
Summary
Objective
To evaluate quality of life in women suffering with osteoporosis with or without vertebral fractures for the first time with the German version of the osteoporosis quality of life questionnaire (OQLQ) and to correlate the German OQLQ with the medical outcome survey short-form health survey 36 (MOS SF-36).
Methods
In a cross-sectional study, the OQLQ and the MOS SF-36 were randomly administered to 100 postmenopausal osteoporotic women with a median age of 73.5 (quartiles 65.0; 80.0) years in order to evaluate their quality of life.
Results
Of the total number, 56 women had osteoporosis with at least one vertebral fracture and 44 women had osteoporosis without vertebral fracture. All items of the OQLQ as well as the MOS SF-36 showed significantly worse values for the women with vertebral fracture compared to those without vertebral fracture. Both questionnaires’ domains evaluating physical wellbeing correlated strongly with each other, supporting the concept of convergent construct validity. The OQLQ domain “emotional function” showed higher correlations with different MOS SF-36 subscores than the MOS SF-36 subscore “role emotional” with the different OQLQ domains.
Conclusion
The German version of the OQLQ was demonstrated to be feasible. Significantly, worse results in the German OQLQ for postmenopausal osteoporotic women compared to those without vertebral fracture revealed discriminant validity. The disease-targeted OQLQ seems to better reflect problems associated with low emotional wellbeing because of osteoporotic vertebral fracture.
Zusammenfassung
Ziel
Erstmalig sollte die deutsche Version des Osteoporosis Quality of Life Questionnaire (OQLQ) bei postmenopausalen osteoporotischen Frauen mit und ohne vertebrale Fraktur zum Einsatz kommen und mit dem Medical Outcome Survey short-form healthsurvey 36 (MOS SF-36) verglichen werden.
Methodik
Im Rahmen einer Querschnittsuntersuchung wurden die beiden Fragebögen in randomisierter Weise von 100 osteoporotischen Frauen im Alter von 73.5 (65.0; 80.0) Jahren ausgefüllt.
Ergebnisse
Sechsundfünfzig Frauen litten an einer Osteoporose mit mindestens einer und 44 Frauen an einer Osteoporose ohne Wirbelkörperfraktur. Frauen mit vertebralen Frakturen hatten bei allen Domänen des OQLQ und des MOS SF-36 signifikant schlechtere Ergebnisse als jene ohne vertebrale Frakturen. Zwischen den beiden Fragebögen zeigte sich eine hohe Korrelation in den Domänen, welche die körperliche Funktion untersuchten. Die OQLQ Domäne „emotionale Funktion“ zeigte höhere Korrelationen mit unterschiedlichen MOS SF-36 Subskalen als die MOS SF-36 Subskala „Rollenfunktion in emotionaler Hinsicht“ mit unterschiedlichen OQLQ Domänen.
Schlussfolgerung
Die deutsche Version des OQLQ war einfach in der Anwendung. Postmenopausale osteoporotische Frauen mit Wirbelkörperfraktur waren in ihrer Lebensqualität deutlich mehr eingeschränkt als jene ohne vertebrale Frakturen. Probleme aufgrund von Einschränkungen im emotionalen Wohlbefinden scheinen mit dem krankheitsspezifischen OQLQ besser zu erfassen zu sein als mit dem MOS SF-36.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Life expectancy of the general population is increasing and, thus, the prevalence of osteoporosis—the most prevalent metabolic bone disease in elderly people—is high. More than 200 million people are affected worldwide [1]. Osteoporosis is defined as a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fracture [2]. Fragility fractures cause an increased mortality and pain as well as a decrease in physical and probably also in social function. Fears and apprehensions are contributing to decreased quality of life (QoL), too.
With an estimated prevalence of approximately 25 % in both men and women, vertebral fractures represent the most common of all osteoporotic fractures [3, 4]. Compared with hip fractures, vertebral fractures are less disabling. However, they may also have a negative impact on the patient’s physical function and Qol. One year after vertebral fracture, irrespective of fracture level, fracture type, or grade of fracture deformation, four-fifth of the patients still had pronounced pain and deteriorated QoL [5].
There is a poor correlation between QoL and findings on radiography or densitometry; to evaluate the effects of osteoporosis on patient’s functional status, direct questioning is required [6]. As in other chronic conditions, assessing health-related QoL and using this as an outcome measure is becoming increasingly important in health services research and in clinical trials evaluating osteoporosis-specific medication, exercise, and any other special treatment. Two different types of instruments—generic and disease-targeted—can be used. The MOS SF-36 (Medical Outcome Study—short form)[7] is such a generic measure designed to be applicable across a wide range of medical conditions. It fulfills stringent criteria of reliability [8].
There exist several different disease-targeted instruments which are designed to be sensitive to the outcomes of the particular disease processes. The Osteoporosis Quality of Life Questionnaire (OQLQ) [6] is one of them designed for use in women with vertebral fractures; its reliability varied from 0.80 to 0.89 for the five domains [9]. Originally this questionnaire was published in English. According to a standardized protocol [10] this disease-specific questionnaire was translated into the German language and we applied it to a small group of female Austrian osteoporotic patients [11]. The aim of the present study was to validate the German version of the OQOL questionnaire in female osteoporotic patients with and without vertebral fractures.
Materials and methods
Subjects
Ambulatory, community-dwelling female patients with the diagnosis of osteoporosis according to the WHO criteria visiting one of three outpatient clinics for osteoporosis of Vienna (the Department of Physical Medicine & Rehabilitation, Medical University of Vienna, or the Departments of Internal Medicine of the Vincent Hospital of Vienna, or the Department of Medicine, Hospital Barmherzige Brüder Wien) were asked to participate in the study. Included were pre and postmenopausal women suffering from primary or secondary osteoporosis. Bone mineral density (BMD) measurements of the lumbar spine and the femoral neck were required to be performed within the preceding year and an X-ray of the thoracal and lumbar spine within the previous 2 years. However, in case of an acute back pain episode within these previous 2 years, a recent X-ray of the spine was made. Patients suffering of nonosteoporotic osteopathies like osteomalacia or Paget’s disease as well as patients suffering from any other disease which may cause back pain like rheumatoid arthritis or vertebral disc herniation were not eligible for the study. Major neurologic, pulmonary, cardiac, or psychiatric illness, which could substantially influence the patient’s QoL, was also excluded. Of course, patients had no linguistic barriers or cognitive impairments.
The study was approved by the Ethics Committee of the Medical University of Vienna.
Bone mineral density measurement
BMD of the lumbar spine and the femoral neck were measured either with dual-energy X-ray absorptiometry (DXA) using QDR 4500 (Hologic, Inc., Waltham, MA, USA) or LUNAR DPX (Lunar Corp., Madison, WI, USA). BMD data are given as T score.
Data collection
Besides sociodemographics, lifestyle factors including habits concerning smoking, alcohol intake, and physical activities as well as medical history (family history, previous fractures, intake of medications) were assessed. On basis of the history and the biochemical analysis patients were classified as suffering from primary or secondary osteoporosis. Standing height was measured in stocking feet to the nearest centimeter using a stadiometer, and weight was measured using a balance beam scale, recalibrated monthly.
For assessing general QoL, the patients filled in the German version of the MOS SF-36 [12]. The questionnaire consists of 36 items related to eight scales that cover different health aspects: “physical functioning” (PFI), “role physical” (ROLPH), “role emotional” (ROLEM), “social functioning” (SOCIAL), “mental health” (MHI), “bodily pain” (PAIN), “vitality” (VITAL), and “general health perception” (GHP). The disease-specific OQLQ which is composed of 30 questions with four sets of seven response options on differently colored cards covering five domains: symptoms (nine items), physical function (five items), activities of daily living (eight items), emotional function (four items), and leisure (four items) was collected on an interviewer-administered basis. The order in which the questionnaires were to be administered to patients had previously been randomized in order to avoid a potential bias by always filling one of the two questionnaires out first.
Statistics
For MOS SF-36 a score of zero represents worst possible health and a score of 100, best possible health. For OQLQ, each item is associated with a seven-point scale in which a rating of 7 represents the best possible function and a rating of 1 the worst possible function. To produce a summary score for each of the five domains, the patient’s ratings on each item are added up and then divided by the number of items in the domain.
The results of these questionnaires as well as of other continuous variables are presented as median (quartiles) and compared between two groups using Wilcoxon’s rank-sum test due to their asymmetric distributions. No adjustment for multiple testing is done due to the exploratory character of the study. Pairwise associations between domain subscores of the two questionnaires are quantified using Spearman’s correlation coefficients. Correlations greater than 0.5 and 0.7 are classified as moderate and strong, respectively.
The reported p-values are the results of two-sided tests. p-values ≤ 0.05 were considered to be statistically significant. All computations have been performed using SAS software Version 9.2 (SAS Institute Inc., Cary, NC, USA, 2008).
Results
One hundred females with a median age of 73.5 [quartiles 65.0; 80.0] years participated in the study. Fifty-six women had osteoporosis with vertebral fracture and 44 women had osteoporosis without vertebral fractures. Nobody had sustained a recent vertebral fracture within the last 6 months. Characteristics of the whole study population as well as for the two subgroups are given in Table 1. There were hardly any smokers; eight women of the whole study population. Nobody reported an alcohol problem. Most patients had primary osteoporosis and the percentage of women with a positive family history was similar in both groups, 32 and 34 %. More patients of those with vertebral fractures compared to those without vertebral fractures had peripheral fragility fractures, 44 (79 %) versus 18 (41 %). The percentage of patients with a regular intake of osteoporosis-specific medication and—if necessary—supplementation with calcium and vitamin D was higher in the group with vertebral fracture. However, patients without vertebral fractures were more active with more women regularly performing gymnastics. The median lumbar spine T-Score was − 2.5 [− 3.1; − 2.1] for the women with vertebral fracture and − 3.0 [− 3.4; − 2.5] for the women without vertebral fracture. Respective values for the femoral neck were − 2.8 [− 3.1; − 2.1] and − 2.3 [− 3.1; − 1.8].
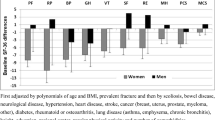
Assessment of both QoL questionnaires was easy to perform; patients did not have any problems answering the questions of the OQLQ. Scores are given in Table 2. All items of the generic MOS SF-36 as well as all items of the disease-specific OQLQ showed significantly worse values for women with vertebral fracture compared to those without vertebral fracture. There were no significant differences in QoL between patients with primary and secondary osteoporosis (data not shown).
Table 3 shows the correlation coefficients between the domains of the two QoL scores. As expected, there was a strong correlation between the domains symptoms as well as activities of daily living of the QOLQ and following MOS SF-36 subscores: physical functioning, role limitations because of physical health problems, bodily pain, and vitality; a moderate correlation existed with general health perception. Except for an only moderate correlation coefficient with the vitality subscore, the correlations of the OQLQ domains physical function and leisure with the accordant MOS SF-36 subscores were similar. However, their correlation coefficients with the vitality subscore were only moderate. The OQLQ domain emotional function showed week to moderate correlations with role physical, mental health, bodily pain, vitality, and general health perception of the MOS SF-36.
Discussion
Osteoporosis is thought to be a silent disease. However, fractures—the clinical outcome of osteoporosis—lead to pain, and probably to restrictions in physical and emotional function as well. The assessment of QoL is needed to properly quantify the disease burden. Several disease-specific questionnaires exist to evaluate possible restrictions in QoL because of osteoporosis. Most of them exist in many different languages. The OQLQ was translated into the German language, but this is the first study evaluating the German version of the OQLQ questionnaire in female osteoporotic patients and correlating it with the general questionnaire MOS SF-36. Handling with this German version of the OQLQ was easy and for the first time it was shown with the German OQLQ that quality of life of women with vertebral fracture was more impaired than that of osteoporotic women without vertebral fracture. This agrees well with previous data evaluating QoL in such patients and showing an inverse association between the number of prevalent vertebral fractures and health-related QoL with the OQLQ [13], the Mini-OQLQ [14, 15], or other QoL questionnaires [16–18].
Regarding the MOS SF-36 questionnaire, we also observed that QoL was compromised in all the domains evaluated in women with vertebral fracture compared to those without vertebral fracture. That finding has already been shown previously [15] and is in line with a Japanese study which found that osteoporotic patients with chronic back pain had a poorer QoL status evaluated with the MOS SF-36 than the standard Japanese population [19].
Correlations between this German version of the OQLQ and the MOS SF-36 were similar to those given in the literature in different languages [9, 19]. The only study correlating all domains of the two questionnaires with each other so far was the investigation performed by Badia and coauthors [20]. Throughout all domains our correlation coefficients were higher than theirs. Differences in the Spanish compared to our German version of the OQLQ as well as differences in patients’ age may explain our higher correlation coefficients. Notably, it was more difficult to assess emotional wellbeing than physical function with these questionnaires. Looking at the MOS SF-36 subscores “role emotional,” “social functioning,” and “mental health” only the last one showed a moderate/week correlation with the OQLQ domain “emotional function”; otherwise there were no correlations with any of the OQLQ domains. On the other hand, the OQLQ domain “emotional function” showed week to moderate correlations with some MOS SF-36 subscores including role physical, mental health, pain, vitality, and general health perception. Thus, the disease-targeted OQLQ seems to better comprise problems associated with reductions in emotional wellbeing due to osteoporotic vertebral fracture. Physical limitations seem to be easier to quantify. Accordant correlations were generally strong.
Since fragility fractures occur in the older age groups and a substantial proportion of these subjects have many clinically relevant comorbidities fractures are likely to be only one of the many medical conditions that influence health-related QoL. Thus, a general QoL questionnaire is suitable to evaluate possible general problems. On the other hand, disease-targeted measures focus on characteristics of particular relevance to the disease which may not be well represented by a generic instrument. Disease-specific and generic health-related QoL instruments are not redundant when applied together; they measure different aspects of health-related QoL. In direct comparisons in varying areas other than osteoporosis, specific instruments have proved more responsive to intervention effects than generic measures [9]. Therefore, it is good to assess both, a generic and a disease-specific questionnaire.
One might ask why many, many years even more than 10 years after vertebral fracture, more patients have back pain and subjectively impaired health status than controls [21]. The change in the shape of the vertebral body due to fracture alters the position of that spinal segment, which affects the alignment of the entire trunk. An increased thoracic kyphosis for instance means an elongation of the back muscles which, in turn, leads to less effective muscle function and excessive strain. Over time the altered spinal configuration may lead to chronic pain, reduction of spinal mobility, and reduced QoL. Of course, this change in posture also means a change in the somatosensory system with an increased susceptibility to falling. Fear of falling and, thus, induced restrictions in activities of daily living, in addition, reduce that person’s QoL.
There are several different disease-specific QoL questionnaires. We decided to use the OQLQ because it proved to be as powerful or even more powerful than alternative instruments for detecting improvement or deterioration in women with osteoporosis and back pain caused by vertebral fractures related to osteoporosis [9] and the OQLQ showed better discriminant power than the QUALEFFO [20]. In addition, we had translated that questionnaire into the German language and, thus, already had some experience using this tool in a small sample size.
BMD measurement was performed to evaluate if patients were osteoporotic according to the WHO criteria. The higher BMD values of the lumbar spine in women with vertebral fracture compared to women without vertebral fracture may be explained by false high BMD values which could result from morphologic changes in the vertebra after fracture. BMD of the femoral hip was lower in patients with vertebral fracture which may show that they were more severely affected than patients without vertebral fracture.
Strength of this study is that we did not have missing values for any item of the OQLQ and that these data are reliable because the OQLQ was assessed on an interviewer-administered basis. The MOS SF-36 is suitable for use with older adults, however, since it had been shown that some assistance may often be required in people aged 75 years and over [22], we assisted the women in case of any ambiguity. Of course, this is an advantage and a disadvantage at the same time because it takes about 10–15 min to fill in the questionnaires and in daily routine every minute counts. Another limitation of the study is that we did not further divide the group of patients with vertebral fracture according to the number or the location of the fracture(s). Sample size was too small to further split the group but we have already known for a long time that the higher the number of vertebral fractures the higher the percentage of postmenopausal women suffering of back pain and limited activity due to back pain [23]. Concerning the impact of the location of vertebral fracture on QoL data are diverse. According to Lips and Van Schoor [24] lumbar fractures have more impact on QoL than thoracic fractures. However, according to another study the location of the vertebral fracture does not make any difference [25].
Conclusions
Health-related QoL refers to how well an individual functions in daily life and her/his subjective perception of wellbeing. Vertebral deformities increase the kyphosis angle and, thus, cause a change in posture and overstraining of the back muscles as well as the vertebral joints. Long-term impairment and restriction in QoL are possible consequences. Postmenopausal osteoporotic women with vertebral fractures are worse off in all domains of the generic MOS SF-36 as well as in the disease-specific OQLQ which was evaluated for the first time in the German language. The German OQLQ correlated well with the MOS SF-36, especially the physical domains. Problems associated with loss in emotional wellbeing because of osteoporotic vertebral fracture seem to be better reflected by the disease-specific questionnaire. Thus, the German OQLQ seems to be suitable to evaluate impairments in QoL in osteoporotic women with vertebral fracture(s).
Acknowledgments
We want to thank Dr Krenbek, Dr Stupphan, Dr Thun, Dr Lung for filling in the questionnaires with the patients. This study was supported by a research grant from the Österreichische Gesellschaftfür Rheumatologie.
References
Reginster YN, Burlet N. Osteoporosis: a still increasing prevalence. Bone 2006;38:S4–S9.
Kanis JA, Burlet N, Cooper C, et al. European guidance for the diagnosis in postmenopausal women. Osteoporos Int. 2008;19:399–428.
O’Neill TW, Felsenberg D, Varlow J, Cooper C, Kanis JA, Silman AJ. The prevalence of vertebral deformity in European men and women: the European Vertebral Osteoporosis Study. JBMR. 1996;11:1010–8.
Jackson SA, Tenenhouse A, Robertson L. Vertebral fracture definition from population-based data: preliminary results from the Canadian multicenter osteoporosis study (CaMos). Osteoporos Int. 2000;11:680–7.
Suzuki N, Ogikubo O, Hansson T. The prognosis for pain, disability, activities of daily living and quality of life after an acute osteoporotic vertebral body fracture: its relation to fracture level, type of fracture and grade of fracture deformation. Eur Spine J. 2009;18:77–88.
Cook DJ, Guyatt GH, Adachi JD, et al. Quality of life issues in women with vertebral fractures due to osteoporosis. Arthritis Rheum. 1993;36:750–6.
Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF 36), I: conceptual framework and item selection. Med Care. 1999;30:150–60.
Brazier JE, Harper R, Jones NMB, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305:160–4.
The Osteoporosis Quality of Life Study Group. Measuring quality of life in women with osteoporosis. Osteoporos Int. 1997;7:478–87.
Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Epidemiol. 1993;46:1427–32.
Kerschan-Schindl K, Uher E, Preisinger E, Pietschmann. Anwendung des in die deutsche Sprache übersetzten Osteoporosis Quality of Life Questionnaire (OQLQ). Wien Klin Wochenschr. 1999;111:608–11.
Bullinger M, Kirchberger I, Ware J. Der deutsche SF-36 health survey. Z f Gesundheitswissenschaften. 1995;3:21–36.
Sambrook PN, Silverman SL, Cauley JA, et al. Helath-related quality of life and treatment of postmenopausal osteoporosis: results from the HORIZON-PFT. Bone 2011;48:1298–1304.
Adachi JD, Joannidis G, Olszynski WP, et al. The impact of incident vertebral and non-vertebral fractures on health related quality of life in postmenopausal women. BMC Musculoskelet Disord. 2002;3:11–6.
Salaffi F, Cimmino MA, Malavolta N, et al. The burden of prevalent fractures on health-related quality of life in postmenopausal women with osteoporosis: the IMOF study. J Rheumatol. 2007;34:1551–60.
Lips P, Cooper D, Agnusdei D, et al. Quality of life in patients with vertebral fractures: Validation of the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO). Osteoporos Int. 1999;10:150–60.
Cockerill W, Lunt M, Silman AJ, et al. Health-related quality of life and radiographic vertebral fracture. Osteoporos Int. 2004;15:113–9.
Jahelka B, Dorner T, Terkula R, Quittan M, Bröll H, Erlacher L. Health-related quality of life in patients with osteopenia or osteoporosis with and without fractures in a geriatric rehabilitation department. WMW. 2009;159:235–40.
Yoh K, Tanaka K, Ishikawa A et al., Health-related quality of life (HRQOL) in Japanese osteoporotic patients and its improvement by elcatonin treatment. J Bone Miner Metab. 2005;23:167–73.
Badia X, Diez-Perez A, Alvarez-Sanz C, et al. Measuring quality of life in women with vertebral fractures due to osteoporosis: a comparison of the OQLQ and QUALEFFO. Qual Life Res. 2001;10:307–17.
Hasserius R, Karlsson MK, Jonsson B, Redlund-Johnell I, Johnell O. Long-term morbidity and mortality after a clinically diagnosed vertebral fracture in the elderly—a 12- and 22-year follow-up of 257 patients. Calcif Tissue Int. 2005;76:235–42.
Hayes V, Morris J, Wolfe C, Morgan M. The SF-36 health survey questionnaire: Is it suitable for use with older adults? Age Ageing. 1995;24:120–5.
Nevitt MC, Ettinger B, Black DM, et al. The association of radiographically detected vertebral fractures with back pain and function: a prospective study. Ann Intern Med. 1998;128:793–800.
Lips P, van Schoor NM. Quality of life in patients with osteoporosis. Rev Osteoporos Int. 2005;16:447–55.
Fechtenbaum J, Cropet C, Kolta S, Horlait S, Orcel P, Roux C. The severity of vertebral fractures and health-related quality of life in osteoporotic postmenopausal women. Osteoporos Int. 2005;16:2175–9.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kerschan-Schindl, K., Patsch, J., Kudlacek, S. et al. Measuring quality of life with the German Osteoporosis Quality of Life Questionnaire in women with osteoporosis. Wien Klin Wochenschr 124, 532–537 (2012). https://doi.org/10.1007/s00508-012-0212-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-012-0212-3