
Abstract
Objective
This study evaluated the prevalence, impact and predictive factors for the occurrence of febrile neutropenia (FN) in elderly patients receiving adjuvant myelosuppressive chemotherapy despite primary prophylaxis with G-CSF (breakthrough FN).
Methods
This was a single-centre, observational, retrospective cohort study. Elderly cancer patients (≥65 years old) who have received adjuvant chemotherapy with primary prophylaxis using G-CSF from Jan 2008 to Aug 2011 were included. Variables identified by the univariate analysis as being associated with FN were included in a multivariable logistic model to investigate the independence of its association with FN.
Results
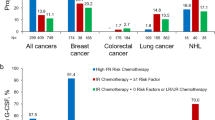
One hundred and forty-five patients and 704 cycles of chemotherapy were analyzed in this study, of which majority were Chinese (79.3 %). The median age of the patients was 69 years old (IQR: 66, 74). Majority of these patients were diagnosed with lymphoma (54.5 %), followed by breast cancer (34.5 %) and small cell lung cancer (8.3 %). In total, 24 patients (16.6 %) manifested at least one episode of FN, of which 41.7 % occurred during the first cycle of treatment. Only a minority of FN patients had clinically significant dose delay or reduction (25.0 % and 12.5 %, respectively). After adjustment with confounders (gender, baseline lymphocyte counts and baseline absolute neutrophil counts), patients with ≥2 comorbidities were at higher risk to develop breakthrough FN (AOR = 4.42, 95 %CI: 1.36–14.40, p = 0.014).
Conclusion
Breakthrough FN is prevalent among elderly cancer patients receiving adjuvant chemotherapy despite G-CSF support, particularly among patients with more than two comorbidities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Febrile neutropenia (FN) is a serious complication of chemotherapy. FN may lead to treatment delays and dose reductions, which may potentially compromise the efficacy of chemotherapy. Patients manifesting FN often require hospitalization and administration of antibiotics. Furthermore, mortality may increase substantially if patients present with concomitant infections, particularly in those who possess multiple co-morbid conditions. Hence, it is prudent to take all precautions to prevent the occurrence of FN, such as judicious usage of granulocyte colony-stimulating factors (G-CSF) prophylaxis. In order to determine the prophylactic strategies of G-CSF, the current guidelines recommend assessing a number of factors to determine the risk of FN. These factors include the myelosuppressive risk of the chemotherapy regimen, patients’ risk factors, patients’ disease status and treatment intent [1–3].
Elderly patients, defined as age equal and above 65 years old, are generally regarded to be more prone to FN and its associated complications due to a decreased metabolism of myelosuppressive drugs, leading to accumulation and subsequent toxicity [4, 5]. Other reasons for increased risk of myelotoxicity in elderly patients include reduced bone marrow function and depletion of hematopoietic stem cell reserves [2, 6, 7]. As such, elderly patients are often candidates for receiving chemotherapy regimens with reduced dose intensity or density, which could potentially compromise treatment efficacy.
G-CSF have been demonstrated to be effective in decreasing the degree and duration of neutrophil nadir, thus decreasing the incidence of FN, mortality and frequency of dose reductions [3, 8]. This was observed across a wide range of malignancies and chemotherapies. There is increasing evidence that elderly patients may also benefit from myelosuppressive regimens especially when they are adequately supported by prophylactic G-CSF. As such, the use of G-CSF as primary prophylaxis in elderly patients undergoing curative chemotherapy with moderate-to-high risk of myelotoxicity is recommended in major guidelines.
Through clinical observations, it has been noted that a proportion of elderly patients may still manifest FN despite receiving prophylactic G-CSF (i.e. breakthrough FN). There is a need to identify clinical characteristics that may predispose elderly patients to breakthrough FN in order for clinicians to improve their supportive care management. Hence, this study was designed to evaluate the prevalence of breakthrough FN among elderly cancer patients receiving myelosuppressive chemotherapy at a cancer center. In addition, we aim to identify patient characteristics that may predispose patients to a higher risk for breakthrough FN.
Methods
Study design
This was a single-center, observational, retrospective cohort study conducted at the National Cancer Centre, Singapore (NCCS). NCCS is the largest ambulatory cancer center in Singapore that treats two-thirds of patients with solid tumors and lymphomas. This study was approved by the Institutional Review Board of NCCS. Patient informed consent was not required in this study.
Patients
All patients 65 years old and above who have completed at least one cycle of myelosuppressive chemotherapy for solid tumors and lymphomas (both Hodgkin’s and non-Hodgkin’s lymphomas) with curative intent (i.e. dose reduction undesired) and received G-CSF as primary prophylaxis were included into the study. In order to be included in the analysis for the impact of FN on chemotherapy delivery, all patients must have completed at least two consecutive cycles of chemotherapy. Patients were excluded if they were receiving growth factors as secondary prophylaxis with chemotherapy (i.e. only after a prior episode of FN). In our institution, antibiotic prophylaxis (such as fluoroquinolones) is not routinely given to patients receiving chemotherapy.
Data collection
A data collection form was developed to collect information on patient demographics, past medical history, pre-treatment laboratory parameters and chemotherapy details. The length of hospitalization, subsequent dose reductions and chemotherapy delays, and treatment given were recorded for every FN episode.
Definitions
FN was defined as a single temperature greater than 38.3 °C or a temperature greater than 38 °C for over an hour and an absolute neutrophil count of <0.5 × 109/L or <1.0 × 109/L and predicted to decline to ≤0.5 × 109/L over the next 48 h [9]. Chemotherapy dose delay was defined as a delay of planned chemotherapy for more than 3 days, and chemotherapy dose reduction was defined as 1 − dose received/dose planned as a percentage [10–12]. A reduction of greater than 15 % was considered clinically significant [10]. In this study, recent surgery indicates surgery performed 3 months or less before or concurrent with chemotherapy while recent radiotherapy (RT) indicates RT given before chemotherapy or intermittently with chemotherapy. In this study, immunologic disorders refer to autoimmune diseases and/or patients who were users of immunosuppressants (besides chemotherapy), while thyroid disorders refer to both hyper- and hypothyroid disorders.
Statistical methods
Descriptive statistics were utilized to summarize patient demographics, disease characteristics, chemotherapy details and the complications of FN such as length of hospitalization stay, chemotherapy dose reductions and delays. Mann–Whitney U test was utilized to compare the dose intensities of chemotherapy between groups. Univariable logistic regression model was utilized to investigate whether patients’ demographics and clinical variables were associated with the incidence of FN. Variables with p value less than 0.2 in the univariable analysis and clinical parameters clinically known to be associated with incidence of FN were included in a multivariable logistic model to investigate if the variables had an independent association. Backward selection was used whereby variables that were not statistically significant (with p > 0.05) were removed from the model. All analyses were performed in SPSS version 20.0. Two-sided p values less than 0.05 were considered statistically significant.
Results
Patient demographics
A total of 145 patients were included in this study, with a total of 704 cycles of chemotherapy being evaluated and each patient received an average of 4.86 cycles. The median age was 69 years old (interquartile range: 66, 74). Majority of the patients were females (64.1 %), Chinese (79.3 %) and had at least two comorbidities (52.4 %). In terms of comorbidities, hypertension (59.3 %) was the most prevalent, followed by hyperlipidemia (37.2 %), cardiovascular disease (22.8 %) and diabetes mellitus (22.1 %).
Among all patients, non-Hodgkin’s lymphoma (54.5 %) and breast cancer (34.5 %) were the most common types of malignancies. Majority of the patients received RCHOP-21 (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone every 21 days, 50.3 %), followed by docetaxel and cyclophosphamide, with or without trastuzumab (16.6 %) and FEC (5-fluorouracil, epirubicin and cyclophosphamide, 6.1 %). Thirty-two percent of the patients had surgery within 3 months of chemotherapy and 4.1 % had recent radiotherapy and chemotherapy (Table 1).
Characteristics of FN patients
Twenty-four patients (16.6 %) developed at least one episode of breakthrough FN of which ten patients had their first FN episode after the first cycle of chemotherapy. One patient had two episodes of FN while another had three episodes of FN despite having received G-CSF prophylaxis for each cycle. Six (25.0 %) FN patients had concurrent infections while four (16.7 %) had open wounds at the time they were admitted for FN. FN patients were hospitalized for a mean number of 5.65 days while 16 patients (66.7 %) received more G-CSF as part of the treatment for FN. There were no significant differences in terms of number of days of hospitalization between those patients who received more G-CSF and those who did not (4.94 ± 1.48 days vs. 7.83 ± 8.08 days, p = 0.42). Six patients (25.0 %) had dose delays of longer than 3 days while only three patients (12.5 %) had dose reductions of more than 15 % in the following chemotherapy cycle after the FN episode (Table 2). There was a statistically significant difference in the median dose intensities between patients who had an FN episode and those who did not (0.87 {0.72, 0.94} vs. 0.96 {0.87, 1.00}, p < 0.05).
Association between clinical characteristics and FN occurrence
Clinical characteristics were investigated for their association with breakthrough FN and were identified by univariate analysis. The results are presented with the odds ratio (OR) and 95 % confidence interval (CI) in Table 3. Characteristics identified by the univariate analysis include: male gender (OR: 3.06, 95 % CI = 1.25–7.50; p = 0.012), having two or more comorbidities (OR: 3.26, 95 % CI = 1.21–8.77; p = 0.015), manifesting cardiovascular disease (OR: 3.81, 95 % CI = 1.51–9.62; p = 0.003), baseline absolute lymphocyte count (ALC) <1.5 × 109/L (OR: 3.94, 95 % CI = 1.41–11.00; p = 0.006) and baseline absolute neutrophil count (ANC) <3.1 × 109/L (OR: 3.21, 95 % CI = 1.11–9.35, p = 0.026) (Table 3).
Several parameters were investigated in the multivariable analysis for associations with breakthrough FN. After adjustment with potential confounders (gender, baseline ANC and ALC), patients with two or more comorbidities were at higher risk to develop breakthrough FN (AOR: 4.42, 95 % CI: 1.36–14.40, p = 0.014) (Table 4).
Discussion
This is the first study to evaluate the prevalence and risk factors associated with breakthrough FN in elderly Asian patients across a wide range of malignancies and myelosuppressive chemotherapy regimens for treatment of solid tumors and lymphomas. To our surprise, despite adherence to current recommendations on primary prophylaxis with G-CSF, a substantial proportion of elderly patients (16.6 %) still experienced FN after chemotherapy. The occurrences of FN have also led to severe complications including dose reduction of chemotherapy as well as hospitalization.
Although elderly patients receiving myelosuppressive chemotherapy are at a higher risk of FN compared to their younger counterparts, current literature (including international guidelines) still advocate the treatment of elderly patients manifesting curable cancers using full-dose chemotherapy in conjunction with G-CSF support. For instance, early stage breast cancer and lymphoma patients constitute over 80 % of the elderly patients in this study, and all patients received chemotherapy with G-CSF routinely per recommendations of international guidelines. It is important to note that a majority of the elderly patients in the community who receive myelosuppressive chemotherapy and require G-CSF support manifest these cancers. As such, patients who manifested varying types of cancer in this study are representative of the real world practice.
Non-Hodgkin’s lymphoma is known to occur more frequently among elderly patients. Typically, over half are diagnosed beyond 60 years old. The International Non-Hodgkin Lymphoma Prognostic Factors Project showed that patients older than 60 years of age had a significantly lower complete response rate and overall survival [13]. The reasons for the poorer treatment outcome in elderly patients are unclear. However, it is understood that elderly patients do not tolerate intensive chemotherapy as well as younger patients, and some studies report that elderly patients have a higher risk of treatment-related mortality. As a result, many clinicians treat elderly patients with reduced dose or less aggressive chemotherapy regimens. In general, these less intensive regimens have used anthracyclines with less cardiotoxicity than doxorubicin, substituted mitoxantrone for doxorubicin, or used short duration weekly therapy. However, less intensive regimens or regimens that do not contain doxorubicin may lead to poorer clinical outcomes. Over the past few years, several trials have evaluated different treatment approaches in older patients with aggressive NHL [14, 15]. The results of these studies suggest that carefully selected elderly patients with good performance status and no significant comorbidities can tolerate aggressive anthracycline-containing regimens as well as younger patients. These patients should be treated initially with full-dose R-CHOP or similar regimens; dosages can be reduced later if severe toxicity occurs. The routine use of hematopoietic growth factors may allow elderly patients to maintain dose intensity.
In an observational study that was conducted by Salar A et al., in the subgroup of patients who received primary prophylaxis with R-CHOP-21, the mean age is 66.2 years old (±12.8), with 32 % of these patients manifesting comorbidities [16]. Interestingly, comparing patients who were receiving primary prophylaxis against those who did not, the incidence of FN were similar (19 % in both groups). However, majority (60 %) of the patients who did not receive primary prophylaxis required reactive G-CSF (either G-CSF secondary prophylaxis or treatment with G-CSF). This stresses that breakthrough FN among elderly may lead to severe infectious consequences that would require severe management with additional growth factor support.
On the other hand, elderly breast cancer patients often receive less myelotoxic chemotherapy (e.g. anthracycline-free regimens such as CMF), and the planned and delivered intensity of chemotherapy may be lower than in younger patients. There is, however, increasing evidence that elderly patients can tolerate standard chemotherapies, provided that they receive appropriate G-CSF support. One study evaluating the use of primary prophylactic G-CSF showed that primary G-CSF prophylaxis does benefit patients above 65 years old. In that study, each additional day of primary prophylactic G-CSF increased the chances for patients to receive more cycles of chemotherapy by 2 % and radiation by 1 % (p < 0.05) [17]. This indicates that the use of growth factors may improve clinical outcomes in breast cancer patients receiving chemotherapy. In another study that evaluates the use of growth factor support in 254 elderly breast cancer patients receiving chemotherapy, the use of pegfilgrastim has greatly reduced the incidence of FN from 24 % to 6 %. This is further implicated by a fewer number of patients experiencing dose delay over 3 days (21 % vs. 14 %) and fewer patients experiencing clinically significant dose reduction (32 % vs. 15 %) [4]. Despite the use of primary prophylactic G-CSF, FN may still occur and cannot be completely eradicated.
It was interesting to us that comorbidities such as cardiovascular diseases had placed our patients at a higher risk for febrile neutropenic events. We were only able to identify one other study that has similarly documented cardiovascular disease as a predictor for FN occurrence [18]. In that study, manifesting cardiovascular diseases brings 2.56 times (95 % CI: 1.04–6.29) higher risk to manifest FN in the predictive model. The degree of association is similarly high in our study. This finding may enable clinicians to better identify elderly patients who are at high risk for breakthrough FN and subsequently provide more protection against FN while they are receiving myelosuppressive chemotherapy. Strategies such as the use of prophylactic antibiotics may be worth exploring. Literature has supported the use of antibiotics to reduce the occurrence of FN among cancer patients manifesting solid tumors and lymphoma. In a randomized, double-blinded, placebo-controlled study, fewer cancer patients experienced febrile episode among those who received levofloxacin prophylaxis, as compared to those who did not receive any prophylaxis (10.8 % vs. 15.2 %, p < 0.001) during chemotherapy [19]. However, elderly patients comprised only one-third of all the included patients, and this study did not allow the planned use of G-CSF. Although the use of antibacterial prophylaxis is deemed appropriate in high risk patients, clinicians are concerned with the increasing occurrence of antibiotic resistance with routine use; furthermore, elderly patients may be more sensitive to side effects of fluoroquinolones (such as QTc prolongation) which may limit the routine use as prophylaxis among elderly patients.
A number of limitations exist in this study. The retrospective nature of this study meant that the information would be only as accurate as what was entered into the various electronic systems and hardcopy medical records of each patient. A number of assumptions were made, such as all FN patients would be admitted to our hospital or at least the record of FN occurrence would be captured in our electronic databases. However, a majority of our patients return to our cancer center for management of cancer or chemotherapy-associated complications, especially when they experience fever and signs of infection such as sore throat, flu-like symptoms and mouth ulcers. Another assumption is that of full compliance to G-CSF being given. Our small sample size may have limited the ability to detect statistical significance for certain risk factors. However, it can still be hypothesis generating. Further studies could be designed to specially evaluate each risk factor which had been identified by the univariate analysis but not the multivariable analysis or to evaluate the prevalence of FN for a specific type of malignancy or chemotherapy.
Conclusions
Despite routine prophylaxis with G-CSF, breakthrough FN is highly prevalent among elderly Asian cancer patients receiving myelosuppressive chemotherapy for solid tumors and lymphomas. The occurrences of FN have also led to severe complications including dose reduction of chemotherapy as well as hospitalization. Furthermore, elderly patients with multiple comorbidities, such as cardiovascular diseases, are at higher risk. Future studies should evaluate potential strategies, including the use of prophylactic antibiotics, to reduce the risk of breakthrough FN in this population.
References
National Comprehensive Cancer Network. Myeloid Growth Factors. www.nccn.org/professionals/physicians_gls/pdf/myeloidgrowth.pdf. Accessed 23 Feb 2013
Aapro MS, Cameron DA, Pettengell R et al (2006) EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphomas and solid tumours. Eur J Cancer 42:2433–2453
Smith TJ, Khatcheressian J, Lyman GH et al (2006) 2006 update of recommendations for the use of white blood cell growth factors: an evidence-based clinical practice guideline. J Clin Oncol 24:3187–3205
Aapro M, Schwenkglenks M, Lyman GH et al (2010) Pegfilgrastim primary prophylaxis vs. current practice neutropenia management in elderly breast cancer patients receiving chemotherapy. Crit Rev Oncol Hematol 74:203–210
Lyman GH, Kuderer NM, Crawford J et al (2011) Predicting individual risk of neutropenic complications in patients receiving cancer chemotherapy. Cancer 117:1917–1927
Aapro M, Crawford J, Kamioner D (2010) Prophylaxis of chemotherapy-induced febrile neutropenia with granulocyte colony-stimulating factors: where are we now? Support Care Cancer 18:529–541
Balducci L, Hardy CL, Lyman GH (2001) Hematopoietic growth factors in the older cancer patient. Curr Opin Hematol 8:170–187
Aapro MS, Bohlius J, Cameron DA et al (2011) 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer 47:8–32
Segal BH, Freifeld AG, Baden LR et al (2008) Prevention and treatment of cancer-related infections. J Natl Compr Canc Netw 6:122–174
Jenkins P, Freeman S (2009) Pretreatment haematological laboratory values predict for excessive myelosuppression in patients receiving adjuvant FEC chemotherapy for breast cancer. Ann Oncol 20:34–40
Chan A, Chen C, Chiang J et al (2012) Incidence of febrile neutropenia among early-stage breast cancer patients receiving anthracycline-based chemotherapy. Support Care Cancer 20:1525–1532
Chan A, Fu WH, Shih V et al (2011) Impact of colony-stimulating factors to reduce febrile neutropenic events in breast cancer patients receiving docetaxel plus cyclophosphamide chemotherapy. Support Care Cancer 19:497–504
The International Non-Hodgkin's Lymphoma Prognostic Factors Project (1993) A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med 329:987–994
Coiffier B, Lepage E, Briere J et al (2002) CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med 346:235–242
Coiffier B, Thieblemont C, Van Den Neste E et al (2010) Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood 116:2040–2045
Salar A, Haioun C, Rossi FG et al (2012) The need for improved neutropenia risk assessment in DLBCL patients receiving R-CHOP-21: findings from clinical practice. Leuk Res 36:548–553
Rajan SS, Stearns SC, Lyman GH et al (2011) Effect of primary prophylactic G-CSF use on systemic therapy administration for elderly breast cancer patients. Breast Cancer Res Treat 130:255–266
Pettengell R, Bosly A, Szucs TD et al (2009) Multivariate analysis of febrile neutropenia occurrence in patients with non-Hodgkin lymphoma: data from the INC-EU Prospective Observational European Neutropenia Study. Br J Haematol 144:677–685
Cullen M, Steven N, Billingham L et al (2005) Antibacterial prophylaxis after chemotherapy for solid tumors and lymphomas. N Engl J Med 353:988–998
Conflict of interest
The authors have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chan, A., Lee, C.P., Chiang, J. et al. Breakthrough febrile neutropenia and associated complications among elderly cancer patients receiving myelosuppressive chemotherapy for solid tumors and lymphomas. Support Care Cancer 21, 2137–2143 (2013). https://doi.org/10.1007/s00520-013-1768-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-013-1768-9