bee colony algorithm for complex optimization problems. Int J Comput Sci Eng 4(1):72
Priyan MK, Nath CG, Balan EV, Prabha KR, Jeyanthi R (2015) Desktop phishing attack detection and elimination using TSO program. In: International conference on smart technologies and management for computing, communication, controls, energy and materials (ICSTM), IEEE, pp 198–201
American Diabetes Association (2005) Diagnosis and classification of diabetes mellitus. Diabetes Care 28:S37–S42
Chobanian AV, Bakris GL, Black HR et al (2003) The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 289:2560–2572
Chandra I, Sivakumar N, Gokulnath CB, Parthasarathy P (2018) IoT based fall detection and ambient assisted system for the elderly. Clust Comput 1–9. https://doi.org/10.1007/s10586-018-2329-2
Brooks SP, Gelman A (1998) General methods for monitoring convergence of iterative simulations. J Comput Gr Stat 7:434–455
Rabe-Hesketh S, Skrondal A (2012) Multilevel and longitudinal modeling using state, 3rd edn. STATA Press, College Station
Schafer JL (1999) Multiple imputations: a primer. Stat Methods Med Res 8(1):3–15
Sterne JA, White IR, Carlin JB et al (2009) Multiple imputations for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 338:b2393
Balan EV, Priyan MK, Nath CG, Devi GU (2014) Efficient energy scheme for wireless sensor network application. In: IEEE international conference on computational intelligence and computing research (ICCIC), IEEE, pp 1–5
Perkins NJ, Schisterman EF (2006) The inconsistency of “optimal” cut points obtained using two criteria based on the receiver operating characteristic curve. Am J Epidemiol 163:670–675
Shera AS, Rafique G, Khawaja IA, Baqai S, King H (1999) Pakistan National Diabetes Survey: prevalence of glucose intolerance and associated factors in Baluchistan province. Diabetes Res Clin Pract 44:49–58
Kim SM, Lee JS, Lee J et al (2006) Prevalence of diabetes and impaired fasting glucose in Korea: Korean National Health and Nutrition Survey 2001. Diabetes Care 29:226–231
Kumar PM, Gandhi UD (2017) Enhanced DTLS with CoAP-based authentication scheme for the internet of things in healthcare application. J Supercomput 1–21. https://doi.org/10.1007/s11227-017-2169-5
Yang W, Lu J, Weng J et al (2010) Prevalence of diabetes among men and women in China. N Engl J Med 362:1090–1101
International Diabetes Federation (IDF) (2013) Diabetes atlas, 5th edn. http://www.idf.org/diabetesatlas/5e/the-globalburden. Accessed 7 June 2013
Zhang H, Xu W, Dahl A, Xu Z, Wang HX, Qi X (2013) Relation of socio-economic status to impaired fasting glucose and Type 2 diabetes: findings based on a large population-based cross-sectional study in Tianjin, China. Diabetes Med 30:e157–e162
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J (2005) Global burden of hypertension: analysis of worldwide data. Lancet 365:217–223
Janghorbani M, Amini M, Gouya MM, Delavari A, Alikhani S, Mahdavi A (2008) Nationwide survey of prevalence and risk factors of prehypertension and hypertension in Iranian adults. J Hypertens 26:419–426
Gokulnath CB, Shantharajah SP (2018) An optimized feature selection based on genetic approach and support vector machine for heart disease. Clust Comput 1–11. https://doi.org/10.1007/s10586-018-2416-4
Mayega RW, Makumbi F, Rutebemberwa E et al (2012) Modifiable socio-behavioral factors associated with overweight and hypertension among persons aged 35 to 60 years in Eastern Uganda. PLoS ONE 7:e47632
Padma T, Mir SA, Shantharajah SP (2017) Intelligent decision support system for an integrated pest management in Apple Orchard. In: Sangaiah A, Abraham A, Siarry P, Sheng M (eds) Intelligent decision support systems for sustainable computing. vol 705. Springer, Cham, pp 225–245
Cunningham-Myrie C, Younger-Coleman N, Tulloch-Reid M et al (2013) Diabetes mellitus in Jamaica: sex differences in burden, risk factors, awareness, treatment and control in a developing country. Trop Med Int Health 18:1365–1378
Islam FMA, Chakrabarti R, Islam MT et al (2016) Prediabetes, diagnosed and undiagnosed diabetes, their risk factors and association with knowledge of diabetes in rural Bangladesh: the Bangladesh population-based diabetes and eye study. J Diabetes 8:260–268
Uma S, Shantharajah SP, Rani C (2017) Passive incidental alertness—based link visualization for secure data transmission in manet. J Appl Secur Res 12(2):304–322
Cheong KC, Yusoff AF, Ghazali SM et al (2013) Optimal BMI cut-off values for predicting diabetes, hypertension and hypercholesterolemia in a multi-ethnic population. Public Health Nutria 16:453–459
Bhowmik B, Munir SB, Ahmed KR et al (2014) Anthropometric indices of obesity and type 2 diabetes in Bangladeshi population: Chandra Rural Diabetes Study (CRDS). Obes Res Clin Pract 8:e201–e298
Feng R-N, Zhao C, Wang C et al (2012) BMI is strongly associated with hypertension, and waist circumference is strongly associated with type 2 diabetes and dyslipidemia, in northern Chinese adults. J Epidemiol 22:317–323
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
This article has been retracted. Please see the retraction notice for more detail:https://doi.org/10.1007/s00521-024-10080-x
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chandra Babu, G., Shantharajah, S.P. RETRACTED ARTICLE: Optimal body mass index cutoff point for cardiovascular disease and high blood pressure. Neural Comput & Applic 31, 1585–1594 (2019). https://doi.org/10.1007/s00521-018-3484-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00521-018-3484-3