
Abstract
Background
Religious/spiritual factors are important for some individuals in the context of life stress. To the authors’ knowledge, the present study is the first to explore the role of women’s attachment to God (anxious vs secure) in their adjustment to breast cancer.
Objective
To explore the (1) pattern of change in women’s attachment to God across time and (2) relationship between attachment to God and coping behaviors and depression.
Methods
All English-speaking women who were scheduled to receive a core breast biopsy at a women’s breast health center were eligible to participate in the study. Women were assessed on attachment to God, positive and negative coping, and depression at pre-diagnosis and 3, 6, and 12 months post-diagnosis. Women who received a benign diagnosis and those with a diagnosis of breast cancer participated in the study.
Results
Attachment to God remained stable across time for both diagnostic groups (cancer, benign). Women from both groups who had a more anxious attachment to God utilized more avoidance coping and reported more depression at different points across time. Breast cancer patients with a more anxious attachment to God reported engaging in less acceptance coping post-diagnosis. Finally, the association between attachment to God and depression was partially mediated by avoidance coping at pre-diagnosis.
Conclusions
Findings indicate that a more anxious attachment to God may contribute to negative patterns of adjustment while a secure attachment may help women remain more directly engaged in their coping with the threat of breast cancer and related diagnostic procedures.
Implications for practice
It is suggested that clinicians remain sensitive to and assess the role of spiritual beliefs in women’s adjustment to the threat of breast cancer from pre-diagnosis up to 1 year post-diagnosis. In particular, women’s belief in and experience of a secure or an anxious attachment with God or higher power may function as a potential resource or as an exacerbating factor, respectively, in their adjustment to breast cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Literature review
While studies have shown that breast cancer and its treatments can negatively impact women’s psychological well-being [1], research has also highlighted the role of personal and social resources in mitigating this impact. Evidence suggests that women who have various resources are better able to adapt to the demands of breast cancer [2]. Specifically, research shows that some individuals rely on religious/spiritual factors when confronted with stressors [3, 4] such as breast cancer [5]. For example, breast cancer patients who have a positive sense of God (i.e., loving) report better adjustment to the demands of diagnosis, treatment, and survivorship [6], a finding that is consistent across cultures and nationalities [7,8,9].
There is also the possibility however that the threat of breast cancer may erode a woman’s faith in a higher power, potentially contributing to poorer coping, mental health, and well-being [10, 11]. In a British study, breast cancer patients who held a negative sense of God (i.e., angry) reported higher levels of anxious and depressed mood [12] while a Canadian study revealed that women’s depressed mood increased across time the more they believed that their cancer was due to God’s anger/punishment [13]. Left unresolved, a negative sense of God can have serious implications for psychological well-being over the long-term [14]. Thus, an individual’s beliefs about God can become a liability rather than a resource in the context of coping with stress [4].
From a theoretical perspective, researchers [15, 16] have argued for the adoption of Bowlby’s attachment theory as a framework from which to understand the link between religion/spirituality and psychological well-being. According to this theory, attachment styles that develop in childhood are believed to be remained stable into adulthood and to become activated at times of stress [17] with a secure attachment style contributing to an individual’s resiliency in coping and adjustment [18]. Secure adult attachment has been linked to adjustment to health events such as diabetes [19], pregnancy [20], and abortion [21]. Conversely, researchers found that anxious or insecure adult attachment was linked to negative event appraisals [22] and maladaptive coping strategies (e.g., avoidance) [23], respectively. Notably, studies have shown that regardless of their adult attachment style (i.e., secure or insecure), some individuals turn to religion and/or God when faced with stress [24]; however, securely attached individuals rely more on positive forms of religious coping while insecurely attached individuals use more negative religious coping strategies [25, 26]. Such findings demonstrate a link between adult attachment styles and religious/spiritual beliefs.
In turn, for some individuals, God may function as another attachment figure or caregiver in providing security and comfort [15] contributing to greater well-being (e.g., positive affect) in general [27] and at times of significant stress [16]. For example, bereaved individuals with a secure attachment to God reported less depressive and grief symptoms and greater stress-related growth [28]. In contrast, insecure attachment to God has been related to greater feelings of emotional distress and decreased life satisfaction in general [29]. Other studies [30,31,32] similarly reported an association between insecure attachment to God and greater emotional distress and that, specifically, a more anxious attachment to God predicted levels of perceived stress beyond the contribution of adult attachment style [33].
Although attachment to God has been investigated in relation to general psychosocial well-being and religious/spiritual coping, few studies have explored the link between attachment to God and general (i.e., non-religious/spiritual) coping behavior within the context of significant life stress. To fully understand the role of spirituality in coping with illness, it is important to study how it functions within the context of other adjustment factors including general cognitive appraisal and coping behavior [34]. One recent study [35] explored the importance of an attachment to God for cancer and dialysis patients. Findings illustrated that individuals who had a secure attachment to God adopted a fighting spirit in coping with their illness whereas those with an insecure attachment to God adopted more an attitude of hopelessness. Thus, attachment to God may serve as a resource for individuals coping with severe illness.
To the authors’ knowledge, the present study is the first to explore the role of attachment to God in women’s adjustment to breast cancer. This longitudinal study assesses women’s attachment to God, general coping behavior, and depressive symptomatology at four times: 2–4 days post-biopsy (pre-diagnosis), and 3, 6, and 12 months post-diagnosis.
First, given that life stress may either activate or undermine spirituality as a resource [4], this study explored the pattern of change in attachment to God across time. A comparison of this pattern of change in attachment to God was conducted between women with breast cancer and women with a benign diagnosis to determine whether attachment to God remained a stable force or was destabilized by the impact of the cancer. Bowlby’s attachment theory suggests that attachment styles would remain stable across the lifespan; however, attachment styles may change when the individual is under significant stress [36]. Second, this study explored the relationship between attachment to God and depression and general coping behavior at each point in time. It was hypothesized that a more anxious attachment to God would be related to higher levels of depression and avoidance coping as well as related to lower levels of positive forms of general coping (e.g., acceptance).
Method
Ethical considerations
This study received approval separately from the university and hospital Research Ethics Boards.
Participants
The Women’s Breast Health Centre is a specialized clinic attached to a large general hospital in a Canadian City where women in the region are referred by general practitioners for the evaluation of potential breast abnormalities. All English-speaking women who were referred over a period of 2–3 years were eligible for the study. Women were excluded from the study if they additionally had one or more severe medical conditions (e.g., heart disease, other cancer) that had been diagnosed in the past year. This exclusion criteria was included so that the focus would remain clearly on women’s reactions and adjustment to the illness event of breast cancer which may be qualitatively different (e.g., have different impacts or demands) than other significant illnesses.
Participant recruitment followed a two-step process. First, a research assistant provided information on the study to women as they awaited their core biopsy procedure at the center. In order to be sensitive to the stressfulness of this time, only minimal information about the purpose of the study was provided. When women indicated an interest in hearing more about the study, they were asked to sign a release form so that their name and contact information could be forwarded to a second research assistant working for the study.
Second, within 24–48 h, the second research assistant contacted interested women by phone to discuss the nature of the study, its purpose, and procedures, in greater detail. For those women who agreed to participate, a second phone contact was scheduled to occur within 2–3 days so as to conduct the initial assessment prior to the women receiving their biopsy results. Informed consent was reviewed at the beginning of the second phone call and full consent was verbally given by the women and recorded by the research assistant prior to the commencement of the pre-diagnosis assessment. Two consent forms were mailed to participants: one for the participants’ records and one to be signed and returned in a self-addressed, stamped envelope for the study records.
It should be noted that both women with a benign diagnosis and those with a diagnosis of breast cancer participated in this study.
Data collection
Women completed self-report inventories on various aspects of their well-being at pre-diagnosis, and 3, 6, and 12 months post-diagnosis. As mentioned above, given the short period of time for the process of diagnosis, the first interview (pre-diagnosis) was conducted over the phone. The post-diagnosis assessments were completed by women at their homes and returned in a self-addressed, stamped envelope to the second research assistant.
Measures/instruments
Demographic variables
Women completed a questionnaire on age, marital status, education, cultural background, religious affiliation, and frequency of religious service attendance. Women rated how important religion and spirituality was in their lives on separate, 5-point Likert scales ranging from “not important at all” (1) to “very important” (5).
Cancer variables
Breast cancer patients self-reported on aspects of their illness at 3, 6, and 12 months post-diagnosis including cancer stage, number of positive lymph nodes, and type of surgery and/or treatment.
Attachment to God inventory
The attachment to God inventory (AGI) was used as it demonstrates convergent and discriminant validity, high internal consistency, and a stable two-factor structure (anxious and avoidant attachment to God) [37]. Women completed only the anxious attachment subscale as it taps into relational elements (e.g., fear of abandonment by God, anger at God) which may be affected by a stressor such as breast cancer. In order to reduce the burden on participants, this 14-item subscale was reduced to those 8 items with the highest factor loadings reported in previous analyses [37]. Women rated their attachment to God or a higher power using a 7-point Likert scale ranging from “strongly disagree” (1) to “strongly agree” (7). The total scale score represents the average of the items, with lower to higher scores indicating a movement from a more secure (1) to a more anxious attachment to God (7) respectively (α = .85). Since the scale used in this study is an abbreviated version of the original scale, no scale cutoffs are available.
Brief COPE
The Brief COPE is a 28-item scale which assesses positive and negative general coping behavior and has been used in studies on breast cancer [38, 39]. To reduce the burden on participants in the present study, only six subscales (12 items) of the Brief COPE were included: Active Coping, Denial, Behavioral Disengagement, Instrumental Support, Acceptance, and Positive Reframing. The subscales of Denial and Behavioral Disengagement are considered measures of negative forms of coping (i.e., avoid the stressor) while the other subscales are measures of positive forms of coping (i.e., engagement and problem-solving in relation to the stressor). Women rated the frequency of use of each coping item on a 4-point Likert scale ranging from not at all (1) to very often (4). Instructions were varied slightly depending on the diagnostic group and the time of assessment so as to orient women toward their current situation. Subscales represent the average of the 2 items. Following the procedure described in a study on breast cancer [40], the Denial and Behavioral Disengagement subscales were averaged to form a general measure of Avoidance Coping. The alpha coefficients of internal consistency for all participants at pre-diagnosis were acceptable: Acceptance (α = .79), Active Coping (α = .78), Instrumental Support (α = .85), Positive Reframing (α = .69), and Avoidance Coping (α = .60). Scores on each subscale range between 1 and 4. There are no cutoff scores for these scales.
Center for epidemiological studies–depression scale
A 9-item short form of the center for epidemiological studies–depression scale (CES-D) [41], shown to be valid for non-depressed primary care patients [42], was used. Participants rated each item on a 4-point Likert scale ranging from “rarely/none of the time” (0) to “most or all of the time” (3). A total depression score is the sum of the items, with a high score representing greater depressive symptomatology (α = .87). The total scale score ranges between 0 and 27. There is no cutoff score used in this study.
Data analysis
All data analyses were conducted with SPSS v24.0. Missing data was treated with listwise deletion. Repeated measures ANOVAs with between subjects-factors were run to determine whether there was a significant change in mean level of attachment to God across time for breast cancer patients and women with a benign diagnosis. Attachment to God at each time point were included as repeated factors and the group variable (cancer or benign diagnosis) was included as a between subject factor. The assumptions of repeated measures ANOVA were evaluated and the data revealed that the assumption of sphericity was violated in ANOVAs. As epsilon was greater than .75, the recommended Huynh-Feldt correction was applied [43]. The data also revealed that scores for attachment to God were positively skewed at all time points and analysis was performed on both untransformed and logarithmically transformed data. As the analysis revealed comparable findings, untransformed results are reported herein. It should be noted that all data analyses at pre-diagnosis were conducted using the full sample (n = 277) while longitudinal analyses were conducted on the subsample of 137 due to attrition across time.
Pearson correlations were conducted to investigate the relationships between attachment to God and general coping and depression at each time. These cross-sectional correlations were calculated separately for breast cancer patients and women with a benign diagnosis with the exception of pre-diagnosis when all participants were included in the same analysis.
Finally, based on the correlation results between variables, a model was proposed wherein the association between attachment to God and depression is mediated by avoidance coping behavior. This model was tested cross-sectionally (i.e., at each of the 4 times) using a bootstrapping method with SPSS macro PROCESS [44]. The model was tested for breast cancer patients and women with a benign diagnosis together at pre-diagnosis (time 1) and separately at all three time points following diagnosis. In this way, a determination could be made on the stability of this mediation model at different phases of the adjustment process. The variables attachment to God, avoidance coping, and depression were entered simultaneously into the model. In this model, depression (Y) was regressed on attachment to God (X) and avoidance coping (M; mediator), and M itself is regressed on X. Total, direct, and indirect effects with bias-corrected confidence intervals (based on 5000 bootstraps) were calculated. A confidence interval that does not include zero indicates a positive effect with 95% certainty [45]. Mediation is indicated by the indirect effect of X on Y (which is the product of the coefficients representing the effect of X on M and M on Y). The X on Y total effect is the sum of both the direct and indirect effects.
Results
Sample description
Of the 277 women who were recruited, a subsample of 137 (49.5%) completed at least three of the four phases of the study. About 44.6% of the 140 women who dropped out received a diagnosis of breast cancer while 53.6% received a benign diagnosis. Despite significant attrition at the end of the 12 month period, independent t test analyses at pre-diagnosis demonstrated that participants did not differ from women who dropped out of the study in terms of age, religious or spiritual importance, attachment to God, general coping strategies, or depression.
Of the subsample of 137 women, 40.1% (n = 55) received a diagnosis of breast cancer while 59.9% (n = 82) received a benign diagnosis. See Table 1 for the demographic composition of the cancer and benign groups as assessed at pre-diagnosis. The mean age of the cancer sample was 60.2 years. All breast cancer patients were married or living common-law. Ninety-six percent were of European-Canadian background, with the majority (78.2%) having a Christian background, either Catholic (32.7%) or Protestant (45.5%). Approximately 46% reported that religion was important or very important while 75.5% reported that spirituality was important or very important in their daily lives. Of the 32 breast cancer patients who reported their stage of cancer, 93.7% reported early stage cancer (0, 1, 2) while 6.3% had stage 3 cancer. Approximately 80% percent of the women had no lymph node involvement and 56.3% had a lumpectomy.
The mean age of the benign sample was 51.2 years. All women with a benign diagnosis were married or living common-law. Approximately 92% were of European-Canadian background, with the majority having a Christian background (71.6%), either Catholic (42%) or Protestant (29.6%). Forty-one percent of the benign group reported that religion was important (25%) or very important (16.3%) while 62.5% reported that spirituality was important or very important in their daily lives.
Findings
The repeated measures ANOVAs revealed no significant effect of time for attachment F(2.44, 205.21) = 1.85, p = 0.15 suggesting a stable pattern of attachment to God across time. The analysis also revealed no significant time X group interaction for attachment to God F(2.44, 252) = .13, p = 0.92 indicating similar patterns of attachment for both breast cancer patients and women with a benign diagnosis. Attachment to God means were low (slightly over 2 at the most) at all points in time and for both diagnostic groups indicating that women’s attachment to God remained relatively secure across time (see Table 2).
Pearson correlations revealed that all women with a more anxious attachment to God reported higher levels of depression and avoidance coping and lower levels of acceptance coping at pre-diagnosis. Breast cancer patients with an anxious attachment to God reported more avoidance and less acceptance coping at 3 months post-diagnosis and higher levels of depression at 6 months post-diagnosis. Anxious attachment to God was not related to coping or depression at 12 months post-diagnosis for breast cancer patients. Women with a benign diagnosis who had a more anxious attachment to God reported greater use of avoidance coping and higher levels of depression at 3, 6, and 12 months post-diagnosis (see Table 3 for correlations).
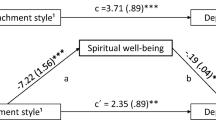
Results for the mediation models can be found in Table 4 (regression coefficients) and in Table 5 (effect sizes). Of the seven models explored, avoidance coping was found to mediate the relationship between anxious attachment to God and depression at time 1 (pre-diagnosis) only. In this model, the total effect and the direct effect were both significant indicating the mediation was partial.
Discussion
The present study investigated the role of attachment to God in women’s response to the threat of breast cancer. First, in relation to the first hypothesis, findings revealed that women’s attachment to God regardless of diagnostic group was relatively secure and that there was no change in this attachment across time. As well, there was no significant difference in attachment to God between the diagnostic groups. These results suggest that attachment to God remains relatively stable and secure within the context of a significant life stressor such as enduring a biopsy procedure alone (benign) or receiving a diagnosis of breast cancer. That is, the threat of a serious illness did not shake women’s faith in God as a reliable source of comfort. These findings support the tenets of adult attachment as put forth by Bowlby [17] and those of attachment to God as suggested by Kirkpatrick [16]; specifically, that attachment style tends to remain fairly stable across time and that secure attachment can serve as a resource for individuals under times of significant life stress.
In relation to the second hypothesis, findings revealed that the more anxiously attached women were to God, the more they engaged in avoidance coping while the more securely they were attached, the less likely they were to rely on avoidance coping prior to receiving a diagnosis. A secure attachment to God may help women remain more directly involved with the stressful demands of the process of diagnosis. Further, the association between attachment to God and avoidance coping strategies was stronger and more consistent across time for those women who received a benign diagnosis. Perhaps women with a benign diagnosis remain uncertain and anxious about their breast health and so they continue to engage their relationship with God in an effort to put the biopsy event and its potential implications behind them. In contrast, women with breast cancer have received a clear answer on their breast health and related demands of the illness and its treatment. As their uncertainty about their breast health has been mitigated and the need for direct action increases (e.g., treatment decision making), breast cancer patients may turn more toward active, problem-focused forms of coping in their adjustment. Finally, breast cancer patients who had a more anxious attachment to God reported using less acceptance coping around the time of surgery and treatment (i.e., 3 months post-diagnosis). It has long been thought that religious/spiritual factors play a significant role in meaning-making and the ability to better accept and integrate stressful life events into one’s life [4] while more negative forms of spirituality, representing the presence of doubt and spiritual struggle, may undermine adjustment to life events such as cancer [10].
Additionally, in relation to hypothesis 2, a more anxious attachment to God was related to higher levels of depression at each point in the adjustment process. The link found between attachment to God and depression supports previous research [28, 30, 31]. While attachment to God remains a significant factor in adjustment for women with a benign diagnosis up to 12 months post-diagnosis, for breast cancer patients it is more strongly related to distress at the time of surgery and treatment (i.e., 3 and 6 months post). These findings support previous research that revealed religious/spiritual factors as being activated more in the early phases of breast cancer adjustment specifically around surgery [12].
Finally, the present study found that the association between attachment to God and depression was partially mediated by avoidance coping but only at pre-diagnosis. Women who were more anxiously attached to God relied more on avoidance coping which in turn led to a greater experience of depression. This finding is important as it suggests that attachment to God may have an impact on women’s ability to stay more directly engaged in coping with the uncertainty of the diagnostic process which in turn has implications for their emotional well-being. If attachment to God is more secure then it may exist as an additional source of support at times of stress [16] which may in fact compensate for any disruption in other sources of support [25].
Limitations and strengths
The current study has some methodological limitations. First, the sample size for breast cancer patients was small especially at the later times of assessment. Second, this sample of Canadian women tended to be less religious as compared to American samples. Thus, results may not be generalizable to more traditionally religious individuals. That said, the study has significant strengths including its longitudinal design, integration of religious/spiritual factors with general measures of coping behavior, and the testing of attachment to God within a mediation model of adjustment to the threat of breast cancer.
Conclusions
The findings of this study supported the theoretical proposal that attachment to God can act as a resource for some individuals at times of stress. Rather than be shaken by doubt and distress, attachment to God remained a stable source of security and comfort for women confronted with the threat of breast cancer. In particular, attachment to God appears to help women cope with the uncertainty they may have about their breast health, whether they were diagnosed with cancer or not. In contrast, a more anxious attachment to God may trigger the use of avoidance coping in response to the demands of breast cancer potentially leading to greater emotional distress. These results suggest that clinicians remain sensitive to and assess the role of religious/spiritual beliefs in women’s adjustment to the threat of breast cancer from pre-diagnosis up to 1 year post-diagnosis. In particular, women’s belief in and experience of a secure or an anxious attachment with God or higher power may function as a potential resource or as an exacerbating factor, respectively, in their adjustment to the threat of breast cancer. Finally, clinicians need to listen for spiritual doubt and whether a woman’s faith in God is shaken by their breast health concerns as an anxious attachment to God may undermine women’s process of adjustment and emotional well-being across time.
References
Linden W, Vodermaier A, MacKenzie R, Greig D (2012) Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J Affect Disord 141(2):343–351. https://doi.org/10.1016/j.jad.2012.03.02
Antoni MH (2003) Stress management intervention for women with breast cancer. American Psychological Association, Washington D.C.
Gall TL, Guirguis-Younger M (2013) Religious and spiritual coping: current theory and research. In: Pargament KI, Exline JJ, Jones JW (eds) APA handbook of psychology, religion and spirituality: Vol. 1. Context, theory and research. American Psychological Association, Washington, DC, pp 349–364
Pargament KI (1997) The psychology of religion and coping. Guilford Press, New York
Schreiber JA, Brockopp DY (2012) Twenty-five years later—what do we know about religion/spirituality and psychological well-being among breast cancer survivors? A systematic review. J Cancer Surviv 6:82–94. https://doi.org/10.1007/s11764-011-0193-7
Schreiber JA (2011) Image of God: Effect on coping and psychospiritual outcomes in early breast cancer survivors. Oncol Nurs Forum 38(3):293–301
Torres E, Dixon C, Richman AR (2016) Understanding the breast cancer experience of survivors: a qualitative study of African American women in rural eastern North Carolina. J Cancer Educ 31:198–206. https://doi.org/10.1007/s13187-015-0833-0
Hammoudeh W, Hogan D, Giacaman R (2017) From a death sentence to a disrupted life: Palestinian women’s experiences and coping with breast cancer. Qual Health Res 27(4):487–496. https://doi.org/10.1177/1049732316628833
Assing Hvidt E, Raun Iversen H, Ploug Hansen H (2013) ‘Someone to hold the hand over me’: the significance of transpersonal ‘attachment’ relationships of Danish cancer survivors. Eur J Cancer Care 22:726–737. https://doi.org/10.1111/ecc.12097
Exline JJ, Park CL, Smyth JM, Carey MP (2011) Anger toward God: social-cognitive predictors, prevalence, and links with adjustment to bereavement and cancer. J Pers Soc Psychol 100(1):129–148. https://doi.org/10.1037/a0021716
Gall TL, Kristjansson E, Charbonneau C, Florack P (2009) A longitudinal study on the role of spirituality in response to the diagnosis and treatment of breast cancer. J Behav Med 32:174–186. https://doi.org/10.1007/s10865-008-9182-3
Thuné-Boyle ICV, Stygall J, Keshtgar MRS, Davidson TI, Newman SP (2013) Religious/spiritual coping resources and their relationship with adjustment in patients newly diagnosed with breast cancer in the UK. Psycho-Oncology 22:646–658. https://doi.org/10.1002/pon.3048
Gall TL, Bilodeau C (2017) “Why me?” - women’s use of spiritual causal attributions in making sense of breast cancer. Psychol Health 32(6):709–727. https://doi.org/10.1080/08870446.2017.1293270
Pargament KI, Koenig HG, Tarakeshwar N, Hahn J (2004) Religious coping methods as predictors of psychological, physical, and social outcomes among medically ill elderly patients: a two-year longitudinal study. J Health Psychol 9:713–730. https://doi.org/10.1177/1359105304045366
Granqvist P (2014) Mental health and religion from an attachment viewpoint: overview with implications for future research. Ment Health Relig Cult 17(8):777–793. https://doi.org/10.1080/13674676.2014.908513
Kirkpatrick L (2005) Attachment, evolution and the psychology of religion. Guilford Press, New York
Bowlby J (1988) A secure base: clinical applications of attachment theory. Routledge, London
Cassidy J, Shaver PR (eds) (1999) Handbook of attachment: theory, research, and clinical applications. Guilford Press, New York
Turan B, Osar Z, Turan JM, Ilkova H, Damci T (2003) Dismissing attachment and outcome in diabetes: the mediating role of coping. J Soc Clin Psychol 22:607–626. https://doi.org/10.1521/jscp.22.6.607.22933
Mikulincer M, Florian V (1999) Maternal-fetal bonding, coping strategies, and mental health during pregnancy: the contribution of attachment style. J Soc Clin Psychol 18:255–276. https://doi.org/10.1521/jscp.1999.18.3.255
Cozzarelli C, Sumer N, Major B (1998) Mental models of attachment and coping with abortion. J Pers Soc Psychol 74:453–467 Retrieved from https://www.researchgate.net
Pielage S, Gerlsma C, Schaap C (2000) Insecure attachment as a risk factor for psychopathology: the role of stressful events. Clin Psychol Psychother 7:296–302. https://doi.org/10.1002/1099-0879(200010)7:4 < 296::AID-CPP262 > 3.0.CO;2-8
Larose S, Boivin M, Doyle AB (2001) Parental representations and attachment style as predictors of support seeking behaviors and perceptions of support in an academic counseling relationship. Pers Relat 8:93–113. https://doi.org/10.1111/j.1475-6811.2001.tb00030.x
Granqvist P (2005) Building a bridge between attachment and religious coping: tests of moderators and mediators. Ment Health Relig Cult 8:35–47. https://doi.org/10.1080/13674670410001666598
Cooper LB, Bruce AJ, Harman MJ, Boccaccini MT (2005) Differentiated styles of attachment to God and varying religious coping efforts. J Psychol Theol 37(2):134–141
Schottenbauer MA, Klimes-Dougan B, Rodriguez BF, Arnkoff DB, Glass CR, Lasalle VH (2006) Attachment and affective resolution following a stressful event: general and religious coping as possible mediators. Ment Health Relig Cult 9:448–471. https://doi.org/10.1080/13694670500440684
Wei M, Ku T-Y, Chen H-J, Wade N, Liao KY-H, Guo G-J (2012) Chinese Christians in America: attachment to God, stress, and well-being. Couns Values 57:162–180
Kelley MM, Chan KT (2012) Assessing the role of attachment to God, meaning, and religious coping as mediators in the grief experience. Death Stud 36:199–227. https://doi.org/10.1080/07481187.2011.553317
Kirkpatrick LA, Shaver PR (1992) An attachment-theoretical approach to romantic love and religious belief. Personal Soc Psychol Bull 18:266–275
Bishop AJ (2008) Stress and depression among older residents in religious monasteries: do friends and God matter? Int J Aging Hum Dev 67(1):1–23. https://doi.org/10.2190/AG.67.1.a
Bradshaw M, Ellison CG, Marcum JP (2010) Attachment to God, images of God, and psychological distress in a nationwide sample of Presbyterians. Int J Psychol Relig 20:130–147. https://doi.org/10.1080/10508611003608049
Homan KJ (2014) A mediation model linking attachment to God, self-compassion, and mental health. Ment Health Relig Cult 17(10):977–989. https://doi.org/10.1080/13674676.2014.984163
Reiner SR, Anderson TL, Lewis Hall ME, Hall TW (2010) Adult attachment, God attachment and gender in relation to perceived stress. J Psychol Theol 38(3):175–185
Gall TL, Charbonneau C, Clarke NH, Grant K, Joseph A, Shouldice L (2005) Understanding the nature and role of spirituality in relation to coping and health: a conceptual framework. Can Psychol 46(2):88–104
Cassibba R, Papagna S, Calabrese MT, Costantino E, Paterno A, Granqvist P (2014) The role of attachment to God in secular and religious/spiritual ways of coping with a serious disease. Ment Health Relig Cult 17(3):252–261. https://doi.org/10.1080/13674676.2013.795138
Mikulincer M, Shaver PR (2007) Attachment in adulthood: structure, dynamics and change. The Guilford Press, New York
Beck R, McDonald A (2004) Attachment to God: the attachment to God inventory, tests of working model correspondence, and an exploration of faith group differences. J Psychol Theol 32(2):92–103 Retrieved from http://www.callisto-science.org
Carver CS (1997) You want to measure coping but your protocol’s too long: consider the Brief COPE. Int J Behav Med 4(1):92–100
Carver CS, Pozo C, Harris SD et al (1993) How coping mediates the effect of optimism on distress: a study of women with early stage breast cancer. J Pers Soc Psychol 65(2):375–390
Stanton AL, Danoff-Burg S, Cameron CL, Bishop M, Collins CA, Kirk SB, Sworowski LA, Twillman R (2000) Emotionally expressive coping predicts psychological and physical adjustment to breast cancer. J Consult Clin Psychol 68:875–882
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1(3):385–401. https://doi.org/10.1177/014662167700100306
Santor DA, Coyne JC (1997) Shortening the CES–D to improve its ability to detect cases of depression. Psychol Assess 9(3):233–243. https://doi.org/10.1037/1040-3590.9.3.233
Girden E (1992) ANOVA: Repeated measures. Sage, Newbury Park
Hayes (2014); http://processmacro.org/download.html
Hayes AF (2017) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach, 2nd edn. The Guilford Press, New York
Funding
This research was supported by a Standard Research Grant (No. 410-2006-0880) from the Social Sciences and Humanities Research Council of Canada.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 12 kb)
Rights and permissions
About this article

Cite this article
Gall, T.L., Bilodeau, C. Attachment to God and coping with the diagnosis and treatment of breast cancer: a longitudinal study. Support Care Cancer 28, 2779–2788 (2020). https://doi.org/10.1007/s00520-019-05149-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-019-05149-6