
Abstract
Purpose
Healthy lifestyles including maintaining a normal weight, consuming a healthy diet, and being physically active can improve prognosis and health-related quality of life (HRQoL) among cancer survivors. The largest proportion of cancer survivors are older adults (≥ 65 years), yet their lifestyle behaviors are understudied. This study sought to examine the lifestyle behaviors (maintaining healthy weight, diet quality, physical activity) of older female cancer survivors and identify associations with HRQoL.
Methods
Older female cancer survivors (n = 171) completed surveys to assess HRQoL (RAND-36), unintentional weight loss, body mass index (BMI), diet quality (HEI-2015), and physical activity. Demographic information and medical record data were also collected. Descriptive analyses, correlations, and stepwise linear regressions were utilized.
Results
Physical and mental HRQoL of the sample (mean age = 74.50 years) were low: 41.94 ± 10.50 and 48.47 ± 7.18, respectively, out of 100. Physical activity was low: 75.3%, 54.2%, and 68.1% reported no strenuous, moderate, and mild physical activity, respectively. Mean BMI was 27.71 ± 6.24 (overweight) with 64% of the participants being overweight or obese. Mean HEI-2015 scores were 66.54 ± 10.0. Engagement in moderate physical activity was associated with higher physical HRQoL (β = 0.42, p = 0.004). Being white (β = 0.53, p < 0.001), older (β = 0.27, p = 0.025), and having higher HEI scores (β = 0.30, p = 0.011) were associated with higher mental HRQoL.
Conclusions
Older cancer survivors report poor diet quality, high rates of being overweight or obese, and low levels of physical activity that impact their HRQoL. Results indicate the need for tailored health coaching for older cancer survivors regarding their lifestyle behaviors to improve prognosis and HRQoL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Older adults (age ≥ 65 years) account for more than 62% of the more than 16.9 million cancer survivors in the USA [1]. Due to the aging of the population, as well as advancements in screenings and treatment, the number of older cancer survivors will continue to grow [2]. Despite a majority demographic, there is limited research focusing on the older cancer survivor population, a heterogeneous group in terms of functional status and healthcare needs [2, 3]. Older cancer survivors are significantly more likely to report fair to poor health and have more chronic medical conditions and functional limitations than their cancer-free counterparts [4]. Both aging and status as a cancer survivor may increase the risk for chronic health conditions and worsen health-related quality of life (HRQoL) [5]. HRQoL is a multidimensional concept that quantifies the physical, psychological, and social aspects of health and their correlates, including health conditions, functional status, and socioeconomic status [6].
One strategy to improve HRQoL is through the adoption and maintenance of healthy lifestyle behaviors such as exercising, eating a balanced diet, not smoking, getting adequate sleep, limiting alcohol consumption, and reducing stress [7]. The National Comprehensive Cancer Network [8], American Society of Clinical Oncology [9], American Institute of Cancer Research [10], American Cancer Society [11], and the American College of Sports Medicine [12] have all provided guidelines regarding health behaviors and lifestyle behaviors for cancer survivors. Unfortunately, previous studies suggest that the majority of cancer survivors do not meet these current guidelines, contributing to the increased risk of negative outcomes including development of secondary cancers, cancer recurrence, and poor HRQoL [5, 13, 14].
Lifestyle behaviors among older female cancer survivors are an understudied area of research despite significant prognostic implications for treatment side effects, cancer-specific mortality, and overall survival [3]. Previous studies have indicated gender differences in health behaviors among older cancer survivors [15, 16]. For example, LeMasters [15] found that female cancer survivors are more likely to eat more fruits and vegetables and be of normal weight, yet less likely to meet physical activity recommendations. Furthermore, older women are of particular importance as they are typically in charge of meal planning and preparation and may have more control over dietary intake of the household compared with older men [17].
Although evidence has been accumulating only recently, several studies have found that lifestyle factors, such as normal body weight, physical activity, and healthy diet, are individually associated with better HRQoL [5, 14, 18]. The few studies that have focused on older female cancer survivors demonstrated that increased healthy lifestyle behaviors are associated with physical and mental HRQoL [16, 19]. However, these studies mainly focused on older breast cancer survivors, limiting its generalizability. In addition, studies focused on potential differences in nutritional intake and physical and psychological well-being by demographic factors, including age, race, and income, are missing.
An exploration of lifestyle factors including nutritional intake, physical activity, and weight, among older female cancer survivors, is warranted because they can be modified and are influenced by biological, social, and psychological variables. Thus, the biopsychosocial model [20] and the social determinants of health model [21] guide this current research. This study sought to examine the self-reported prevalence of lifestyle behaviors (maintaining healthy weight, dietary intake, physical activity) of older female cancer survivors. A second objective was to identify associations between lifestyle behaviors and physical and mental HRQoL among older female cancer survivors.
Methods
Participants
Eligible participants were female, aged 65 or older, who had received primary cancer treatment (i.e., chemotherapy, surgery, radiation) within the past 5 years, were community-dwelling, and able to complete a survey in English. Women with all cancer subtypes and stages, as well as women receiving maintenance therapy (i.e., hormonal therapy), were eligible to participate. Participants were excluded if they had a cancer diagnosis greater than 10 years prior to the time of study recruitment, in order to minimize recall bias regarding changes in health status since completion of cancer treatment.
Recruitment
Women who met the eligibility criteria were recruited through two primary methods. The first method was during follow-up visits to the [22] Geriatric Oncology Clinic. When prospective patients were identified, a physician study member provided the participant with a recruitment flyer, which had the study coordinator’s name and contact information. The second method involved the identification of prospective participants through medical records obtained from the cancer center’s registry. When patients were identified as meeting the eligibility criteria, the study coordinator was provided with the prospective participant’s name and mailing address. A recruitment letter explaining the survey was sent to the prospective participants asking them to contact the study coordinator if they were interested. Women who contacted the study coordinator were screened to verify that they met eligibility criteria. The study goals and responsibilities were explained and then participants were asked whether they were willing to participate. Eligible women who were interested in participating accessed the survey by the provided link to the Research Electronic Data Capture (REDCap) survey in the recruitment letter, or they requested the survey via mail or telephone. REDCap is a secure web application for building and managing online surveys and databases.
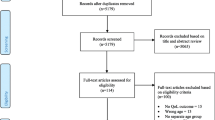
Of the 1200 women who met the eligibility criteria that were contacted for participation, 215 expressed interest in participating in the study. Forty-four women expressed interest but did not respond to subsequent follow-up attempts and 171 women completed survey measures. Thus, the response rate was 14.3%.
Informed consent, as well as a HIPAA (Health Insurance Portability and Accountability Act) waiver to collect basic demographic and clinical characteristics from their medical records, was obtained from all participants. All participants received a $10 gift card for their time. The Ohio State University Institutional Review Board approved the informed consent procedures and study protocol.
Measures
RAND-36: the 36-item health survey [23]
This 36-item survey is comprised of eight subscales assessing the following aspects of HRQoL: physical functioning, role functioning physical, pain, general health, energy/fatigue, social functioning, role functioning emotional, and emotional well-being. Responses to these items are on a 5-point Likert scale. Responses to the individual items are transformed during data analysis to a scale ranging from 0 to 100, with 100 being the highest subscale score for each of the 8 subscales [6, 23]. In addition, two composite scores can be created from the 8 subscales concerning physical (physical composite score (PCS)) and mental (mental composite score (MCS)) health concerns. For the purposes of this study, the PCS and MCS were used as measures of the participants’ physical and mental HRQoL, respectively [6, 23].
Healthy weight
Participant’s body mass index (BMI) was calculated from their reported height and weight in kg/m2. BMI was divided into 6 categories: underweight (< 18.5), normal weight (18.5 to < 25), overweight (25 to < 30), class 1 obese (30 to < 35), class 2 obese (35 to < 40), and extreme obesity (≥ 40) [24]. Unintentional weight loss was assessed using the yes/no question, “Have you recently lost weight without trying?” from the Malnutrition Screening Tool [25].
Diet History Questionnaire
The Diet History Questionnaire II (DHQ II) [26] is a food frequency questionnaire consisting of 134 food item questions and 8 dietary supplement questions. Questions inquire about dietary intake over the past 12 months and include questions about portion size and frequency, food preparation, alcohol intake, and special diet restrictions. Responses were imputed into Statistical Analysis Software in order to calculate Healthy Eating Index (HEI)-2015 scores. The HEI scoring software provides a score, which relates to quality of diet, from the diet information collected from the DHQ II. Total HEI score ranges from 0 to 100, with 100 being in complete compliance with the Dietary Guidelines for Americans [27]. HEI scores > 80 indicate a “good” diet, scores ranging from 51 to 80 reflect a diet that “needs improvement,” and HEI scores < 51 imply a “poor” diet [28].
Physical activity
Physical activity was measured by questions regarding the intensity of the exercise (strenuous, moderate, mild), frequency (none, 2, 3, 4, 5, or more days a week), and duration (< 20, 20–39, 40–59, ≥ 1 h). Physical activity questions are from the Personal Habits Questionnaire (Form 35) utilized in the Women’s Health Initiative Clinical Trial and Observational Study [29].
Social support
Social support was measured by the 8-item Modified Medical Outcomes Study Social Support Survey (mMOS-SS) [30]. The score for mMOS-SS was calculated as the average score of subscale items transformed to a 0–100 scale, with higher scores indicating more support. The mMOS-SS is scored on a 5-point scale and has two subscale measures of emotional or instrumental support.
Demographic and clinical variables
Participants provided self-reported demographic information, including age, gender, race, ethnicity, education, employment status, and household income. Clinical information regarding cancer diagnosis, American Joint Committee on Cancer (AJCC) stage at diagnosis, time since diagnosis, and number of chronic conditions was obtained through medical record review.
Data analysis
Descriptive statistics were used for the demographic and health characteristics, HEI-2015 total score and subcomponent scores, and physical activity. DHQ II scores were converted to the HEI-2015 scores, per guidelines from the National Cancer Institute, utilizing SAS 24 and Diet*Calc [31]. A series of t tests and ANCOVAs with Bonferroni post hoc analyses were utilized for multiple comparisons of the mean PCS and MCS by demographic and clinical characteristics as well as lifestyle behaviors. Pearson’s and Spearman’s correlations were used to assess potential associations among PCS, MCS, lifestyle behaviors, demographic and clinical characteristics, and social support. Chi-square analyses were used to determine significant relationships between cancer type (breast/non-breast) and participation in strenuous, moderate, and mild exercise (yes/no). Stepwise linear regressions were conducted to assess potential associations between PCS, MCS, HEI total score, physical activity (mild, moderate, vigorous), and healthy weight (BMI, unintentional weight loss), while controlling for demographic (age, race, education, marital status, employment) and clinical (cancer type, AJCC stage, time since diagnosis, number of chronic conditions) characteristics, and instrumental and emotional social support. IBM SPSS Statistics version 25.0 was used.
Results
Older female cancer survivors (n = 171) completed a one-time survey that assessed their HRQoL, diet quality, physical activity, and weight. Eighty-nine (52%) participants completed paper-based surveys, 80 (46.8%) completed REDCap surveys, and 2 (1.2%) completed telephone surveys. The majority of the sample (median age = 74.50 ± 8.43 years) were white (90%), married (54.7%), breast cancer survivors (67.7%), and completed at least a bachelor’s degree (54.7%). Other cancer types included hematologic (13.5%) and gynecologic (12%) cancers. Self-reported health was mostly very good (42.4%) and good (40%) (Table 1).
HRQoL
Table 2 shows the HRQoL results for older female cancer survivors. Average PCS and MCS were 41.94 ± 10.50 and 48.47 ± 7.18, respectively, out of 100. The social functioning subscale was the highest, with an average of 82.50. The energy/fatigue subscale was the lowest with an average of 42.74. Potential differences in mean PCS and MCS were examined related to sample’s demographic and clinical characteristics and lifestyle behaviors (Table 3). Participants with the lowest PCS and MCS were disabled/unemployed, single/never married, and/or had low incomes and low total HEI scores.
Older female cancer survivors who were married, a normal weight, had higher incomes, no unintentional weight loss, higher HEI total scores, and engaged in strenuous and/or moderate exercise had significantly higher mean PCS. Older female cancer survivors who had at least a college degree, were retired, and had no unintentional weight loss had significantly higher mean MCS.
Healthy weight
Median participant BMI was 26.54 ± 6.22 kg/m2 (overweight). Sixty-four percent of the participants had a BMI higher than 25, which is categorized as being overweight (31%) or obese (33.7%). Twenty-six percent of the sample reported recent unintentional weight loss (Table 1).
Dietary intake
Participants had a mean HEI-2015 score of 66.54 ± 10.0 out of 100; scores ranged from 34.6 to 89.8. This was influenced by a high consumption of total vegetables, whole fruits, total protein foods, seafood and plant proteins, low consumption of whole grains, and high consumption of saturated fat. Table 4 describes the mean HEI-2015 scores in each component for the study sample.
Physical activity
Participants’ self-reported physical activity was low: 75.3%, 54.2%, and 68.1% of the participants reported no strenuous, moderate, and mild physical activity, respectively (Fig. 1). Sixteen (9.3%) participants reported engagement in mild, moderate, and strenuous activity, 40 (23.4%) participants reported only mild and moderate exercise, and 35 (20.5%) participants reported only strenuous and moderate exercise. Among the 45 participants reporting strenuous activity, the most common durations were 20–39 min (n = 17, 37.8%) and 40–59 min (n = 17, 37.8%). Among the 80 participants who reported moderate activity, 35 (43.8%) and 23 (28.8%) participants exercised moderately for 20–39 min and 40–59 min, respectively. Among the 51 participants who reported mild activity, the most common (41.2%) duration was 20–39 min.

Frequency of self-reported physical activity among older female cancer survivors
Participation in physical activity did differ by cancer type. Participants with a history of breast cancer participated in strenuous exercise more often than participants with other reported cancers (hematologic, gynecologic, other) (n = 31 vs. n = 15, χ2 = 5.50, p = 0.025). Similarly, participants with a history of breast cancer participated in moderate exercise more often than participants with other reported cancers (n = 49 vs. n = 31, χ2 = 4.48, p = 0.046).
Correlations
Being married (r = 0.20, p = 0.02), college educated (r = 0.19, p = 0.03), and having higher emotional social support (r = 0.303, p < 0.001) were positively associated with higher physical HRQoL. Physical HRQoL was positively correlated with engaging in strenuous (r = 0.31, p < 0.001) and moderate physical activity (r = 0.35, p < 0.001), as well as lower BMI (r = − 0.34, p < 0.001), no unintentional weight loss (r = 0.191, p = 0.027), and higher total HEI score (r = 0.34, p < 0.001).
Higher mental HRQoL was positively associated with older age (r = 0.29, p = 0.004), being college educated (r = − 0.22, p = 0.012), and being retired (r = − 0.21, p = 0.012). Higher total HEI scores (r = 0.171, p = 0.044) and no unintentional weight loss (r = 0.26, p = 0.002), as well as higher instrumental (r = 0.20, p = 0.019) and emotional (r = 0.29, p = 0.001) social support, were positively associated with higher mental HRQoL.
Regressions
Stepwise linear regressions were used to determine the associations between lifestyle behaviors (maintaining healthy weight, dietary intake, physical activity) and physical (PCS) and mental (MCS) HRQoL. Controlling for demographic and clinical factors, engagement in moderate physical activity was associated with higher physical HRQoL (β = 0.42, p = 0.004; Model: F = 9.51, p = 0.004). Being white (β = 0.53, p < 0.001), older (β = 0.27, p = 0.025), and having higher HEI scores (β = 0.30, p = 0.011) was associated with higher mental HRQoL (Model: F = 11.50, p < 0.001).
Discussion
This study sought to examine the lifestyle behaviors (maintaining healthy weight, dietary intake, physical activity) of older female cancer survivors and to identify associations with physical and mental HRQoL. Results indicated multiple challenges in the healthy lifestyles of older cancer survivors. Older female cancer survivors in this study had low physical and mental HRQoL, low physical activity, and were overweight. Furthermore, poor diet quality, high rates of being overweight or obese, and low levels of physical activity impacted their HRQoL.
In this study, the mean PCS (41.94) and MCS (48.47) scores coincided with previously reported ranges (40.2–45.2 and 47.6–54.0, respectively) among older female cancer survivors [5, 18]. In comparison, results indicated that both the PCS and MCS of older female cancer survivors were below the average for older adults in the USA. PCS and MCS scores were lowest among participants who were disabled/unemployed, single/never married, and/or had low incomes and low total HEI scores [32]. These differences of both demographic and lifestyle behaviors indicate that there may be sub-groups of older female cancer survivors who are particularly vulnerable to non-adherence to healthy lifestyle behaviors, particularly older female cancer survivors of a lower socioeconomic status. The vulnerability of older cancer survivors becomes further apparent considering the influence of the secondary effects of cancer treatment on the evolution of the cancer survivor’s health behaviors and risk of cancer recurrence in the future. Additionally, due to the variety of quality of life measures (i.e., FACT-B; EQ-5D; PROMIS), it is difficult to compare HRQoL among older female cancer survivors. Future research may consider utilizing measures that are specifically designed to capture dimensions of HRQoL that are unique to older cancer survivors [33].
The study findings indicated that there is room for improvement regarding lifestyle behaviors among older female cancer survivors. Nearly 70% of participants reported no mild exercise and were overweight/obese. Similar findings have been observed among older cancer survivors [13, 34,34,36]. For example, Gjerset and colleagues found that 62% of older cancer survivors were physically inactive [35]. Similarly, Tarasenko and colleagues [36] found that 57.5% of young-old (65–74 years) and 60.5% of old-old (≥ 75 years) cancer survivors did not engage in sufficient levels of physical activity. Studies of older cancer survivors have reported similar prevalence of being overweight or obese ranging from 61 to 83% [34, 37, 38]. The total HEI-2015 score of participants in this study was 66.4 out of 100, in the diet “needs improvement” category. From 2015–2016 NHANES data, the average HEI-2015 score of older adults was 64 [39]. Furthermore, a study by Lee et al. using 2005–2016 NHANES data found the average HEI-2015 score for older cancer survivors was 54.9 [40]. The slightly higher HEI-2015 score in this study could be explained by the majority of participants being white and highly educated, characteristics that have previously been associated with higher HEI scores [41]. Improvement in these lifestyle behaviors can lead to increased HRQoL. Coinciding with the literature [5, 13, 16], women who engaged in lifestyle behaviors of maintaining a healthy weight, exercise, and healthy diet had higher PCS and MCS.
After accounting for demographic characteristics, health factors, and lifestyle behaviors, engagement in moderate physical activity was associated with physical HRQoL. Evidence suggests that physical activity, even among older, sedentary cancer survivors, can improve HRQoL, particularly physical HRQoL [13, 18]. A potential reason for this association is related to functional capacity. Scarabottolo [42] found that older adults who were physically active were 77% more likely to have better scores in functional capacity. Physical activity can improve cardiopulmonary function, muscle strength, and, ultimately, physical HRQoL among older cancer survivors. Despite its benefits [43], the promotion of physical activity from healthcare providers remains less than optimal among older cancer survivors [44]. Furthermore, older female cancer survivors may be less likely to engage in physical activity due to lifelong gender roles [15, 16]. Designing physical activity interventions tailored to the older adult’s capabilities, goals, and needs, as well as facilitators and barriers, is warranted [45]. These specific strategies will facilitate the long-term adherence of physical activity among older female cancer survivors.
Higher total HEI scores were predictive of higher mental HRQoL, corresponding with the literature. Evidence on positive effects from healthy eating on mental health-related outcomes among cancer survivors is growing [16, 46]. However, there is a paucity of studies focused on dietary quality and its associations among older female cancer survivors. Examination of dietary intake, using validated assessments, as well as utilizing registered dietitian nutritionists (RDNs), is desperately needed among this population [47]. Malnutrition is a prevalent complication of cancer and a risk factor for adverse outcomes, such as reduced survival and impaired quality of life, among older cancer survivors [48]. Reasons for older cancer survivors not following dietary recommendations include lack of knowledge, motivational and structural barriers (i.e., lack of access to healthy food), and geriatric factors (e.g., taste changes, xerostomia) [3, 47]. There is tremendous potential for dietary interventions lead by RDNs to promote optimal physical and mental health in older cancer survivors.
In the current study, race was significantly associated with HRQoL, even after controlling for demographic, health, and lifestyle variables. This association has been established within the literature, where older Black adults with cancer consistently report lower mental HRQoL [49]. Potential multi-level (i.e., system-, provider-level) factors that may negatively impact mental HRQoL were not explored in the current study. Future research should develop culturally sensitive interventions to improve survivorship outcomes, including HRQoL, among older Black cancer survivors.
Increased age was also positively associated with mental HRQoL. The majority of studies among the general older adult population suggest that older age is associated with better HRQoL [46, 50]. Older cancer survivors have comparable mental HRQoL compared with older adults of the same age without cancer [13, 18, 19]. For older adults with and without a history of cancer, HRQoL may reflect a general sense of well-being and life satisfaction rather than physical functioning [46, 50]. These findings are supported by the Socioemotional Selectivity Theory and resilient aging, which posit that older adults tend to provide more positive evaluations of their lives and emotional states, while adjusting to changes of physical health and other adverse life events [50, 51]. This positivity effect that comes with age may have influenced the reported mental HRQoL of this sample.
Interventions may be more effective in improving HRQoL among cancer survivors if they address multiple health behaviors [52]. Previous multi-health behavior interventions [7, 16] (e.g., exercise, diet quality, and modest weight loss) among older long-term cancer survivors resulted in clinically meaningful improvements in HRQoL. Utilization of informal (e.g., family, friends) and formal (e.g., primary care physicians, health coaches) sources of support and information can serve as motivators for older cancer survivors to adopt healthier lifestyles, in hopes of improving overall health and HRQoL.
Limitations
This study was cross-sectional and did not evaluate changes in HRQoL and lifestyle behaviors over the course of cancer treatment or recovery. Although this study adjusted for demographic and clinical variables, there may be unmeasured variables (e.g., health literacy) that impact the association between lifestyle behaviors and HRQoL. The data were collected via self-report, which can lead to inaccurate information. A study limitation is that duration of physical activity was measured by range; thus, specific metabolic equivalents (METs) and adherence to the current guidelines of physical activity based on minutes could not be calculated. Results from the DHQ II can underestimate fiber and whole grain content in one’s diet due to the lack of questions regarding whole grain products, as well as the misunderstanding of “whole grain” vs. “whole wheat” on product labels. Another limitation is the small sample size and limited demographic variability of this study. Participants were recruited from one cancer center, and the majority were white breast cancer survivors, which limits generalizability.
Conclusion
This study identified key health behavior (maintaining healthy weight, diet quality, and physical activity) vulnerabilities of older female cancer survivors. Specifically, participants were, on average, overweight, had suboptimal diet quality, and did not engage in adequate physical activity. Furthermore, the physical and mental HRQoL of this sample was lower than that of older adults who were not cancer survivors. Lower physical and mental HRQoL was associated with both demographic (age, race) and lifestyle characteristics (diet quality, physical activity). These findings can inform the development of tailored health behavior interventions to support the unique health and wellness needs of older female cancer survivors.
Data availability
Available for review upon request.
References
Siegel RL, Miller KD, Jemal A (2020) Cancer statistics, 2020. CA: A Cancer J Clin 70(1):7–30
Bluethmann SM, Mariotto AB, Rowland JH (2016) Anticipating the “silver tsunami”: prevalence trajectories and comorbidity burden among older cancer survivors in the United States. AACR
Presley CJ, Dotan E, Soto-Perez-de-Celis E, Jatoi A, Mohile SG, Won E et al (2016) Gaps in nutritional research among older adults with cancer. J Geriatr Oncol. 7(4):281–292
Rao AV, Demark-Wahnefried W (2006) The older cancer survivor. Crit Rev Oncol/Hematol. 60(2):131–143
Inoue-Choi M, Lazovich D, Prizment AE, Robien K (2013) Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention is associated with better health-related quality of life among elderly female cancer survivors. J Clin Oncol 31(14):1758–1766
Ware JE, Kosinski M, Keller SD, Kosinski M, Keller S, Ware J et al (1994) SF-36 physical and mental health summary scales: a user’s manual
Pekmezi DW, Demark-Wahnefried W (2011) Updated evidence in support of diet and exercise interventions in cancer survivors. Acta Oncol 50(2):167–178
Network NCC (2015) NCCN clinical practice guidelines in oncology: survivorship. NCCN, Fort Washington
American Society of Clinical Oncology. American Society of Clinical Oncology Clinical Practice Survivorship Guidelines and Adaptations. Am Soc Clin Oncol
World Cancer Research Fund International/American Institute for Cancer Research (2018) Diet, nutrition, physical activity and cancer: a global perspective: a summary of the third expert report. World Cancer Research Fund International, London
Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, Schwartz AL et al (2012) Nutrition and physical activity guidelines for cancer survivors. CA: Cancer J Clin 62(4):242–274
Campbell KL, Winters-Stone KM, Wiskemann J, May AM, Schwartz AL, Courneya KS et al (2019) Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc. 51(11):2375–2390
Blair CK, Robien K, Inoue-Choi M, Rahn W, Lazovich D (2016) Physical inactivity and risk of poor quality of life among elderly cancer survivors compared to women without cancer: the Iowa Women’s Health Study. J Cancer Survivorship. 10(1):103–112
Koh D, Song S, Moon S-E, Jung S-Y, Lee ES, Kim Z et al (2924) Adherence to the American Cancer Society guidelines for cancer survivors and health-related quality of life among breast cancer survivors. Nutrients. 11(12):2019
LeMasters TJ, Madhavan SS, Sambamoorthi U, Kurian S (2014) Health behaviors among breast, prostate, and colorectal cancer survivors: a US population-based case-control study, with comparisons by cancer type and gender. J Cancer Survivorship 8(3):336–348
Mosher CE, Sloane R, Morey MC, Snyder DC, Cohen HJ, Miller PE et al (2009) Associations between lifestyle factors and quality of life among older long-term breast, prostate, and colorectal cancer survivors. Cancer. 115(17):4001–4009
Flagg LA, Sen B, Kilgore M, Locher JL (2014) The influence of gender, age, education and household size on meal preparation and food shopping responsibilities. Public Health Nutr. 17(9):2061–2070
Pisu M, Azuero A, Halilova KI, Williams CP, Kenzik KM, Kvale EA et al (2018) Most impactful factors on the health-related quality of life of a geriatric population with cancer. Cancer. 124(3):596–605
Kent EE, Ambs A, Mitchell SA, Clauser SB, Smith AW, Hays RD (2015) Health-related quality of life in older adult survivors of selected cancers: data from the SEER-MHOS linkage. Cancer. 121(5):758–765
Engel GL (1977) The need for a new medical model: a challenge for biomedicine. Science. 196(4286):129–136
Wilkinson RG, Marmot M (2003) Social determinants of health: the solid facts. World Health Organization, Copenhagen
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform. 42(2):377–81
Hays RD, Sherbourne CD, Mazel RM (1993) The rand 36-item health survey 1.0. Health economics. 2(3):217–227
Centers for Disease Control (2018) About adult BMI—healthy weight—CDC
Ferguson M, Capra S, Bauer J, Banks M (1999) Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition. 15(6):458–464
National Institutes of Health (2010) Epidemiology and Genomics Research Program. National Cancer Institute. Diet History Questionnaire, version 2.0 (DHQ-II). SNAP Education Connection. Contract No.: April 19, 2020
U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015-2020 dietary guidelines for Americans, 8th Edition December 2015. Available from: https://health.gov/dietaryguidelines/2015/guidelines. Accessed 1 Jun 2020
Bowman SA, Lino M, Gerrior SA, Basiotis PP (1998) In: US Department of Agriculture, Center for Nutrition Policy and Promotion CNPP-5 (ed) The Healthy Eating Index: 1994-1996, Washington, DC
Design of the Women’s Health Initiative clinical trial and observational study (1998) The Women’s Health Initiative Study Group. Control Clin Trials. 19(1):61–109
Moser A, Stuck AE, Silliman RA, Ganz PA, Clough-Gorr KM (2012) The eight-item modified Medical Outcomes Study Social Support Survey: psychometric evaluation showed excellent performance. J Clin Epidemiol. 65(10):1107–1116
EGRP/DCCPS/NCI/NIH. SAS Code
Mielck A, Vogelmann M, Leidl R (2014) Health-related quality of life and socioeconomic status: inequalities among adults with a chronic disease. Health Qual Life Outcomes. 12(1):58
Fitzsimmons D, Gilbert J, Howse F, Young T, Arrarras J-I, Brédart A et al (2009) A systematic review of the use and validation of health-related quality of life instruments in older cancer patients. Eur J Cancer. 45(1):19–32
Maliniak ML, Patel AV, McCullough ML, Campbell PT, Leach CR, Gapstur SM et al (2018) Obesity, physical activity, and breast cancer survival among older breast cancer survivors in the Cancer Prevention Study-II Nutrition Cohort. Breast Cancer Res Treat. 167(1):133–145
Gjerset GM, Fosså SD, Courneya KS, Skovlund E, Thorsen L (2011) Exercise behavior in cancer survivors and associated factors. J Cancer Survivorship. 5(1):35–43
Tarasenko Y, Chen C, Schoenberg N (2017) Self-reported physical activity levels of older cancer survivors: results from the 2014 National Health Interview Survey. J Am Geriatr Soc. 65(2):e39–e44
Bluethmann SM, Foo W, Winkels RM, Mama SK, Schmitz KH (2019) Physical activity in older cancer survivors: what role do multimorbidity and perceived disability play? J Aging Phys Act. 1(aop):1–9
Forsythe LP, Alfano CM, George SM, McTiernan A, Baumgartner KB, Bernstein L et al (2013) Pain in long-term breast cancer survivors: the role of body mass index, physical activity, and sedentary behavior. Breast Cancer Res Treat. 137(2):617–630
US Department of Agriculture Food and Nutrition Service. Healthy Eating Index (HEI) | USDA-FNS [October 6, 2019]. Available from: https://www.fns.usda.gov/resource/healthy-eating-index-hei
Lee E, Hines R, Schulz V, Rovito M, Garcia J (2019) Diet quality in a nationally representative sample of American adult cancer survivors (P05-028-19). Curr Dev Nutr 3(Suppl 1)
Hiza HA, Casavale KO, Guenther PM, Davis CA (2013) Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J Acad Nutr Diet. 113(2):297–306
Scarabottolo CC, Cyrino ES, Nakamura PM, Tebar WR, da Silva Canhin D, Gobbo LA et al (2019) Relationship of different domains of physical activity practice with health-related quality of life among community-dwelling older people: a cross-sectional study. BMJ open. 9(6):e027751
Garcia DO, Thomson CA (2014) Physical activity and cancer survivorship. Nutr Clin Pract. 29(6):768–779
Halilova KI, Pisu M, Azuero A, Williams CP, Kenzik KM, Williams GR et al (2019) Healthy lifestyle discussions between healthcare providers and older cancer survivors: Data from 12 cancer centers in the Southeastern United States. Cancer Med. 8(16):7123–7132
Overholser LS, Callaway C (2018) Preventive health in cancer survivors: what should we be recommending? J Natl Compr Cancer Netw. 16(10):1251–1258
Cohrdes C, Mensink GB, Hölling H (2018) How you live is how you feel? Positive associations between different lifestyle factors, cognitive functioning, and health-related quality of life across adulthood. Qual Life Res. 27(12):3281–3292
Trujillo EB, Claghorn K, Dixon SW, Hill EB, Braun A, Lipinski E et al (2019) Inadequate nutrition coverage in outpatient cancer centers: results of a national survey. J Oncol 2019:7462940
Zhang X, Tang T, Pang L, Sharma SV, Li R, Nyitray AG et al (2019) Malnutrition and overall survival in older adults with cancer: a systematic review and meta-analysis. J Geriatr Oncol. 10(6):874–883
Pergolotti M, Deal AM, Williams GR, Bryant AL, Bensen JT, Muss HB et al (2017) Activities, function, and health-related quality of life (HRQOL) of older adults with cancer. J Geriatr Oncol. 8(4):249–254
Chopik WJ, Newton NJ, Ryan LH, Kashdan TB, Jarden AJ (2019) Gratitude across the life span: age differences and links to subjective well-being. J Posit Psychol. 14(3):292–302
Carstensen LL, Mikels JA (2005) At the intersection of emotion and cognition: aging and the positivity effect. Curr Dir Psychol Sci. 14(3):117–121
Prochaska JJ, Spring B, Nigg CR (2008) Multiple health behavior change research: an introduction and overview. Prev Med. 46(3):181–188
Funding
This study was partially funded by the Ohio State University Comprehensive Cancer and Aging Program.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jessica L. Krok-Schoen, Janell Pisegna, and Christian Stephens. The first draft of the manuscript was written by Jessica L. Krok-Schoen and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Krok-Schoen, J.L., Pisegna, J., Arthur, E. et al. Prevalence of lifestyle behaviors and associations with health-related quality of life among older female cancer survivors. Support Care Cancer 29, 3049–3059 (2021). https://doi.org/10.1007/s00520-020-05812-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-020-05812-3