
Abstract
Purpose
(1) To determine, in women with breast cancer-related lymphedema (BCRL), the frequency, intensity and distress of body image and sexuality concerns. (2) To examine relationships between body image and sexuality concerns, and lymphedema, personal and cancer treatment factors.
Method
Women with BCRL (n = 64) completed the Lymphedema Symptom Intensity and Distress Scale – Arm (LSIDS-A), which focuses on the intensity and distress of a range of lymphedema symptoms. They also underwent a lymphedema assessment. Responses to eight questions from the LSIDS-A regarding sexuality, body image and intimate relationships were considered. Frequency of responses was tabulated. Multiple linear regressions were used to determine if specific factors were related to higher intensity and distress scores associated with body image and sexuality issues.
Results
Body image and sexuality concerns were common (48%, 23% respectively). Participants reported a range (0–10) of intensity and distress related to body image and sexuality symptoms. Univariate linear regression revealed greater intensity of sexuality concerns was associated with younger age, whilst distress related to sexuality concerns was associated with higher inter-arm bioimpedance ratio and shorter duration of lymphedema. Body image concerns were not related to any considered factors.
Conclusion
Body image and sexuality concerns are common, intense and distressing for patients with breast cancer lymphedema. Assessment of both the intensity and distressed caused by these symptoms is necessary to understand the impact of lymphedema.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer-related lymphedema (BCRL) is a common and feared, sequelae of breast cancer treatment. Lymphedema occurs when damage or dysfunction in the lymphatic system interferes with its ability to drain fluid from the interstitial space for return to the blood stream [1]. The accumulation of protein-rich fluid results in a chronic, persistent swelling [1]. It is estimated that 20% of women who undergo axillary lymph node dissection will develop upper limb lymphedema [2]. As BCRL is a lifelong condition, a focus on the long-term psychosocial effects for those affected is needed [3,4,5,6].
Following breast cancer treatment, women may experience disturbance in their body image and sexual functioning [7,8,9]. Body image can be defined as ‘a person’s perceptions, thoughts and feelings about his or her body’ [10]. Sexuality is a broad term encompassing engagement in sexual activity: sexual expression and orientation; sexual functioning; as well as attitudes towards sex and elements of intimacy, romance and relationships [11, 12]. However, for this study, sexuality is considered as engagement and interest in sexual activity. For breast cancer survivors who develop BCRL, additional concerns, such as feeling self-conscious about the appearance of the affected limb [3, 13], sentiments of the arm looking unattractive [14] and seeing it as a permanent, visible sign of disability [4], are also reported. Women with BCRL may report more challenges in sexual relationships than women without BCRL [15], which can be as a result of pain or swelling and feeling self-conscious, or treatment options such as compression garments hindering intimacy and spontaneity [14]. Furthermore, women with BCRL are also more likely to report poorer emotional and psychological wellbeing [5] and quality of life [6, 16] compared to breast cancer survivors without BCRL and have significantly poorer perceptions related to body image, appearance and sexuality [4]. Body image disturbance has been implicated in the development of depression, anxiety and stress in women with BCRL [17, 18], which can have a profound impact on quality of life, suggesting the need for adequate identification and support for those affected.
To date, however, no study has primarily aimed to determine the frequency of body image and sexuality concerns in women with BCRL. An understanding of whether there are any factors that may make patients more likely to be affected by these issues is also needed. Whilst limited previous research has investigated possible contributing factors to body image and sexuality concerns [6, 19, 20], the individual must also be considered within a wider context. Studies looking at specific factors related to poor psychological outcomes in women with BCRL tend to focus on outcome measures related to general quality of life [6] and distress [20], rather than outcomes specifically related to body image and sexuality. The primary aim of this study is, therefore, to determine, in women with BCRL, the frequency, intensity and distress associated with body image and sexuality concerns. A secondary aim is to determine whether these concerns are related to any specific personal, lymphedema or cancer treatment factors.
Methods
This is a secondary data analysis. Data was originally collected as part of a larger cross-sectional study on the detection of breast cancer-related lymphedema [21, 22] and was granted ethical approval by the Human Research Ethics Committee (HREC/09/HARBR/4; 0902-004 M) at each institution where the study was conducted. Written, informed consent was provided from each participant prior to participation. All collected data was stored in a deidentified manner, in a secure research data storage system.
Participants
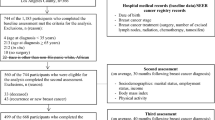
Participants were recruited over the period of 2009–2012 through open advertisement. All included had previously been diagnosed with, and treated for, upper limb lymphedema secondary to unilateral breast cancer, but had not received any active treatment, such as bandaging, within 3 months of inclusion in the study. For this analysis, participants were excluded if they were male, had a diagnosis other than breast cancer (e.g. melanoma), did not complete the Lymphedema Symptom Intensity and Distress Scale – Arm (LSIDS-A) questionnaire or did not undergo mastectomy or wide local excision breast surgery.
Assessments
Participants attended a single assessment session, where initial information regarding participant demographics, as well as breast cancer and lymphedema history, was collected. All participants underwent a number of physical tests, including bioimpedance spectroscopy (BIS) and circumference measurements, and completed a questionnaire regarding their lymphedema symptoms.
Lymphedema symptom intensity and distress scale – arm: LSIDS-A
Body image and sexuality concerns were captured through the Lymphedema Symptom Intensity and Distress Scale – Arm (LSIDS-A) questionnaire. The LSIDS-A is a 36-item questionnaire, developed to serve as a single assessment tool for evaluation of both physical and psychological symptoms in women with BCRL, and to act as a conduit for communication between the patient and healthcare provider [23]. Except for a question related to sexual activity, the LSIDS-A instructions ask the patient to reflect on their symptom experience over the past week. Participants then respond with ‘yes’, ‘no’ or for four questions related to sexual activity, ‘prefer not to answer’. The question specific to sexual activity asks the patient to reflect on whether the symptom had been present since developing lymphedema, rather than during the past week. If a participant answers ‘yes’ to a symptom, they then rate the intensity and distress of the symptom on separate visual analogue scales from 1, ‘slight’, to 10, ‘severe’. Intensity is described as the severity of the symptom itself, whilst distress encompasses the physical or emotional response to that symptom [24].
The instrument covers a range of lymphedema symptoms including physical, emotional, behavioural and social domains. In the current study, eight symptoms related to body image and sexuality were considered. They were analysed separately and were grouped into two clusters to assess overall body image and sexuality. These two clusters were informed by the clusters of symptoms identified in development of the questionnaire but modified to support the aims of the current study. ‘Body image’ comprised lack of confidence in self, concerns about looks, feeling less sexually attractive and loss of confidence in body, whereas ‘sexuality’ comprised lack of interest in sex and a decrease in sexual activity. Two additional questions concerning partner lack of interest in sex and feeling misunderstood by significant other were included in the individual question analysis but excluded from the body image and sexuality clusters as these two questions were about the impact of their disease on someone else. To be included in the analysis of each cluster, participants needed to respond ‘yes’ to at least one of the constituent symptoms. Each participant was given an overall intensity and distress score for the cluster by summing their scores for each symptom. For example, both intensity and distress for the ‘body image’ cluster were scored out of a maximum of 40.
The instrument has good reliability for the overall intensity (Cronbach’s alpha = 0.93) and distress (Cronbach’s alpha = 0.94) scores [23]. When compared to other breast cancer, lymphedema and quality of life questionnaires, such as the Functional Assessment of Cancer Therapy – Breast, Upper Limb Lymphoedema 27 and Marlowe-Crowne Social Desirability Scale, the LSIDS-A was found to have acceptable convergent and divergent validity [23].
Bioimpedance spectroscopy
Bioimpedance spectroscopy (BIS) was used to assess the extracellular fluid volume in the upper limbs of participants [25], using an SBF7 impedance spectrometer (Impedimed Ltd, Brisbane, Queensland, Australia), according to a standardised protocol described in previous studies [21, 22, 26]. Briefly, patients were positioned supine, with their arms by their sides, slightly abducted from their body. The skin was cleaned with an alcohol wipe prior to the application of Ag–AgCl gel electrodes, placed as per the manufacturer’s directions. To determine whole-arm impedance, defined as from the wrist to the axilla [26], electrodes were placed bilaterally just distal to the metacarpophalangeal joint on the third metacarpal, on the dorsal surface of the wrist in line with the ulnar styloid, and just distal to the metatarsophalangeal joints on the second and third metatarsals. Measurements were taken for the right arm, then the left. A software supplied by the manufacturers (Bioimp v5.2.4.0, Impedimed Ltd) was used to process all data files. Impedance for both arms was determined at zero resistance (R0). To compare the unaffected and affected limbs, the impedance of both is expressed as a ratio:
Circumference measurements
Circumference measurements were determined using perometry (1000 Juzo Perometer), according to a standardised protocol [21, 22, 27]. Briefly, participants were seated, with the arm to be measured abducted 90° from the body, the elbow fully extended, the palm facing downwards, and the thumb tucked into the hand, with the arm slightly stretched to reach the hand rest ensuring that the full length of the arm was measured. To ensure measurements began from the ulnar styloid, hand measurements were taken bilaterally, which were used to determine the 0 cm starting point [28]. Circumferences were determined in 10 cm increments, up to 40 cm distal to the ulna styloid using the Peroplus software. If the arm length was insufficient for a measurement to be taken at 40 cm, both limb measurements were taken at the maximum length available. Inter-limb circumference differences were determined at each level by subtracting the circumference of the unaffected arm from the affected arm:
The interlimb circumference difference at each increment was then compared to diagnostic threshold set at 2 standard deviations above normative values, which have been found to be both highly sensitive and specific in the diagnosis of lymphedema [22, 29]. Each participant was given a score from 0 to 5, reflecting how many arm segments were above diagnostic thresholds, indicating the extensiveness of their lymphedema.
Data analysis
For patient demographics, the mean and standard deviation (SD) were calculated for each continuous variable, such as age, height and weight. Frequencies were determined for each of the categorical variables. Response rates for each of the eight symptoms considered from the LSIDS-A were determined by calculating the proportion of the sample that answered ‘yes’ to the presence of the symptom. For questions with a ‘prefer not to answer’ option, the proportion of respondents was also calculated. For each individual intensity and distress scale, the mean, median and range were determined.
Univariate linear regression was used to determine the extent to which higher intensity and distress scores associated with body image and sexuality concerns can be explained by personal, lymphedema and cancer treatment factors [30]. Seven participants did not have complete circumference measurement data and excluded from the regression analysis. One participant was further excluded from the body image distress model, as they answered ‘yes’ to symptoms, but did not provide a distress score. Variables included in the analysis were age, body mass index (BMI), number of arm segments affected by lymphedema, BIS ratio, length of time with lymphedema, final breast surgery (mastectomy or wide local excision) and whether the dominant side was affected. All statistical analysis was completed in Microsoft Excel (Version 16.23) and SPSS (V27.0.1.0 IBM, Chicago, USA).
Results
Sixty-four participants were included in this analysis (Table 1). The average (SD) age for participants was 60.9 (10.0) years. The participants, on average, were slightly overweight, with a BMI of 26.5 (5.5), and 52% of the sample had lymphedema present in their dominant arm. The median number of arm segments affected by lymphedema was three out of a maximum of five.
Overall, 61% of participants reported the presence of at least one of the eight symptoms considered in this analysis (Table 2), with 31% of the sample reporting three or more symptoms. At least one body image concern was reported by 48% of the sample and 23% reported at least one sexuality concern. When the partner questions were removed, 22% of the sample reported the presence of three or more symptoms. When ‘prefer not to answer’ was a possible answer (four questions), it was selected by 16–30% of the sample, with 33% of the participants choosing ‘prefer not to answer’ for at least one question. Although overall average intensity and distress scores for most symptoms were similar, there was individual variability, with 17% of individual responses reporting greatly different intensity and distress scores (difference ≥ 3) in response to one symptom. Of these, 35% had distress scores at least 3 points higher than the intensity scores, and the remaining 65% reported higher intensity scores. Lack of confidence in self was the only symptom in which no participant scored distress as 10, whilst lack of confidence in body and lack of confidence in self were the only symptoms in which no participant reported an intensity score of 10.
Univariate linear regression assessed what factors predicted higher intensity and distress scores related to body image and sexuality concerns (Table 3). The intensity of sexuality concerns was related to younger age only. In contrast, distress caused by sexuality concerns was associated with shorter duration of lymphedema and higher bioimpedance inter-arm ratios. For body image symptoms, no significant factors were identified for either intensity or distress.
Discussion
Body image and sexuality concerns are common for women with BCRL. The majority of participants in this study reported at least one concern related to body image, sexuality or intimate relationships, and more than 20% reported three or more body image and sexuality concerns. Body image concerns were more common than sexuality concerns and these issues also appear to be notably intense and distressing. Regression analysis did not clarify which factors contribute to body image concerns. However, the analysis did show that younger age, extensiveness of lymphedema, duration of lymphedema and lymphedema in the dominant arm were significantly related to sexuality symptoms.
Significant variability in individual intensity and distress scores was seen in this study, giving weight to these two concepts being considered as different aspects of the patient experience. Intensity is defined as the severity of the symptom, whilst distress refers to the physical or emotional response to the symptom [31]. Although Ridner [23] originally suggested multiplying intensity and distress together to provide an overall ‘symptom burden’, they were considered separately in this study which was supported by our findings. Seventeen percent of all responses reported intensity and distress scores that differed by three points or more on a 10-point scale. A third of women reported a symptom being more distressing than its intensity, suggesting that assessing only the presence or intensity of a symptom will not fully capture the impact it has on the individual. To provide optimal support for women with BCRL, not only do body image and sexuality concerns need to be identified, but their impact on the individual should be considered.
The relationship found between symptoms associated with sexuality and lymphedema had mixed agreement with previous studies. For example, in contrast to some previous reports [20], but in agreement with others [14], we found a significant relationship between lymphedema severity and the distress associated with sexuality symptoms. Differences in these findings may relate to how the severity of lymphedema has been assessed. Perception of severity of arm swelling has previously been associated with psychosocial distress and sexuality concerns [14, 32]. Furthermore, in contrast to previous findings [19], we found that women who had lymphedema for shorter periods of time had greater sexuality concerns. This may reflect women becoming more accustomed to their lymphedema over time. However, in agreement with previous research [19], BMI was not found to be related to the intensity or distress of symptoms related to sexuality or body image. It is unclear whether the additional option of ‘prefer not to answer’ for the questions on sexuality impacted the findings in this study.
Explanatory factors for body image concerns were not identified in the current study, possibly reflecting how body image was captured or the sample size of this study. Women with BCRL report lymphedema as looking ‘ugly’ and being mistaken for body fat, rather than swelling, causing them to feel self-conscious in both intimate relationships and in public [14]. Whilst the LSIDS-A addresses some symptoms associated with body image concerns, it focuses on symptoms of negative body image. To more fully capture the complexity of body image, a suite of questionnaires on concepts such as body image disturbance, body satisfaction and body confidence may be needed [33]. Other qualitative studies into this area have reported factors that contribute to poor body image, including the comments and perceptions of others [13, 34], the use of compression garments [14, 15] and being treated as though disabled [14], which are not addressed in the LSIDS-A questionnaire.
The high number of ‘prefer not to answer’ responses in this study highlights the reluctance of patients to discuss their body image and sexuality concerns. Ridner et al. [19] reported ‘prefer not to answer’ or non-response of 6–15%, which were lower than in this study. Despite the reluctance for some to engage with these questions, support regarding body image and sexuality has been identified as an unmet need for breast cancer survivors [35], and there is dissatisfaction with the quality of care and advice received [36]. However, many women with BCRL choose only to discuss sexuality concerns with their partner [14], placing the partner in a position of having a significant influence over a woman’s thoughts in this area. A supportive and understanding partner can have a pivotal role in assisting women with BCRL to overcome sexual concerns [14] whereas inadequate partner support can have a significant impact on body image disturbance and issues with sexual functioning [10, 11, 37]. In the current study, the symptom ‘misunderstood by significant other’ had the highest average distress score. Clinicians should proactively assist in identifying body image and sexuality concerns. Patients report preferring to wait for the healthcare professional to initiate the discussion [38, 39], but also criticise these discussions for being prescriptive and rigid [40] and focusing too heavily on physical functioning, rather than emotional aspects [41]. There is also reluctance from clinicians to engage in these conversations [38]. They cite awkwardness and lack of confidence in the area as reasons for their hesitation [38, 39], resulting in women with BCRL rarely being asked about their body image and sexuality by their healthcare providers [14]. Although in this study, the group who chose ‘prefer not to answer’ for at least one question was slightly older on average (66 years) in comparison to those who did not select this as answer (58 years); this is likely not simply an issue of age. Lack of clinician attention regarding body image and sexuality has been identified as an issue in populations over 50, regardless of breast cancer or lymphedema diagnosis [9]. Better understanding the role of the partner and clinician, and greater clinician confidence and comfort, may be required to ensure better support and care for women with BCRL.
Whilst this study provides new insight into the prevalence, intensity and distress of body image and sexuality concerns in women with BCRL, there are opportunities for future research. To date, much of the research in this area, including the current study, are cross-sectional in design, with lower sample sizes. A properly powered longitudinal study, commencing from the onset of lymphedema, may provide more insight as to when body image and sexuality concerns are at their most severe and whether they fluctuate over time. Furthermore, as this is a secondary analysis of previously collected data, it would be worthwhile to determine the ongoing currency of the findings. However, as our findings are similar to older studies without evidence of improvements in care in this area, it would be unexpected if current findings would be different. In addition, exploration of factors that are likely to be associated with poor body image and sexuality within a longitudinal study may provide greater clarity regarding personal, lymphedema and cancer treatment factors, especially duration, all of which remain unclear.
Conclusion
Body image and sexuality concerns are common, intense and distressing in women with BCRL. Despite their prevalence, there are many factors that contribute to these concerns that are yet to be understood. Whilst associations between lymphedema extensiveness, younger age, lymphedema in the dominant arm and shorter duration of lymphedema were found with sexuality concerns, further research is warranted, particularly in terms of the factors contributing to body image concerns.
Data availability
Data not available.
Code availability
Not applicable.
References
Padera TP, Meijer EF, Munn LL (2016) The lymphatic system in disease processes and cancer progression. Annu Rev Biomed Eng 18:125–158
Disipio T, Rye S, Newman B, Hayes S (2013) Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol 14:500–515
Taghian NR, Miller CL, Jammallo LS, O’Toole J, Skolny MN (2014) Lymphedema following breast cancer treatment and impact on quality of life: a review. Crit Rev Oncol Hematol 92:227–234
Fu MR, Ridner SH, Hu SH, Stewart BR, Cormier JN, Armer JM (2013) Psychosocial impact of lymphedema: a systematic review of literature from 2004 to 2011. Psychooncology 22:1466–1484
Tsuchiya M, Takahashi M (2016) Psychosocial impact of lymphoedema after breast surgery. Curr Breast Cancer Rep 8:47–51
Chachaj A, Malyszczak K, Pyszel K, Lukas J, Tarkowski R, Pudelko M et al (2010) Physical and psychological impairments of women with upper limb lymphedema following breast cancer treatment. Psychooncology 19:299–305
Boquiren VM, Esplen MJ, Wong J, Toner B, Warner E, Malik N (2016) Sexual functioning in breast cancer survivors experiencing body image disturbance. Psychooncology 25:66–76
Fobair P, Stewart SL, Chang S, D’Onofrio C, Banks PJ, Bloom JR (2006) Body image and sexual problems in young women with breast cancer. Psychooncology 15:579–594
Bakht S, Najafi S (2010) Body image and sexual dysfunctions: comparison between breast cancer patients and healthy women. Procedia Soc Behav Sci 5:1493–1497
Grogan S (2016) Body image: understanding body dissatisfaction in men, women and children. Taylor & Francis, London
McAuliffe L, Bauer M, Nay R (2007) Barriers to the expression of sexuality in the older person: the role of the health professional. Int J Older People Nurs 2:69–75
Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ (2007) A study of sexuality and health among older adults in the United States. N Engl J Med 357:762–774
Ridner SH, Bonner CM, Deng J, Sinclair VG (2012) Voices from the shadows: living with lymphedema. Cancer Nurs 35:E18-26
Winch C, Sherman K, Koelmeyer L, Christiansen K, Mackie H, Boyages J (2015) Sexual concerns of women diagnosed with breast cancer-related lymphedema. Supportive Care in Cancer 23(12):3481–3491
Radina ME, Fu MR, Horstman L, Kang Y (2015) Breast cancer-related lymphedema and sexual experiences: a mixed-method comparison study. Psychooncology 24:1655–1662
Beaulac SM, McNair LA, Scott TE, LaMorte WW, Kavanah MT (2002) Lymphedema and quality of life in survivors of early-stage breast cancer. Arch Surg 137:1253–1257
Alcorso J, Sherman KA (2016) Factors associated with psychological distress in women with breast cancer-related lymphoedema. Psychooncology 25:865–872
Teo I, Novy DM, Chang DW, Cox MG, Fingeret MC (2015) Examining pain, body image, and depressive symptoms in patients with lymphedema secondary to breast cancer. Psychooncology 24:1377–1383
Ridner SH, Sinclair V, Deng J, Bonner CM, Kidd N, Dietrich MS (2012) Breast cancer survivors with lymphedema: glimpses of their daily lives. Clin J Oncol Nurs 16:609–614
Passik SD, Newman ML, Brennan M, Tunkel R (1995) Predictors of psychological distress, sexual dysfunction and physical functioning among women with upper extremity lymphedema related to breast cancer. Psychooncology 4:255–263
Dylke ES, Ward LC, Meerkin JD, Nery L, Kilbreath SL (2013) Tissue composition changes and secondary lymphedema. Lymphat Res Biol 11:211–218
Dylke ES, Schembri GP, Bailey DL, Bailey E, Ward LC, Refshauge K et al (2016) Diagnosis of upper limb lymphedema: development of an evidence-based approach. Acta oncologica (Stockholm, Sweden) 55:1477–1483
Ridner SH, Dietrich MS (2015) Development and validation of the lymphedema symptom and intensity survey-arm. Supportive care in cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 23:3103–3112
Stolldorf DP, Dietrich MS, Ridner SH (2016) A comparison of the quality of life in patients with primary and secondary lower limb lymphedema: a mixed-methods study. West J Nurs Res 38:1313–1334
Cornish BH, Chapman M, Hirst C, Mirolo B, Bunce IH, Ward LC et al (2001) Early diagnosis of lymphedema using multiple frequency bioimpedance. Lymphology 34:2–11
Ward LC, Dylke E, Czerniec S, Isenring E, Kilbreath SL (2011) Confirmation of the reference impedance ratios used for assessment of breast cancer-related lymphedema by bioelectrical impedance spectroscopy. Lymphat Res Biol 9:47–51
Stanton A, Northfield J, Holroyd B, Mortimer P, Levick J (1997) Validation of an optoelectronic limb volumeter (Perometer®). Lymphology 30:77–97
Czerniec SA, Ward LC, Refshauge KM, Beith J, Lee MJ, York S et al (2010) Assessment of breast cancer-related arm lymphedema—comparison of physical measurement methods and self-report. Cancer Invest 28:54–62
Dylke ES, Yee J, Ward LC, Foroughi N, Kilbreath SL (2012) Normative volume difference between the dominant and nondominant upper limbs in healthy older women. Lymphat Res Biol 10:182–188
Peat JK (2005) Medical statistics : a guide to data analysis and critical appraisal, 1st edn. Blackwell Pub, Malden, Mass
Stolldorf DP, Dietrich MS, Ridner SH (2016) Symptom frequency, intensity, and distress in patients with lower limb lymphedema. Lymphat Res Biol 14:78–87
Ridner SH (2009) The psycho-social impact of lymphedema. Lymphat Res Biol 7:109–112
Schroff H, Calogero R, Thompson JK (2009) Assement of body image. In: Allison DB, Baskin ML (eds) Handbook of assessment methods for eating behaviors and weight-related problems: measures, theory and research (2nd edition). Sage Publications, pp 115–136
Rhoten B, Radina M, Adair M, Sinclair V, Ridner S (2015) Hide and seek: body image-related issues for breast cancer survivors with lymphedema. J Womens Health Issues Care 4:1–7
Male DA, Fergus KD, Cullen K (2016) Sexual identity after breast cancer: sexuality, body image, and relationship repercussions. Curr Opin Support Palliat Care 10:66–74
Ussher JM, Perz J, Gilbert E (2013) Information needs associated with changes to sexual well-being after breast cancer. J Adv Nurs 69:327–337
Gilbert E, Ussher JM, Perz J (2010) Sexuality after breast cancer: a review. Maturitas 66:397–407
Krebs LU (2012) Sexual health during cancer treatment. Adv Exp Med Biol 732:61–76
Pinto AC (2013) Sexuality and breast cancer: prime time for young patients. J Thorac Dis 5(Suppl 1):S81–S86
Vieira EM, Santos DB, Santos MA, Giami A (2014) Experience of sexuality after breast cancer: a qualitative study with women in rehabilitation. Rev Lat Am Enfermagem 22:408–414
Halley MC, May SG, Rendle KA, Frosch DL, Kurian AW (2014) Beyond barriers: fundamental ‘disconnects’ underlying the treatment of breast cancer patients’ sexual health. Cult Health Sex 16:1169–1180
Acknowledgements
The authors would like to thank David Cantwell for his time, assistance and advice on the data analysis for this study.
Funding
This study was funded by a grant from Cancer Australia, obtained by SLK.
Author information
Authors and Affiliations
Contributions
Emma Hoyle: methodology, data analysis and writing original draft; Elizabeth Dylke: methodology, data collection, data analysis and writing—review and editing. Sharon Kilbreath: methodology, data collection and writing review and editing.
Corresponding author
Ethics declarations
Ethics approval
This study had appropriate ethical approval (Human Research Ethics Committee; HREC/09/HARBR/4; 0902-004 M).
Consent to participate
All participants provided written consent prior to participating in this study.
Consent for publication
No participants are identifiable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hoyle, E., Kilbreath, S. & Dylke, E. Body image and sexuality concerns in women with breast cancer-related lymphedema: a cross-sectional study. Support Care Cancer 30, 3917–3924 (2022). https://doi.org/10.1007/s00520-021-06751-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-021-06751-3