
Abstract
Objectives
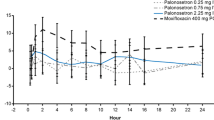
Palonosetron is a novel 5-hydroxytryptamine3 (5 HT3) receptor antagonist, which has been shown to be superior to first generation 5 HT3 receptor antagonists regarding the prevention of acute, delayed and overall chemotherapy-induced nausea and vomiting. First generation 5 HT3 receptor antagonists may induce electrocardiographic changes of heart rate and repolarization. The acute cardiac effect of palonosteron is unknown. The purpose of this study is to determine acute effects of palonosetron on electrocardiographic (ECG) parameters in cancer patients.
Materials and methods
The study had a prospective design. Seventy-six cancer patients with normal cardiac function who received palonosetron for prevention of chemotherapy-induced nausea and vomiting were enrolled. Standard 12-lead ECG recordings were performed at baseline and 30 min after palonosetron administration. P wave durations and corrected QT intervals were measured; P wave dispersion (Pd) and QTc dispersion were calculated.
Results
Median heart rate did not differ among 76 patients enrolled before and after palonosetron administration (p: 0.6). Systolic and diastolic blood pressures were not significantly different before and after palonosteron (p values 0.9 and 0.3, respectively). Although median QT min value was higher after palonosetron administration than before palonosetron administration, the difference was not statistically significant (p: 0.6).
Conclusion
Palonosetron seems to have no acute arrhythmogenic potential.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Chemotherapy-induced nausea and vomiting (CINV) is considered to be the most distressing and debilitating side effect of chemotherapy and can profoundly affect patients' quality of life [1, 2]. Chemotherapeutic agents trigger the process of emesis through activation of multiple neurotransmitter receptors in the vomiting center of the brain, chemoreceptor trigger zone and gastrointestinal tract [3, 4]. Pharmacological treatment of CINV has focused on blocking these receptors using agents such as antihistamines, phenothiazines, benzodiazepins, corticosteroids, 5 HT3 receptor antagonists and neurokinin 1 antagonists [5].
The discovery of selective 5 HT3 receptor antagonists for the prophylaxis and/or treatment of chemotherapy and radiotherapy-induced emesis have been an important advance in oncology [6]. Their antiemetic efficacy has been demonstrated in several clinical trials. Although having an overall excellent safety profile, first generation 5 HT3 receptor antagonists have been reported to induce clinically insignificant or significant electrocardiographic changes and arrhythmias in clinical trials [6–16]. Generally, these changes are most prominent within 1–2 h after a dose of 5 HT3 receptor antagonists and return to baseline within 24 h.
In phase III clinical trials for the prevention of acute, delayed and overall CINV caused by chemotherapeutics of moderate emetic potential, palonosetron, the novel 5 HT3 receptor antagonist, is found to be superior to first generation 5 HT3 receptor antagonists [17, 18]. The improved clinical efficacy of palonosetron may be due, in part, to its more potent binding, longer half-life and unique structural characteristics [17]. These features of palonosetron may lead to different side effects as well. Unlike the first generation of 5 HT3 receptor antagonists, ECG changes and arrhythmias related to palonosetron are unknown.
The surface 12-lead ECG is a noninvasive, practical and safe measurement used to detect drug-induced cardiac adverse effects in most clinical trials [19, 20]. The common parameters used for measuring the arrhythmogenic potential of a drug are P dispersion (Pd), QT interval prolongation and QT dispersion (QTd). These parameters are accurate predictors of drug effects on cardiac repolarization [21]. Prolongation or increased heterogeneity of repolarization is the cause of polymorphic ventricular tachycardia, fibrillation and sudden cardiac death in genetically inherited or acquired forms of long QT syndrome [1]. For example, dolasetron has been shown to increase the QTc interval when given at high doses and the prescribing information for dolasetron and tropisetron carries a cardiovascular warning [1, 22]. Similarly, an increment in mean QTc interval was detected after ondansetron administration [23].
Pd has been used to evaluate the discontinuous propagation of sinus impulses while P max has been used to measure the prolongation of atrial conduction time. It has been reported that prolongation of either P wave or P max duration shows an increased risk for atrial fibrillation [7, 27].
The cardiac safety of ondansetron, granisetron, dolasetron and tropisetron has been investigated in several studies [1, 6–16]. To our knowledge, this is the first clinical trial about the acute effects of palonosetron on ECG parameters. The aim of this prospective study was to determine the acute effects of palonosetron on ECG parameters regarding cardiac depolarization and repolarization.
Materials and methods
Patients
Seventy-six cancer patients with a mean age of 49.5 ± 1.1 years (range 18–72 years) who received emetogenic chemotherapy and used palonosetron for the prevention of acute chemotherapy-induced nausea and vomiting were included in the study. ECG recordings were obtained before and 30 min after palonosteron administration (before chemotherapy), and P wave duration, Pd, QTc and QTd were defined. Pretreatment cardiac evaluation was performed by echocardiography in all patients. The exclusion criteria were a history of and/or documented coronary artery disease, valvular or congenital heart disease, congestive heart failure, cardiac arrhythmias, bundle branch block using drugs that may interfere with cardiac repolarization and comorbidities including diabetes mellitus, hypertension and thyroid disease. The protocol was approved by the ethics committee and all patients gave written informed consent.
Study procedures
All patients were evaluated by clinical examination of vital signs including systolic blood pressure, diastolic blood pressure and heart rate before palonosteron administration. A 12-lead ECG was recorded on all patients just before palonosteron administration. After ECG recordings, all patients were administered an infusion of 8 mg I.V. dexamethasone over 30 min and followed immediately by palonosetron, a single dose of 0.25 mg I.V. administered over 30 s. A second ECG was performed 30 min after the palonosetron administration. After the second ECG recording, the patients were administered chemotherapy. The ECG recordings were evaluated by the same cardiologist who was blinded to the clinical status of the patient and the timing of ECG recording.
The onset of the P wave was defined as the point of the first visible upward departure of the trace from the bottom of the baseline. The return to the baseline of the bottom of the trace in wave was considered to be the end of the P wave. P max in any of the 12-lead surface ECGs was measured and used as a marker of prolonged atrial conduction time. P wave dispersion was defined as the difference between the longest P wave duration (P max) and the shortest P wave duration (P min) recorded from multiple surfaces ECG leads [24, 25]. P wave dispersion, detected from the surface ECG, has been thought to reflect left atrial enlargement and altered conduction. P wave dispersion and P wave maximal duration reflects the activation of atrial muscle and may depend primarily upon the mass of tissue excited, which have been used in the assessment of the risk for atrial fibrillation. The clinical significance of P wave duration has been demonstrated in many clinical conditions, especially in paroxysmal atrial fibrillation [25–27].
The QT was defined as the interval from the beginning of the QRS complex to the end of the T wave, and QTc is the QT interval corrected for the heart rate calculated from the ECG by the Bazett Formula [28]. The longest QT duration (QT max) and the shortest QT duration (QT min) were identified. They were corrected according to heart rate by using the Bazett Formula and defined as QTc max and QTc min. QTd was calculated as the difference between the longest and shortest QTc intervals, measured in each of the 12 ECG leads.
P-wave duration, QT and RR intervals were measured. Pd and QTd were calculated. Baseline and follow-up measurements were compared.
Statistical analysis
The results were analyzed with the SPSS statistical software package (version 13.0, SPSS, Chicago, IL, USA). The data were expressed as mean ± standard deviation and interquartile range where appropriate. Statistical comparison of quantitative data was performed by paired sample t-test. A p value of <0.05 was considered as statistically significant.
Results
Median heart rate did not differ among 76 patients enrolled before and after palonosetron administration (p: 0.6). Systolic and diastolic blood pressures were not significantly different before and after palonosteron (p values 0.9 and 0.3, respectively). Table 1 demonstrates the comparative heart rate and blood pressure measurements before and after palonosetron administration. Although median QT min value was higher after palonosetron administration than before palonosetron administration, the difference was not statistically significant (p: 0.6). Comparative ECG parameters obtained before and 30 min after palonosetron administration are given in Table 2.
Discussion
Prevention and/or treatment of CINV, for which the 5 HT3 receptor antagonists are currently regarded as the gold standard, are important in the management of cancer patients. The use of 5 HT3 receptor antagonists may lead to some cardiac side effects related to repolarization. Electrophysiological effects 5 HT3 receptor antagonists including ondansetron, granisetron, dolasetron and tropisetron on ECG parameters were investigated in detail [1, 3, 4, 7, 8, 13–15]. However, the data about acute effects of palonosetron on ECG parameters is lacking in the literature. In this prospective study, we demonstrated that palonosetron has no significant effects on cardiac repolarization.
The studies investigating the cardiac side effects of 5 HT3 receptor antagonists are carried out in both healthy subjects [14, 15, 29, 30] and cancer patients [1, 6–8]. Boike et al. compared the cardiovascular effects of granisetron (10 μg/kg, I.V. over 30 s or 5 min) and ondansetron (32 mg, I.V. over 15 min) in a placebo-controlled trial in healthy adults without any cardiac abnormalities [14]. They reported that there were no clinically important changes among the two administration protocols of granisetron versus ondansetron or of granisetron versus placebo in healthy adults. Although the mean postdose QTc interval was significantly longer for ondansetron, it was not statistically meaningful. In a single-blinded study designed by Benedict et al. [29], effects of ondansetron were compared with those of dolasetron mesylate. Thirty healthy male volunteers received single doses of I.V. dolasetron mesylate (1.2 mg/kg, 1.8 mg/kg and 2.4 mg/kg), ondansetron (32 mg) and placebo. The changes in ECG intervals of dolasetron mesylate or ondansetron were acute, asymptomatic and transient. Dolasetron mesylate caused significant dose-related increases in heart rate and PR and QRS intervals within 4 h of administration. However, ondansetron caused a decrease in heart rate and increase in JT interval. Both ondansetron and dolasetron mesylate (2.4 mg/kg) increased QTc interval. Dolasetron mesylate predominantly altered the ECG parameters related to ventricular repolarization (QRS duration), whereas ondansetron predominantly affected ventricular depolarization as measured by the prolongation in the JT interval. All of these changes returned to baseline within 8 h of treatment.
Acute cardiac side effects of tropisetron were also reported in a study [7]. In this study, it was shown that tropisetron did not have any ventricular or atrial arrhythmogenic effect measured by P max, P min, P dispersion, QTc max, QTc min and QTd. However, it was found that tropisetron may cause a slight decrease in heart rate.
In many studies primarily designed to compare the antiemetic efficacy of different 5 HT3 receptor antagonists, cardiac side effects were also compared. In a multicenter study [12], in the patients who used high dose cisplatin (≥80 mg/m2), single I.V. doses of dolasetron mesylate (1.8 mg/kg or 2.4 mg/kg) and granisetron (3 mg) were compared. Regarding the antiemetic efficacy, both dosages of dolasetron mesylate and granisetron were found to be equally effective. Among the three treatment groups, QRS duration was not differently significant, whereas both PR and QTc intervals were significantly increased in patients in the dolasetron group after 1–2 h of drug administration. No significant difference was observed among the treatment groups at 24 h of treatment. In our study, in order to eliminate additional effects of chemotherapeutic agents on ECG parameters, we obtained ECG recordings 30 min after palonosetron administration just before chemotherapy. We are aware of the fact that this lag period may be inadequate to observe some effects of palonosetron on ECG changes.
In a study designed by Lofters et al., the efficacy and the adverse effects of dolasetron mesylate and ondansetron were compared [31]. ECG changes were observed in both groups of patients, but were significantly more common in dolasetron-treated patients. QTc and QRS interval prolongation were the most frequently encountered ECG changes. Nonetheless, all ECG changes were asymptomatic and none required treatment.
In this study, we hypothesized that due to its different structure and affinity to 5 HT3 and cardiac ion receptors, palonosetron may have unique effects on cardiac repolarization. Voltage-dependent Na+ and K+ channels are important determinants of the ECG [32]. The drugs that block K channels may induce QT prolongation, while the drugs that block Na+ channels may produce QRS widening. It was demonstrated that human cardiac Na+ channels are blocked by granisetron, ondansetron and dolasetron in a concentration-dependent manner (kuryshev), meaning that 5 HT3 receptor antagonists may lead to cardiac repolarization problems. In fact, 5 HT3 receptor antagonists have also been reported to widen the QRS complex and prolong JT, QT and PR intervals [6, 14, 29]. Accordingly, it was shown that dolasetron may prolong QRS by 5 to 20%, and ondansetron may increase QT and JT intervals by 2 to 5% [14, 15, 29].
The frequency of cardiac ion channel blockage is related to the accumulation of drug-bound inactivated channels, which is related to drug serum. Significant delays in cardiac repolarization have been observed with 5 HT3 receptor antagonists at doses higher than those required to block 5-HT3 receptors. In our study, we did not encounter any cardiac repolarization problems with palonosetron. Given the higher 5 HT3 receptor affinity of palonosetron, the drug may induce antiemesis within lower serum concentration limits, yet not high enough for cardiac ion channel blockage, therefore, having less cardiac side effects within therapeutic concentration, when compared to other 5 HT3 receptor antagonists. In conclusion, our study disclosed that palonosetron has no acute arrhythmogenic effect related to cardiac repolarization.
References
Aapro M, Bourke JP (2003) Rapid intravenous administration of granisetron prior to chemotherapy is not arythmogenic: results of a pilot study. Eur J Cancer 39:927–931
O'Brien BJ, Rusthoven J, Rocchi a et al (1993) Impact of chemotherapy-induced nausea and vomiting on patients' functional status and on costs: survey of five Canadian centers. Can Med Assoc J 149:296–302
Navari RM (2003) Pathogenesis-based treatment of chemotherapy-induced nausea and vomiting-two new agents. J Support Oncol 1:89–103
De Leon A (2006) Palonosetron (Aloxi): a second-generation 5-HT3 receptor antagonist for chemotherapy-induced nausea and vomiting. Bayl Univ Med Cent Proc 19:413–416
Doherty KM (1999) Closing the gap in prophylactic antiemetic therapy: patient factors in calculating the emetogenic potential of chemotherapy. Clin J Oncol Nurs 3:113–119
Jantunen IT, Kataja VV, Muhonen TT, Parviainen T (1996) Effects of granisetron with doxorubicin or epirubicin on ECG intervals. Cancer Chemother Pharmacol 37:502–504
Yavas O, Yazici M, Eren O, Boruban C, Artac M, Genc M (2008) The acute effect of tropisetron on ECG parameters in cancer patients. Support Care Cancer 16:1011–1015
Buyukavci M, Olgun Hi Ceviz N (2005) The effects of ondansetron ang granisetron on electrocardiography in children receiving chemotherapy for acute leukemia. Am J Clin Oncol 28:201–204
Navari RM, Koeller JM (2003) Electrocariographic and cardiovascular effects of the 5-hydroxitryptamine 3 receptor antagonists. Ann Pharmocother 37:1276–1286
Watanabe H, Hasegawa A, Shinozaki T et al (1995) Possible cardiac side effects of granisteron an entiemetic agent, in patients with bone and soft-tissue sarcomas receiving cytotoxic chemotherapy. Cancer Chemother Pharmacol 35:278–282
Kasinath NS, Malak O, Tetzlaff J (2003) Atrial fibriallation after ondansetron for the prevention and treatment of postoperative nausea and vomiting a case report. Can J Anaesth 50:229–231
Audhuy B, Cappelaere P, Martin M et al (1996) A double-blind, randomized comparison of the antiemetic efficacy of two intravenous doses of dolasetron mesilate and granisetron in patients receiving high dose cisplatin chemotherapy. Eur J Cancer 32A(5):807–813
Ballard HS, Bottino G, Bottino J (1992) Ondansetron and chest pain. Lancet 340(8827):1107
Boike SC, Ilson B, Zariffa N et al (1997) Cardiovascular effects of i.v. granisetron at two administration rates and of ondansetron in healthy adults. Am J Health Syst Pharm 54(10):1172–1176
Hunt TL, Cramer M, Shah A et al (1995) A double-blind placebo-controlled, dose-ranging safety evaluation of single-dose intravenous dolasetron in healthy male volunteers. J Clin Pharmocol 35(7):705–712
Hesketh P, Navari R, Grote T et al (1996) Double-blind, randomized comparison of the antiemetic efficacy of intravenous dolasetron mesylate and intravenous ondansetron in the prevention of acute cisplatin-induced emesis in patients with cancer. Dolasetron Comparative Chemotherapy-induced Emesis Prevention Group. J Clin Oncol 14(8):2242–2249
Eisenberg P, Figueroa-Vadillo J, Zamora R, Charu V, Hajdenberg J, Cartmell A, Macciocchi A, Grunberg S (2003) Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer 98:2473–2482
Gralla R, Lichinitser M, Van Der Vegt S, Sleeboom H, Mezger J, Peschel C, Tonini G, Labianca R, Macciocchi A, Aapro M (2003) Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol 14:1570–1577
Morganroth J (2007) Cardiac repolarization and the safety of new drugs defined by electrocardiography. Clin Pharmacol Ther 81(1):108–113
Morganroth J (2001) Focus on issues in measuring and interpreting changes in the QTc interval duration. Eur Heart J 3:105–111
Morganroth J (2007) Evaluation of the effect on cardiac repolarization (QTc interval) of oncologic drugs. Ernst Schering Res Found Workshop 59:171–184
Kris MG, Grunberg SM, Gralla RJ et al (1994) Dose-ranging evaluation of the serotonin antagonist dolasetron mesylate in patients receiving high-dose cisplatin. J Clin Oncol 12:1045–1049
Lifsey DS, Gralla RJ, Clark RA, Kline RC (1993) Electrocardiographic changes with serotonin antagonist antiemetics:rate of occurrence and clinical relevance. Proc Am Soc Clin Oncol 12:463, abst 1611
Gialafos JE (1999) P-wave dispersion. Eur Heart J 20(4):317
Dilaveris PE, Gialafos EJ, Sideris SK, Theopistou AM, Andrikopoulos GK, Kyriakidis M, Gialafos JE et al (1998) Simple electrocardiographic markers for the prediction of paroxysmal idiopathic atrial fibrillation. Am Heart J 135:733–738
Dilaveris PE, Gialafos EJ, Andrikopoulos GK, Richter DJ, Papanikolaou V, Poralis K, Gialafos JE (2000) Clinical and electrocardiographic predictors of recurrent atrial fibrillation. Pacing Clin Electrophysiol 23:352–358
Bitzen A, Sternickel K, Lewalter T, Schwab JO, Yang A, Schrickel JW, Linhart M et al (2007) Automatic p wave analysis over 24 hours in patients with paroxysmal or persistent atrial fibrillation. Ann Noninvasive Electrocardiol 12:306–315
Bazzet HR (1920) An analysis of the time relations of electrocardiographs. Heart 7:353–370
Benedict CR, Arbogast R, Martin L, Patton L, Morrill B, Hahne W (1996) Single-blind study of the effects of intravenous dalasetron mesylate versus ondansetron on electrocardiographic parameters in normal volunteers. J Cardiovasc Pharmacol 28:53–59
Gray GW, McLellan TM, Ducharme MB (1996) Granisetron shows no pro-arrhythmic effect in normal subjects during or after exercise in a hot environment. Aviat Space Environ Med 67(8):759–761
Lofters WS, Pater JL, Zee B et al (1997) Phase III double-blind comparison of dolasetron mesylate and ondansetron and an evaluation of the additive role of dexamethasone in the prevention of acute and delayed nausea and vomiting due to moderately emetogenic chemotherapy. J Clin Oncol 15(8):2966–2973
Kuryshev YA, Brown AM, Wang L, Benedict CR, Rampe D (2000) Interactions of the 5-hydroxytryptamine 3 antagonist class of antiemetic drugs with human cardiac ion channels. J Pharmacol Exp Ther 295(2):614–620
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yavas, C., Dogan, U., Yavas, G. et al. Acute effect of palonosetron on electrocardiographic parameters in cancer patients: a prospective study. Support Care Cancer 20, 2343–2347 (2012). https://doi.org/10.1007/s00520-011-1348-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-011-1348-9