
Summary
Background
The goal of this study was to compare outcomes of patients with severe traumatic brain injury (TBI) who had been admitted either during workdays from 7 a.m. to 7 p.m. (“regular service”) or during any other time (“on-call service”).
Material and methods
Between March 2002 and April 2012, 17 Austrian centers enrolled TBI patients into two observational studies that focused on effects of guideline compliance (n = 400) and on prehospital and early hospital management (n = 777), respectively. Data on trauma severity, clinical status, treatment, and outcomes were collected prospectively. All patients with severe TBI (Glasgow Coma Scale score < 9) were selected for this analysis. Secondary transfers and patients with unsurvivable injuries were excluded. The International Mission for Prognosis and Analysis of Clinical Trials in TBI core model was used to estimate probabilities of hospital death and unfavorable long-term outcome (Glasgow Outcome Scale score < 4). Based on time of arrival, patients were assigned to groups “regular service” or “on-call service.”
Results
Data from 852 patients were analyzed (413 “regular,” 439 “on-call service”). “On-call” patients were younger (45 vs. 51 years, P < 0.001) and had a higher rate of alcohol intoxication (41 vs. 11 %, P < 0.001). Trauma severity was comparable; the probabilities of death and unfavorable outcome were identical. There were no differences regarding computed tomography findings or treatment. Hospital mortality (24 vs. 28 %, P = 0.191) and rate of patients with unfavorable outcome at 6 months (43 vs. 48 %, P = 0.143) were comparable.
Conclusions
In Austria, the time of hospital admission has no influence on outcomes after severe TBI.
Zusammenfassung
Grundlagen
Das Ziel dieser Studie war, die Behandlungsergebnisse von Patienten mit schwerem Schädelhirntrauma (SHT) zu vergleichen, die entweder an Werktagen zwischen 07.00 und 19.00 Uhr (“regulärer Dienst”; „RD“) oder zu irgendeiner anderen Zeit (“Bereitschaftsdienst“, „BD“) eingeliefert wurden.
Methodik
Zwischen 3/2002 und 4/2012 rekrutierten 17 österreichische Zentren Patienten mit SHT für 2 Beobachtungsstudien, die den Effekt einer Richtlinien-konformen Behandlung (n = 400) bzw. die Ergebnisse einer besseren Erstversorgung (n = 777) untersuchten. Angaben zu Verletzungsschwere, klinischem Status, Therapie und Behandlungsergebnis wurden prospektiv erhoben. Alle Patienten mit schwerem SHT (Glasgow Coma Scale score < 9) wurden für diese Analyse ausgewählt. Sekundäre Transferierungen und Patienten mit nicht überlebbaren Verletzungen wurden exkludiert. Das IMPACT Core Model wurde verwendet, um die Wahrscheinlichkeit von Tod im Krankenhaus und von ungünstigem Langzeitergebnis (definiert als Glasgow Outcome Scale score < 4 nach 6 Monaten) abzuschätzen. Je nach Zeitpunkt der Einlieferung wurden die Patienten der Gruppe „RD“ oder „BD“ zugeteilt. Demografische Daten, Verletzungsschwere, Therapie und Behandlungsergebnisse wurden mittels Chi2-Test, T-Test, und logistischer Regression verglichen.
Ergebnisse
852 Datensätze waren verfügbar (413 “RD”, 439 “BD”). “BD”-Patienten waren jünger (45 vs. 51 Jahre, P < 0.001) und waren häufiger alkoholisiert (41 vs. 11 %, P < 0.001). Die Verletzungsschwere war vergleichbar, die Wahrscheinlichkeiten von Tod und von ungünstigem Behandlungsergebnis waren identisch. Es fanden sich keine Unterschiede hinsichtlich CT-Diagnosen und Behandlung. Spitalsmortalität (24 vs. 28 %, P = 0.191) und Prozentsatz der Patienten mit ungünstigem Langzeitergebnis (43 vs. 48 %, P = 0.143) waren vergleichbar.
Schlussfolgerungen
In Österreich hat der Zeitpunkt der Einlieferung ins Krankenhaus keinen signifikanten Einfluss auf die Behandlungsergebnisse von Patienten mit schwerem SHT.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Traumatic brain injury (TBI) is a major cause of morbidity and mortality, and is the leading cause of death in people aged 15–45 years [1]. Tagliaferri et al. [2] reported that TBI accounted for the majority of trauma deaths in Europe. It is generally agreed that patients with TBI should be treated without unnecessary delay to avoid secondary brain insults. Some studies have shown that trauma patients admitted during the night shift or on weekends have worse outcomes than those admitted during the day shift or on weekdays: Egol et al. [3] reported that patients admitted between midnight and 6 a.m. had a significantly higher risk for in-hospital mortality, and another study showed that TBI patients admitted at night had a significantly longer interval between hospital admission and surgery [4]. Other studies, however, found no significant effect of time of admission [5, 6], and one study reported lower mortality of trauma patients admitted on weekends [7].
There are two key factors that may influence outcomes of patients who are admitted during the night or on holidays: due to reduced staffing, fewer physicians, nurses, and technicians may be available, which might cause some delay of treatment, and fatigue may become a problem, as almost all physicians work 24-h shifts. The goal of this study was to analyze the effects of the time of hospital admission on outcomes in a sample of patients with severe TBI that had been collected prospectively over the past 10 years. Our hypothesis was that patients who were admitted during the night shift or on holidays/weekends would have higher rates of hospital death and unfavorable long-term outcome compared with patients who arrived on weekdays.
Patients and methods
Between 2001 and 2012, the International Neurotrauma Research Organization (INRO, a nongovernmental research organization, founded in 1999; based in Vienna, Austria) coordinated two projects that focused on Austrian patients with TBI. Both projects were purely observational and enrolled pediatric as well as geriatric patients, TBI patients with multiple trauma, and patients with low Glasgow Coma Scale (GCS) scores. The first project analyzed epidemiology and hospital treatment of patients with severe TBI as well as the effects of guideline-based treatment [8]. This project started in March 2002; five centers enrolled 400 patients until June 2005. The second project focused on prehospital and early hospital management of patients with moderate and severe TBI. It started in March 2009; 16 centers enrolled 777 patients until April 2012. Both projects were done with approval of the local ethical committees. Due to the purely observational design of the projects, informed consent of the patients was not mandatory; however, all patients who recovered sufficiently to consent gave written permission to use their data for scientific purposes.
The data were collected in 17 Austrian centers. Of these centers, 13 were “high-volume” centers: 4 free-standing trauma hospitals, 2 University departments of Traumatology, and 7 large trauma departments in tertiary hospitals. The four remaining centers were “low-volume” centers; they included three trauma departments in regional hospitals and one smaller trauma hospital. All centers were able to provide state-of-the-art patient management. The number of patients enrolled by these centers (median: 50, interquartile range (IQR): 29-101, range: 12–163) varied considerably, as 4 “high volume” centers participated in both projects, and some centers joined the second project with just few months remaining for patient inclusion. Using the prognostic International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) core model [9], the observed vs. expected mortality ratio was < 1 for 16 of 17 centers (median: 0.85, IQR: 0.67–0.95, range: 0.59–1.09)—this confirms that the centers provided high-quality treatment.
Treatment in the field was provided by emergency physicians. All patients had rapid examination including documentation of vital signs (GCS score, pupillary status, blood pressure, heart rate, and oxygen saturation). Rapid sequence intubation facilitated by hypnotics and relaxants, ventilation, treatment of hemorrhage, and fluid resuscitation were done as appropriate. After admission, each patient was examined by a trauma team (anesthesiologists, trauma surgeons, and/or neurosurgeons, radiologists, nurses), and a computed tomography (CT) scan was done. The patients then underwent surgery as appropriate and/or were admitted to the intensive care unit (ICU). Neurosurgery was provided by neurosurgeons (6 centers) or by trauma surgeons (11 centers) who had the option of consulting neurosurgeons for more difficult cases. In a previous study, we have shown that the specialty of the surgeon had no impact on outcomes of the patients [10]. Intensive care was provided by anesthesiologists in cooperation with neurosurgeons or trauma surgeons.
A database developed by INRO was used to collect data. Basic demographic data of the patient, cause and location of trauma, prehospital status and treatment, mechanism and severity of trauma (Abbreviated Injury Score [AIS], Injury Severity Score [ISS]), results of CT scans, results of laboratory testing, and data on surgical procedures and outcomes were recorded prospectively. Prehospital data were documented by paramedics, and were then transferred into the databases. CT scans were interpreted by neurosurgeons, trauma surgeons, and radiologists, and the summarized findings were entered into the CT page of the database. This CT page collected detailed data on basal cisterns, midline shift, and main findings. Data on duration of various treatments, complications, and outcomes were collected at discharge from the ICU and at hospital discharge. Information on status and location was recorded at 6 months after injury. This was done by phone calls to the patients and/or their relatives; in some cases, the Glasgow Outcome Scale (GOS) score was recorded at patients’ follow-up visits to the centers. In all centers, data were collected by local investigators; data quality was monitored by the INRO project manager (Alexandra Brazinova). Missing or implausible data were reported to local investigators who then submitted missing or corrected values. Personal data protection was observed, and the identifiers were kept separately from the data.
All patients who had severe TBI (defined as AIS “head” > 2 and/or enrollment GCS score < 9) were selected for this analysis. Patients with unsurvivable injuries (AIS “head” = 6) and those who had been transferred from another hospital were excluded. Data on trauma mechanism, trauma severity, CT findings, treatment, and outcomes were retrieved for each patient. The IMPACT core model [9] was used to estimate the probabilities of hospital death and unfavorable long-term outcome. This model has been validated for our patient sample. To describe long-term outcomes, the GOS [11] was used. “Favorable outcome” was defined as a GOS score of 5 or 4; “unfavorable outcome” was defined as a GOS score of 3 or less at 6 months after trauma.
Based on the time of arrival at the center, patients were assigned to group “regular service” (arrival at workdays from 7 a.m. to 7 p.m.) or to group “on-call service” (arrival at any other time). In the centers that participated in the TBI projects, minimum in-house staffing during “on-call service” included two surgeons, one anesthesiologist, one radiologist, two surgical nurses, one anesthesia nurse, one radiology technician, and one to two paramedic assistants. Depending on the size of the center, other surgical specialists would be available either from in-house departments, or from other hospitals. During “regular service,” the teams could be considerably larger. Physicians usually worked 24-h shifts, and all others worked 12-h shifts.
Demographic data, clinical status, treatment, and outcomes of these two groups were compared. In addition, demographic and treatment data were analyzed, and rates of mortality and unfavorable outcomes were calculated for the following groups:
-
admission between midnight and 6 a.m. vs. admission between 6 a.m. and midnight,
-
admission on workdays vs. admission on holidays/weekends (including the nights),
-
admission between 7 a.m. and 7 p.m. (day) vs. admission between 7 p.m. and 7 a.m. (night),
-
admission during the night (7 p.m. to 7 a.m.) vs. admission on workdays (7 a.m. to 7 p.m.) vs. admission on holidays/weekends (7 a.m. to 7 p.m.).
Statistical analysis
Our sample was large enough (power = 0.83) to detect a small effect (d = 0.2) at a significance level of 0.05. Two-tailed t-test (for comparisons of mean values), Fisher’s exact test, and chi-square test (for analysis of 2 × N contingency tables) were done as appropriate to identify differences between the groups. To check for associations with outcomes, we constructed logistic regression models for hospital death and unfavorable long-term outcome, where the effects of time of admission on outcomes were corrected for age, GCS scores, and ISS. Data are presented as means with standard deviations, or as proportions. A P-value of < 0.05 was considered statistically significant.
Results
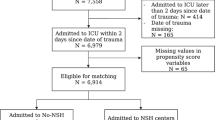
Of the 1,177 patients in the database, 202 patients had been transferred from another hospital, 74 had an unsurvivable injury (AIS “head” = 6), and 49 had only moderate TBI (AIS “head” < 3 and GCS score > 8 at enrollment). This left 852 patients with severe TBI for analysis. Of these, 413 arrived on a workday between 7 a.m. and 7 p.m. (“regular service” group), and 439 arrived at another time (holiday, weekend, night; “on-call service” group).
Demographic data, data on status, and data on trauma severity are given in Table 1. “On-call” patients were significantly younger. Patients aged between 15 and 34 years were significantly more likely to be admitted during “on-call service” (Fig. 1); patients from all other age groups were more likely to be admitted during “regular service.” “On-call” patients had a significantly higher rate of alcohol intoxication (Table 1) and had different trauma mechanisms (fewer falls, more motor vehicle accidents, and more motorbike accidents). Trauma severity was comparable; AIS “head,” ISS, GCS score, rates of hypoxia and hypotension, and pupillary reactivity were not different. The probabilities of death and unfavorable outcome were almost identical.

Percentages of cases admitted during “regular service” and “on-call service” vs. age groups (years)
With regard to treatment (Table 2), the rate of helicopter transport was significantly lower in “on-call” patients because Austrian rescue helicopters usually do not fly missions after dark. All other treatment variables were not different. The intervals between admission and CT scan and between admission and start of neurosurgery (if required) were comparable. There were no differences regarding CT scan findings (Table 2). The causes of death (Table 2) were not different. Hospital mortality and rate of patients with unfavorable outcome at 6 months were lower in the “on-call” group, but this difference was not significant.
Table 3 gives an overview of the rates of hospital deaths and unfavorable outcome at 6 months for groups with different admission times. Patients who arrived between midnight and 6 a.m. had lower hospital mortality, and had a significantly lower rate of unfavorable outcome. The same pattern was found for patients who arrived during the night shift vs. during the day shift. No significant differences were found for all other comparisons. For all comparisons, patients who arrived during the night shift or during holidays/weekends were significantly younger, were more likely to test positive for blood alcohol, and had different trauma mechanisms.
The multivariate analysis (Table 4) showed that only age, ISS, and first GCS score were significantly associated with outcomes; after correction for these factors, alcohol intoxication had no significant effect.
Discussion
This study presents an analysis of the effects of the time of hospital admission for Austrian patients with severe TBI who had direct transport to the participating centers and had survivable injuries. We choose to compare “on-call service” to “regular service” in detail because the influence of both reduced staffing and fatigue was expected to be found in the “on-call” patients. However, we found that “on-call” service was adequate because the time of admission had no significant effect on hospital mortality and on the rate of unfavorable outcome at 6 months after trauma. The guidelines of the Austrian Society of Traumatology state that all departments admitting severe trauma cases must have at least one full trauma team available 24/7 to care for these patients. Thus, limitation of service during “on-call” times does not affect treatment of severe cases (but may affect patients with minor injuries, e.g., by longer intervals between admission and treatment). This study also found no effects of fatigue. Our hypothesis has been proven wrong.
This study confirms previous findings from Guly et al. [6]: this British group used data from Trauma Audit and Research Network (3 years, 40,866 cases) and reported that 31.1 % of trauma patients with an ISS > 15 who were admitted “out of hours” died, compared with 33.5 % of patients who were admitted inside “working hours.” Similar results have been reported by Carmody et al. [5]: this group from California reviewed 8,015 consecutive trauma admissions (3 years) and found that mortality of trauma patients admitted at night was significantly lower than that of patients admitted during the day (10.1 vs. 13.1 %). They performed different comparisons (e.g., morning vs. night for all patients, for blunt trauma, for penetrating trauma, weekday vs. weekend, and weeknight vs. weekend night) and found no significant differences in ISS-matched mortality rates. A recent study by Carr et al. [7] used data from the Pennsylvania trauma system (5 years, 90,461 cases) and reported that patients who arrived on weeknights were more likely to die than patients who arrived on weekdays (unadjusted mortality: 7.5 vs. 6.6 %). In the adjusted analysis, there was no significant difference in mortality between weekday and weeknight admissions, and patients who arrived on weekends were less likely to die than those who arrived on weekdays (odds ratio (OR): 0.89; 95 % confidence interval (CI): 0.81–0.97). None of these three articles reported data on staffing.
Other authors reported different results. Egol et al. [3] used 2002–2006 data from the US National Trauma Data Bank and analyzed outcomes of 601,388 patients aged > 18 years. They found that cases admitted between midnight and 6 a.m. were significantly more likely to die (OR: 1.18; 95 % CI: 1.12–1.25, adjusted analysis). This pattern was found in all trauma centers, but was weakest at level 1 trauma centers and strongest at level 3 and 4 trauma centers. This article did not report data on staffing.
All studies discussed so far included all trauma patients, while our study included only patients with severe TBI. There is only one study that also focused on TBI patients [4]; it showed that patients who arrived between 6 p.m. and 8 a.m. had significantly longer intervals between admission and start of neurosurgery; no data on staffing were given. In our study, however, there were no differences regarding the intervals admission to CT scan and admission to neurosurgery.
What are the possible reasons for the small outcome differences observed in our study? The differences in mortality and unfavorable outcome were most pronounced in all analyses that included periods after 7 p.m. No differences were observed for patients who were admitted during weekends or holidays between 7 a.m. and 7 p.m. There were no differences in treatment, and only age and rate of alcohol intoxication were significantly different. Age is one of the most important factors influencing outcomes after TBI as demonstrated in the large study done by Hukkelhoven et al. [12] and by a number of other studies. The significant effect of age has been confirmed by our results. In addition to the factor “age,” it seems possible that “alcohol intoxication” may be responsible for the small difference in outcomes. There is evidence that alcohol intoxication may be beneficial for patients with moderate and severe TBI [13, 14]. Suggested mechanisms for this beneficial effect include a reduction of the neuroinflammatory response to TBI [15] and a decrease in pneumonia rate after TBI [16].
Conclusions
The study analyzed hospital mortality and long-term outcome of patients admitted either during workdays (regular service) or during holidays/weekends and nights (“on-call service”). “On-call” patients were younger and were more likely to have positive blood alcohol levels. There were no differences in trauma severity or treatment. Timing of hospital admission had no effect on outcomes, although mortality and rate of unfavorable outcomes were insignificantly lower in “on-call” patients.
References
Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341–53.
Tagliaferri F, Compagnone C, Korsic M, Servadei F, Kraus J. A systematic review of brain injury epidemiology in Europe. Acta Neurochir (Wien). 2006 Mar;148(3):255–68. Discussion 268.
Egol KA, Tolisano AM, Spratt KF, Koval KJ. Mortality rates following trauma: the difference is night and day. J Emerg Trauma Shock. 2011 Apr;4(2):178–83.
Kim YJ. Night admission to the emergency department: a factor delaying time to surgery in patients with head injury. J Clin Nurs. 2010 Oct;19(19–20):2763–70.
Carmody IC, Romero J, Velmahos GC. Day for night: should we staff a trauma center like a nightclub? Am Surg. 2002 Dec;68(12):1048–51.
Guly HR, Leighton G, Woodford M, Bouamra O, Lecky F. The effect of working hours on outcome from major trauma. Emerg Med J. 2006 Apr;23(4):276–80.
Carr BG, Reilly PM, Schwab CW, Branas CC, Geiger J, Wiebe DJ. Weekend and night outcomes in a statewide trauma system. Arch Surg. 2011 Jul;146(7):810–7.
Rusnak M, Janciak I, Majdan M, Wilbacher I, Mauritz W. Severe traumatic brain injury in Austria VI: effects of guideline-based management. Wien Klin Wochenschr. 2007 Feb;119(1–2):64–71.
Steyerberg EW, Mushkudiani N, Perel P, Butcher I, Lu J, McHugh GS, et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 2008 Aug 5;5(8):e165. Discussion e165.
Leitgeb J, Mauritz W, Brazinova A, Matula C, Majdan M, Wilbacher I, et al. Outcome of patients with severe brain trauma who were treated either by neurosurgeons or by trauma surgeons. J Trauma Acute Care Surg. 2012 May;72(5):1263–70.
Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975 Mar 1;1(7905):480–4.
Hukkelhoven CW, Steyerberg EW, Rampen AJ, Farace E, Habbema JD, Marshall LF, et al. Patient age and outcome following severe traumatic brain injury: an analysis of 5600 patients. J Neurosurg. 2003 Oct;99(4):666–73.
Salim A, Teixeira P, Ley EJ, DuBose J, Inaba K, Margulies DR. Serum ethanol levels: predictor of survival after severe traumatic brain injury. J Trauma. 2009 Oct;67(4):697–703.
Berry C, Salim A, Alban R, Mirocha J, Margulies DR, Ley EJ. Serum ethanol levels in patients with moderate to severe traumatic brain injury influence outcomes: a surprising finding. Am Surg. 2010 Oct;76(10):1067–70.
Goodman MD, Makley AT, Campion EM, Friend LA, Lentsch AB, Pritts TA. Preinjury alcohol exposure attenuates the neuroinflammatory response to traumatic brain injury. J Surg Res. 2013 Oct;184(2):1053–8.
Hadjibashi AA, Berry C, Ley EJ, Bukur M, Mirocha J, Stolpner D, et al. Alcohol is associated with a lower pneumonia rate after traumatic brain injury. J Surg Res. 2012 Apr;173(2):212–5.
Acknowledgments
We are very grateful to the investigators from the participating centers who enrolled patients and collected data: H. Artmann MD (Schwarzach), N. Bauer MD (Linz UKH), F. Botha MD (Linz WJ), F. Chmeliczek MD (Salzburg LKA), G. Clarici MD (Graz Uni), D. Csomor MD (Wr. Neustadt), R. Folie MD (Feldkirch), R. Germann MD, PhD (Feldkirch), F. Gruber MD (Linz AKH), H-D. Gulle MD (Klagenfurt), T. Haidacher MD (Graz UKH), G. Herzer MD (Wr. Neustadt), P. Hohenauer MD (Salzburg LKA), A. Hüblauer MD (Horn), J. Lanner MD (Salzburg UKH), V. Lorenz MD (Wien UKH XII), C. Mirth MD (St. Pölten), W. Mitterndorfer MD (Linz AKH), W. Moser MD (Klagenfurt), H. Schmied MD (Amstetten), K-H Stadlbauer MD, PhD (Innsbruck), H. Steltzer MD, PhD (Wien UKH XII), Ernst Trampitsch MD (Klagenfurt), A. Waltensdorfer MD (Graz Uni), A. Zechner MD (Klagenfurt). We are also grateful to researchers from INRO: Ingrid Wilbacher PhD collected data during the first project; Ivan Janciak PhD developed and managed the databases used for both projects.
Funding
The data used for this study was collected for a project funded by the Austrian Worker’s Compensation Board (AUVA; FK 33/2003) and by the “Jubilee Fund” of the Austrian National Bank (Project No. 8987), and for a project funded by the Ministry of Health (Contract Oct. 15, 2008) and the AUVA (FK 11/2008, FK 11/2010, FK 09/12). INRO is supported by an annual grant from Mrs. Ala Auersperg-Isham and Mr. Ralph Isham, and by small donations from various sources.
Conflicts of interest
The authors do not have any conflicts of interest. This study has not been presented anywhere.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mauritz, W., Brazinova, A., Majdan, M. et al. Effects of time of hospital admission on outcomes after severe traumatic brain injury in Austria. Wien Klin Wochenschr 126, 278–285 (2014). https://doi.org/10.1007/s00508-014-0521-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-014-0521-9