
Abstract
Background
The effect of sarcopenia on digestive carcinoma surgery outcomes is controversial. We aimed to assess the effect of sarcopenia defined by the European Working Group on Sarcopenia in Older People (EWGSOP) or the Asian Working Group for Sarcopenia (AWGS) on outcomes following digestive carcinoma surgery.
Methods
Eligible studies were searched from PubMed, EMBASE and other databases from inception to April 2018. We conducted a meta-analysis to estimate the risk ratios or mean differences of outcomes in the sarcopenia group versus the non-sarcopenia group. Stratified analyses and sensitivity analyses were performed.
Results
We included 11 cohort studies, with a sarcopenia prevalence ranging from 11.6 to 33.0%. Sarcopenia was associated with an increased risk of total complications (RR = 1.87, P < 0.00001), major complications (RR = 2.45, P = 0.002), re-admissions (RR = 2.53,P < 0.0001), infections (RR = 2.23, P = 0.09), severe infections (RR = 2.96, P = 0.04), 30-day mortality (RR = 3.36, P = 0.001), longer hospital stay (MD = 4.61, P = 0.001) and increased hospitalization expenditures (SMD = 0.25, P = 0.02). Sarcopenia differentially affected outcomes when stratified, and the results were stable.
Conclusions
Sarcopenia defined by the EWGSOP or AWGS Consensus was a high-risk factor for digestive carcinoma surgery outcomes. Different tumour site and muscle mass measurements are the sources of heterogeneity. More high-quality studies are needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Digestive carcinomas mainly fall into gastric, colorectal, esophageal and liver types. According to the global estimation of cancer incidence and mortality in 2018 announced by International Agency for Research on Cancer (IARC), new cases of digestive carcinoma accounted for 16.8% of the total new cancers and digestive cancer-related deaths 35.4% of the total [1]. Currently, surgery is still the main therapeutic method; however, due to the limitation of early diagnosis and treatment, digestive carcinomas have higher mortality than other neoplasms [2, 3]. Since the aging problem is getting so serious that senior citizens will account for 22% of all population in the world until 2050, the incidence of digestive carcinoma is higher among the elderly [4]. Studies have shown that the complication rate, mortality and length of hospital stay after digestive carcinoma surgery increase with patient age [5, 6].
Sarcopenia was first put forward by Irwin Rosenberg in 1989 and defined as an age-related loss of skeletal muscle mass [7]. It has been found that focussing solely on skeletal muscle mass may limit clinical applications. Muscle mass has a non-linear relationship with muscle strength [8], and the loss of muscle strength also has important clinical significance. For this reason, the 2010 EWGSOP Consensus [9] and the 2014 AWGS Consensus [10] defined sarcopenia as a syndrome characterized by a progressive and generalized loss of skeletal muscle mass and strength with a risk of adverse outcomes, such as physical disability, poor quality of life and death. Several studies have shown that sarcopenia may increase the risk of postoperative complications and thus reduce the survival rate of patients undergoing digestive carcinoma surgery [11, 12].
Sarcopenia always occurs as part of the aging process [13, 14], muscle loss starts at 30 years of age and accelerates after 70 years [15] and the prevalence of sarcopenia is 5~13% in people aged from 60 to 70 years old as well as 11~50% in people aged over 80 years [16]. Sarcopenia is also related to malnutrition, disuse, surgery, cancer, chronic diseases and so on [17,18,19,20]. The characteristics of elderly patients undergoing digestive carcinoma surgery are consistent with the main causes of sarcopenia such as aging, malnutrition and cancer. Therefore, the prevalence of sarcopenia in elderly patients undergoing digestive carcinoma surgery is higher than that in the general population, varying from 11.1 to 76% [21].
To improve the poor prognosis, therefore, we should pay more attention to such related risk factors as sarcopenia. Although the EWGSOP and AWGS Consensus have updated the definition of sarcopenia, most of studies still confine sarcopenia to the loss of muscle mass, ignoring the decline of muscle strength and function [22,23,24,25]. The effect of sarcopenia on clinical outcomes is controversial among studies using different definitions of sarcopenia. For example, one study [26] concluded that sarcopenia defined by AWGS Consensus was only related to postoperative complications but not to readmissions, hospital stay and mortality. But another study [24] showed that sarcopenia, defined as the loss of muscle mass, was related to a higher risk of longer hospital stay. Recently, several meta-analyses [21, 27] aimed to find a relationship between sarcopenia and clinical outcomes, but these studies included articles that define sarcopenia using different criteria, which may have resulted in some bias and great heterogeneity. A related meta-analysis [28] paid attention to this aspect and conducted a subgroup analysis stratified by the different definitions of sarcopenia, suggesting that studies using the EWGSOP definition had higher relative risks associated with sarcopenia and less heterogeneity. However, that analysis, only with three studies based on the EWGSOP Consensus definition, also had high heterogeneity and focused only on postoperative complications. We found that the effect of sarcopenia on outcomes is also controversial among studies using the EWGSOP or AWGS Consensus definition [12, 29].
Therefore, our study aimed to further assess the effect of sarcopenia just defined by the EWGSOP or AWGS Consensus on clinical outcomes in elderly patients undergoing digestive carcinoma surgery.
Methods
The Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines were followed when we conducted and reported this systematic review [30].
Literature search
The PubMed, Web of Science, EMBASE, Cochrane Library, Science Direct, CNKI, and WanFang databases were searched from inception to April 2018. The search strategy keywords and the medical subject headings (MeSH) used included digestive carcinoma, surgery, and sarcopenia. Reference lists of all relevant systematic reviews were searched to identify additional studies. The literature search was conducted by one author, who had received systematic training. The languages of the literature were limited to English and Chinese.
Eligibility criteria
We included clinical studies that met these criteria: (1) only observational studies; (2) studies investigating the effects of sarcopenia on clinical outcomes; (3) the target patients were aged 60 years or older with digestive carcinoma and received surgical treatment; (4) considering there are different definitions of sarcopenia (Box 1), we just included studies that defined sarcopenia by the EWGSOP or AWGS Consensus; and (5) the end points of interest included at least one of the following characteristics: total complications, major complications, infections, severe infections, re-admissions, 30-day mortality, hospital stay and hospitalization expenditures. We excluded meeting proceedings, letters, reviews, commentary and grey literature.
Box 1 The definitions of sarcopenia
Reference | Irwin Rosenberg(1989) | EWGSOP Consensus(2010)/AWGS Consensus(2014) |
|---|---|---|
Definition | Loss of skeletal muscle mass | Loss of skeletal muscle mass and strength or physical function |
Data extraction
Two researchers independently extracted the data and any disagreements were resolved via consensus. We extracted the first author’s last name, publication year, country, study type, sample size, sex proportion, tumour site, measurements cut-off value for sarcopenia and the postoperative outcomes, including total complications, major complications, infections, severe infections, re-admissions and 30-day mortality after surgery, hospital stay and hospitalization expenditures. We defined postoperative complications using the Clavien-Dindo classification as follows [31]: “total complications” were equal to “Clavien-Dindo grade ≥ 2”, and “major complications” were equal to “Clavien-Dindo grade ≥ 3”. If insufficient information was available, then the authors were contacted via e-mail.
Quality assessment
Risk of bias was assessed by two researchers independently using the Newcastle–Ottawa Scale (NOS) [32]. A score equal to or less than 5 was considered as low quality, 6 or 7 as moderate and 8 or 9 as high. Any disagreements were resolved through consensus.
Statistical analysis
The meta-analysis was undertaken using Review Manager (RevMan V.5.3; Cochrane Collaboration, Oxford, UK) when more than two studies reported the same outcome with a significance level of 0.05 [33]. We pooled the risk ratios (RRs) or mean differences (MDs) for dichotomous or continuous variables using a fixed or random effects model as appropriate. The I2 statistic was used to quantify statistical heterogeneity. The fixed effects model was used when I2 ≤ 30%, and a random effects model was used when I2 > 30%. Subgroup analyses were performed to investigate the origin of the heterogeneity [34]. We performed stratified analyses according to the muscle mass measurements and tumour site to investigate the effect modifications of these variables on the association between sarcopenia and the risk of clinical outcomes. Then, we conducted sensitivity analyses to test the robustness.
Results
Search results
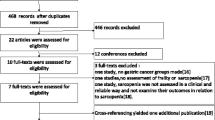
From a total of 10,226 records identified following a detailed search, 11 studies [11, 12, 26, 29, 35,36,37,38,39,40,41] with 2419 participants were finally included (Fig. 1). Of these studies, two were retrospective cohort studies [11, 29], and the others were prospective cohort studies. One study focused on colorectal cancer patients [26], six focused on gastric cancer patients [12, 29, 36, 38, 39, 41], two focused on esophageal cancer patients [11, 40] and two focused on liver cancer patients undergoing liver transplantation [35, 37]. The characteristics of the included studies are summarized in Table 1. The clinical outcomes of the included studies are shown in Table 2.

The detailed literature search and screening process
Quality assessment
The quality assessments of the 11 included studies are summarized in Table 3. Of these studies, four were graded as high quality [12, 26, 35, 41], six as moderate [11, 36,37,38,39,40] and one as low [29].
Relationship between sarcopenia and complications
Eight studies [12, 26, 29, 35, 36, 38, 39, 41] reported an association of sarcopenia with total complications. One study was excluded due to loss of data [36]. We calculated the summary RR value using a random effects model, which suggested that sarcopenia was associated with an increased risk of total complications, with a pooled RR of 1.87 (95% CI 1.52–2.30). High heterogeneity was found across these studies (χ2 = 10.74, P = 0.10, I2 = 44%) (Fig. 2a). The pooled results from the four studies focused on major complications [12, 26, 29, 41] that suggested that sarcopenia was associated with an increased risk of major complications (RR = 2.45, 95% CI 1.38–4.32). No significant heterogeneity was observed across these four studies (χ2 = 2.18, P = 0.53, I2 = 0%) (Fig. 2b).

Summary results of the clinical outcomes for subjects with sarcopenia versus those without sarcopenia. a Total complications. b Major complications. c Re-admissions. d Infections. e Severe infections. f Thirty-day mortality. g The length of the hospital stay
Relationship between sarcopenia and re-admissions
Five studies [12, 26, 39,40,41] reported a relation of sarcopenia to re-admissions. The pooled results from these five studies showed that sarcopenia was associated with an increased risk of re-admission (RR = 2.53, 95% CI 1.66–3.85). No significant heterogeneity was found among the studies (χ2 = 2.09, P = 0.72, I2 = 0%) (Fig. 2c).
Relationship between sarcopenia and infections
Five studies [12, 26, 29, 40, 41] focused on patients’ postoperative infections, such as surgical site infections and pneumonia. The results showed that sarcopenia was associated with an increased risk of infections (RR = 2.23, 95% CI 1.23–4.03) in the random effects model due to relatively high heterogeneity (χ2 = 8.16, P = 0.09, I2 = 51%) (Fig. 2d). Two studies [29, 35] reported an association between sarcopenia and severe infections with a CD grade of IIIa or higher. The analyses showed that sarcopenia conferred a higher risk of severe infections, with a pooled RR of 2.96 (95% CI 1.04–8.46) in the fixed effects model due to a lack of heterogeneity (χ2 = 0.57, P = 0.45, I2 = 0%) (Fig. 2e).
Relationship between sarcopenia and 30-day mortality
Three studies [35, 37, 41] observed 30-day mortality. We combined the 30-day mortality data using a fixed effects model given the relatively low heterogeneity (χ2 = 2.63, P = 0.27, I2 = 24%). The results showed that sarcopenia was associated with an increased risk of 30-day mortality, with a pooled RR of 3.36 (95% CI 1.60–7.06) (Fig. 2f).
Relationship between sarcopenia and the length of the hospital stay
Nine studies [11, 12, 26, 29, 35, 38, 39, 41] focused on sarcopenia and the length of the hospital stay. We calculated the mean difference using a random effects model due to the high heterogeneity (χ2 = 23.12, P = 0.003, I2 = 65%). The results showed that sarcopenia was associated with a longer postoperative hospital stay, with a mean difference of 4.61 (95% CI 1.84–7.39) (Fig. 2g).
Relationship between sarcopenia and hospitalization expenditures
Two studies [39, 41] reported an association between sarcopenia and hospitalization expenditures. In the fixed effects model, sarcopenia was associated with more hospitalization expenditures, with a standardized mean difference of 0.25 (95% CI 0.04–0.46). No significant heterogeneity was found between the studies (χ2 = 0.11, P = 0.74, I2 = 0%) (Fig. 2h).
Subgroup analyses
We did subgroup analyses according to the muscle mass measurements and tumour site. Results are shown in Table 4.
Discussion
In our study, the prevalence of sarcopenia varied from 11.6 to 33% in the included studies, which was lower than that of other studies because our included studies defined sarcopenia based only on the EWGSOP or AWGS Consensus. The prevalence of sarcopenia was 18.14% for gastric, 11.9% for colorectal, 29.7% for esophageal, and 19.7% for liver cancer patients. We infer that the reason for the higher prevalence of sarcopenia in oesophageal cancer patients might be related to the inadequate intake of energy and proteins caused by progressive dysphagia.
The pathology of sarcopenia is complex and can include specific nutritional deficiencies [42], a lack of physical activity [43], insulin resistance [44] and chronic inflammation [45]. Sarcopenia may also result in a decline in the metabolic rate and aerobic capacity and an increased risk of physical disability, poor quality of life and death [46, 47]. The prognosis of digestive carcinoma surgery is unfavourable; thus, enhanced recovery after surgery, advanced surgical techniques, perioperative nursing and preoperative risk assessments have received more attention as a way to improve the prognosis. Currently, preoperative risk assessments include the American Society of Anaesthesiologists classification, nutritional risk screening and a preoperative routine examination. However, these indicators are not accurate. The guidelines from the American College of Surgeons also highlighted the importance of assessing sarcopenia prior to oncologic surgery in the elderly [48]. Recently, some articles have investigated the association between sarcopenia and the risk of adverse outcomes following digestive carcinoma surgery, although the conclusions are controversial. To the best of our knowledge, our meta-analysis is the first to investigate the relationships between sarcopenia defined by the EWGSOP or AWGS Consensus and outcomes after surgery for digestive carcinoma. Our meta-analysis showed that sarcopenia was associated with a high risk of worse clinical outcomes, including total complications, major complications, re-admissions, infections, severe infections, 30-day mortality, hospital stay and hospitalization expenditures. These results suggest that we should add sarcopenia to preoperative risk assessments and construct a surgical risk prediction model. Clinicians need to analyse risk factors for sarcopenia in patients who plan to undergo digestive carcinoma surgery and then formulate interventions for specific disease and nutritional statuses based on the risk factors to alleviate adverse postoperative outcomes.
The heterogeneity of our meta-analysis was low, except for total complications, infections and lengths of hospital stay. Subgroup analyses showed that sarcopenia remained a high-risk factor for re-admissions across muscle mass measurements, whereas different effect results were found for total complications, infections and lengths of hospital stay in the different subgroups. Currently, many methods for muscle mass measurement have been developed, including dual X-ray absorptiometry (DXA), BIA, sonography, magnetic resonance imaging (MRI) and CT. CT is the gold standard and has become part of preoperative investigations in patients with abdominal carcinoma. BIA, DXA and skinfold measurements are not performed routinely during oncological evaluations, but these measurements also have their own advantages. In this meta-analysis, we found that sarcopenia significantly affected all outcomes in the CT subgroup, so the lack of a uniform muscle mass assessment methodology might have affected the study outcomes. We also found that the source of heterogeneity in total complications and infections was the muscle mass measurements. Thus, clinical trials need to compare other muscle mass measurements with CT and recommend the best method for different races and illnesses to narrow measurement error in the future. When stratified by tumour site, sarcopenia remained a high-risk factor for total complications regardless of tumour site. Sarcopenia influenced re-admissions more significantly in the gastric cancer subgroup. Additionally, sarcopenia increased the risk of total complications and infections more strongly in the colorectal cancer subgroup and affected the hospital stay more severely in the esophageal cancer subgroup. We also found that tumour site resulted in high heterogeneity in the hospital stay analysis. As a result, we should pay more attention to investigations of the specific, greater impact of sarcopenia on patients with carcinoma, such as colorectal carcinoma. Sensitivity analyses proved that our results were stable.
The main findings of this systematic review need to be considered in the context of several key limitations. First, to reduce heterogeneity from different definition criteria between studies, we included only 11 articles that defined sarcopenia using the EWGSOP or AWGS Consensus. This low number may have led to some bias in our conclusions. Secondly, we performed subgroup analysis based only on the different muscle mass measurements and tumour site due to the small number of studies. Lastly, although we suspected that the article quality might introduce some bias, due to the small number of articles with only one low-quality article included, we did not stratify another subgroup analysis.
Conclusions
Sarcopenia defined by the EWGSOP or AWGS Consensus was associated with a high risk of adverse outcomes across digestive carcinoma patients who had received surgery. By comparing different muscle mass measurements and tumour sites, our meta-analysis suggested that more attention should be paid to comparing the best muscle mass measurement, identifying high-risk patients for sarcopenia among digestive carcinoma patients and performing more high-quality studies. Due to the lack of a universal definition of sarcopenia, the findings should be interpreted with caution.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424. https://doi.org/10.3322/caac.21492
Thrumurthy SG, Chaudry MA, Hochhauser D, Mughal M (2013) The diagnosis and management of gastric cancer. BMJ (Clinical research ed) 347(nov04 1):f6367
Papenfuss WA, Kukar M, Oxenberg J, Attwood K, Nurkin S, Malhotra U, Wilkinson NW (2014) Morbidity and mortality associated with gastrectomy for gastric cancer. Ann Surg Oncol 21(9):3008–3014
Nations DEU (2013) World population prospects: the 2012 revision highlights and advance tables. New York United Nations Department of Economic & Social Affairs
Wagner D, Demarco MA, Amini N, Buttner S, Segev D, Gani F, Pawlik TM (2016) Role of frailty and sarcopenia in predicting outcomes among patients undergoing gastrointestinal surgery. World J Gastrointest Surg 8(1):27–40
Takeshita H, Ichikawa D, Kubota T, Okamoto K, Shiozaki A, Fujiwara H, Otsuji E (2013) Surgical outcomes of gastrectomy for elderly patients with gastric cancer. World J Surg 37(12):2891–2898
Rosenberg IH (1997) Sarcopenia: origins and clinical relevance. J Nutr 127(5 Suppl):990s–991s. https://doi.org/10.1093/jn/127.5.990S
Binay Safer V, Safer U, Kaplan M, Terekeci H, Top C (2015) Limitations of the definition of sarcopenia in cancer surgery. J Surg Oncol 112(1):116–116
Cruz-Jentoft AJ, Jean Pierre B, Bauer JM, Yves B, Tommy C, Francesco L, Martin FC, Jean-Pierre M, Yves R, Schneider SM (2010) Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 39:412–423
Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, Chou MY, Chen LY, Hsu PS, Krairit O, Lee JS, Lee WJ, Lee Y, Liang CK, Limpawattana P, Lin CS, Peng LN, Satake S, Suzuki T, Won CW, Wu CH, Wu SN, Zhang T, Zeng P, Akishita M, Arai H (2014) Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 15(2):95–101
Makiura D, Ono R, Inoue J, Kashiwa M, Oshikiri T, Nakamura T, Kakeji Y, Sakai Y, Miura Y (2016) Preoperative sarcopenia is a predictor of postoperative pulmonary complications in esophageal cancer following esophagectomy: a retrospective cohort study. Journal of Geriatric Oncology 7(6):430–436
Wang SL, Zhuang CL, Huang DD, Pang WY, Lou N, Chen FF, Zhou CJ, Shen X, Yu Z (2016) Sarcopenia adversely impacts postoperative clinical outcomes following gastrectomy in patients with gastric cancer: a prospective study. Ann Surg Oncol 23(2):556–564
Morley JE (2012) Sarcopenia in the elderly. Fam Pract 29(Suppl 1):i44–i48. https://doi.org/10.1093/fampra/cmr063
Walston JD (2012) Sarcopenia in older adults. Curr Opin Rheumatol 24(6):623–627
Haehling SV, Morley JE, Anker SD (2010) An overview of sarcopenia: facts and numbers on prevalence and clinical impact. J Cachexia Sarcopenia Muscle 1(2):129–133
Morley JE, Anker SD, Haehling SV (2014) Prevalence, incidence, and clinical impact of sarcopenia: facts, numbers, and epidemiology—update 2014. J Cachexia Sarcopenia Muscle 5(4):253–259
Muscaritoli M, Anker SJ, Aversa Z, Bauer JM, Biolo G, Boirie Y, Bosaeus I, Cederholm T, Costelli P, Fearon KC (2010) Consensus definition of sarcopenia, cachexia and pre-cachexia: joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin Nutr 29(2):154–159
Laviano A, Meguid MM, Inui A, Muscaritoli M, Rossi-Fanelli F (2005) Therapy insight: cancer anorexia-cachexia syndrome—when all you can eat is yourself. Nat Clin Pract Oncol 2(3):158–165
Scott D, Blizzard L, Fell J, Giles G, Jones G (2010) Associations between dietary nutrient intake and muscle mass and strength in community-dwelling older adults: the Tasmanian Older Adult Cohort Study. J Am Geriatr Soc 58(11):2129–2134
Valenzuela RER, Ponce JA, Morales-Figueroa GG, Muro KA, Carreón VR, Alemán-Mateo H (2013) Insufficient amounts and inadequate distribution of dietary protein intake in apparently healthy older adults in a developing country: implications for dietary strategies to prevent sarcopenia. Clin Interv Aging 8(2):1143–1148
Zhang G, Meng S, Li R, Ye J, Zhao L (2017) Clinical significance of sarcopenia in the treatment of patients with primary hepatic malignancies, a systematic review and meta-analysis. Oncotarget 8(60):102474–102485
Voron T, Tselikas L, Pietrasz D, Pigneur F, Laurent A, Compagnon P, Salloum C, Luciani A, Azoulay D (2015) Sarcopenia impacts on short- and long-term results of hepatectomy for hepatocellular carcinoma. Ann Surg 261(6):1173–1183
Peng P, Hyder O, Firoozmand A, Kneuertz P, Schulick RD, Huang D, Makary M, Hirose K, Edil B, Choti MA (2012) Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma. J Gastrointest Surg 16(8):1478–1486
Lieffers JR, Bathe OF, Fassbender K, Winget M, Baracos VE (2012) Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br J Cancer 107(6):931–936
Nakashima Y, Saeki H, Nakanishi R, Sugiyama M, Kurashige J, Oki E, Maehara Y (2017) Assessment of sarcopenia as a predictor of poor outcomes after esophagectomy in elderly patients with esophageal cancer. Ann Surg 267:1
Huang DD, Wang SL, Zhuang CL, Zheng BS, Lu JX, Chen FF, Zhou CJ, Shen X, Yu Z (2015) Sarcopenia, as defined by low muscle mass, strength and physical performance, predicts complications after surgery for colorectal cancer. Colorectal Dis Off J Assoc Coloproctol Great Britain Ireland 17(11):O256–O264
Jones K, Gordon-Weeks A, Coleman C, Silva M (2017) Radiologically determined sarcopenia predicts morbidity and mortality following abdominal surgery: a systematic review and meta-analysis. World J Surg 41(9):2266–2279
Simonsen C, De HP, Bjerre ED, Suetta C, Hojman P, Pedersen BK, Svendsen LB, Christensen JF (2018) Sarcopenia and postoperative complication risk in gastrointestinal surgical oncology: a meta-analysis. Ann Surg 268(1):1
Fukuda Y, Yamamoto K, Hirao M, Nishikawa K, Nagatsuma Y, Nakayama T, Tanikawa S, Maeda S, Uemura M, Miyake M (2015) Sarcopenia is associated with severe postoperative complications in elderly gastric cancer patients undergoing gastrectomy. Gastric Cancer : official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association 34(3):S227–S227
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Clinical research ed)
Dindo D, Demartines N, Clavien P (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Chuling F, Hui H, Zuojun X (2016) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies
Doi SAR, Barendregt JJ, Khan S, Thalib L, Williams GM (2015) Advances in the meta-analysis of heterogeneous clinical trials I: the inverse variance heterogeneity model. Contemporary Clin Trials 45(Pt A):130–138
Shuster JJ (2011) Review: Cochrane handbook for systematic reviews for interventions, Version 5.1.0, published 3/2011. Julian P.T. Higgins and Sally Green, Editors. Res Synth Methods 2 (2):126–130
Harimoto N, Yoshizumi T, Izumi T, Motomura T, Harada N, Itoh S, Ikegami T, Uchiyama H, Soejima Y, Nishie A (2017) Clinical outcomes of living liver transplantation according to the presence of sarcopenia as defined by skeletal muscle mass, hand grip, and gait speed. Transplant Proc 49(9):2144–2152
Huang DD, Chen XX, Chen XY, Wang SL, Shen X, Chen XL, Yu Z, Zhuang CL (2016) Sarcopenia predicts 1-year mortality in elderly patients undergoing curative gastrectomy for gastric cancer: a prospective study. J Cancer Res Clin Oncol 142(11):1–10
Kaido T, Ogawa K, Fujimoto Y, Ogura Y, Hata K, Ito T, Tomiyama K, Yagi S, Mori A, Uemoto S (2013) Impact of sarcopenia on survival in patients undergoing living donor liver transplantation. Am J Transplant 13(6):1549–1556
Kawamura T, Makuuchi R, Tokunaga M, Tanizawa Y, Bando E, Yasui H, Aoyama T, Inano T, Terashima M (2018) Long-term outcomes of gastric cancer patients with preoperative sarcopenia. Ann Surg Oncol 4:1–8
Cai Z, Cai D, Yao D, Chen Y, Wang J, Li Y (2016) Associations between body composition and nutritional assessments and biochemical markers in patients with chronic radiation enteritis: a case-control study. Nutr J 15(1):57. https://doi.org/10.1186/s12937-016-0177-6
Makiura D, Ono R, Inoue J, Fukuta A, Kashiwa M, Miura Y, Oshikiri T, Nakamura T, Kakeji Y, Sakai Y (2018) Impact of sarcopenia on unplanned readmission and survival after Esophagectomy in patients with esophageal cancer. Ann Surg Oncol 25(2):1–9
Zhou CJ, Zhang FM, Zhang FY, Yu Z, Chen XL, Shen X, Zhuang CL, Chen XX (2017) Sarcopenia: a new predictor of postoperative complications for elderly gastric cancer patients who underwent radical gastrectomy. J Surg Res 211:137–146
Visser M, Deeg DP (2003) Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): the Longitudinal Aging Study Amsterdam. J Clin Endocrinol Metab 88(12):5766–5772
Patrick K, Arny F, Juan L, Robert W, Evans WJ (2007) Effect of 10 days of bed rest on skeletal muscle in healthy older adults. Jama 297(16):1772–1774
Evans WJ, Farrell PA (2011) The aging pancreas: effects of aging on insulin secretion and action
Matteo C, Kritchevsky SB, Baumgartner RN, Atkinson HH, Penninx BWHJ, Leon L, Palla SL, Ambrosius WT, Tracy RP, Marco P (2005) Sarcopenia, obesity, and inflammation—results from the trial of angiotensin converting enzyme inhibition and novel cardiovascular risk factors study. Am J Clin Nutr 82(2):428
Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, Garry PJ, Lindeman RD (1998) Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 147(8):755–763
Evans WJ (2010) Skeletal muscle loss: cachexia, sarcopenia, and inactivity. Am J Clin Nutr 91(4):1123S–1127S
Chow WB, Rosenthal RA, Merkow RP, Ko CY, Esnaola NF (2012) Optimal preoperative assessment of the geriatric surgical patient: a best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J Am Coll Surg 215(4):453–466
Funding
This work was funded by the Postgraduate Research & Practice Innovation Program of Jiangsu Province awarded to Xu Xinyi.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hua, H., Xu, X., Tang, Y. et al. Effect of sarcopenia on clinical outcomes following digestive carcinoma surgery: a meta-analysis. Support Care Cancer 27, 2385–2394 (2019). https://doi.org/10.1007/s00520-019-04767-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-019-04767-4