
Abstract
Moor mud applications in the form of packs and baths are widely used therapeutically as part of balneotherapy. They are commonly given as therapy for musculoskeletal disorders, with their thermo-physical effects being furthest studied. Moor baths are one of the key therapeutic elements in our recently developed and evaluated 3-week prevention program for subjects with high stress level and increased risk of developing a burnout syndrome. An embedded pilot study add-on to this core project was carried out to assess the relaxing effect of a single moor bath. During the prevention program, 78 participants received a total of seven moor applications, each consisting of a moor bath (42 °C, 20 min, given between 02:30 and 05:20 p.m.) followed by resting period (20 min). Before and after the first moor application in week 1, and the penultimate moor application in week 3, salivary cortisol was collected, blood pressure and heart rate were measured, and mood state (Multidimensional Mood State Questionnaire) was assessed. A Friedman test of differences among repeated measures was conducted. Post hoc analyses were performed using the Wilcoxon signed-rank test. A significant decrease in salivary cortisol concentration was seen between pre- and post-moor bath in week 1 (Z = −3.355, p = 0.0008). A non-significant decrease was seen between pre- and post-moor bath in week 3. Mood state improved significantly after both moor baths. This pilot study has provided initial evidence on the stress-relieving effects of single moor baths, which can be a sensible and recommendable therapeutic element of multimodal stress-reducing prevention programs. The full potential of moor baths still needs to be validated. A randomized controlled trial should be conducted comparing this balneo-therapeutic approach against other types of stress reduction interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The medical application of peloids (e.g., peat, fango, medicinal mud) is one of the key components of health resort medicine. Moor baths are prepared using moor mud (peat pulp) consisting of organic matter, minerals, and water. They have been widely used therapeutically as part of balneotherapy in European health resorts for more than 200 years (Beer et al. 2013; Gutenbrunner et al. 2010). Moor mud applications in the form of packs and baths (head out immersion) can be used to help with a variety of complaints, mainly in musculoskeletal disorders. Arthroses, osteoporosis, rheumatic diseases (e.g., ankylosing spondylitis, rheumatoid arthritis in subacute and chronic stage, fibromyalgia), gynecological disorders (e.g., chronic inflammation, infertility, ovarian failure), and psoriasis are the most common indications for treatment with moor baths (Beer et al. 2013; Kraft 2012; Stier-Jarmer et al. 2015).
Moor baths are associated with thermo-physical, astringent, resorptive, and chemical effects of which the most studied are the thermo-physical effects. The pulpy consistency, the high level of heat preservation, and the evenly slow heat release enable careful heat transfer by conduction. The supplied heat penetrates into deeper tissue structures and results in an increase in core body temperature by about 2 °C during a 20-min moor bath. With this passive mild whole body hyperthermia, pain relief, relaxation of muscles and subcutaneous connective tissues, and anti-inflammatory effects can be achieved (Beer et al. 2013).
Furthermore, taking a warm moor bath is usually found to be beneficial and relaxing (Kraft 2012). The relaxing and stress-relieving effect, however, is part of physicians’ and patients’ knowledge gained from experience but has not been scientifically examined to date.
In recent years, a number of studies have been conducted aiming at examining the stress-relieving effect of single therapeutic interventions, including in the field of balneotherapy, using salivary cortisol concentration as an objective stress marker, often coupled with self-report data (Matousek et al. 2010).
Pawlow and Jones, for example, found that a brief relaxation exercise (20 min) caused significantly lower levels of post-intervention heart rate, state anxiety, perceived stress, and salivary cortisol concentration, as well as increased self-reported levels of relaxation, than a control intervention (20 min of quietly sitting) (Pawlow and Jones 2005). Kanitz et al. aimed at evaluating the effects of a single rhythmical massage intervention compared to a sham massage on well-being, mood, and salivary cortisol concentration. No statistically significant effects were observed within this trial (Kanitz et al. 2015). A Japanese study examined the stress-relieving effect of bathing in warm thermal mineral water (sodium-chloride; 42 °C; 60 min) in a high- and a low-stress group of healthy male students using a pre-post-design. Salivary cortisol levels and subjective perception of stress significantly decreased during spa bathing with a stronger decline in the high-stress group (Toda et al. 2006). Austrian researchers were able to show that bathing in warm thermal mineral water (sodium, chloride, and hydrogen carbonate; 36 °C; 25 min) had a stress-relieving effect in healthy volunteers. Participants were randomized to bathing, progressive muscle relaxation (PMR), or resting. Salivary cortisol levels decreased during interventions in all three groups. Self-reported levels of relaxation were higher in participants in the bathing group compared to the control groups (Matzer et al. 2014).
To our knowledge, similar studies to evaluate the stress-relieving effects of moor baths have not yet been performed. Moor baths are one of the key therapeutic elements in our recently developed and evaluated secondary prevention program for subjects with high stress level and increased risk of developing burnout syndrome. We assumed that, despite the pain-reducing and muscle relaxing potential, moor baths also have stress-relieving and relaxing effects (Stier-Jarmer et al. 2016). This paper will present findings from an embedded pilot study add-on to the core project, designed to test the hypothesis that a single moor bath has a relaxing effect which is reflected both in the physiological stress/relaxation response and in the psychological state.
Materials and methods
This pilot study was embedded in a randomized controlled study with waiting control group design, evaluating a multimodal program for stress reduction and burnout prevention by combining traditional health resort treatment with stress management interventions. The 3-week prevention program included four key therapeutic elements: (1) a stress management seminar on burnout prevention, (2) relaxation (Hatha-Yoga, Qigong, mindfulness training, progressive muscle relaxation), (3) physical exercise (“back school,” endurance sports activities), and (4) local natural remedies (moor baths followed by resting period and massage). Participants were adults with an above-average level of perceived stress (PSQ total ≥50, which corresponds to the mean plus one standard deviation in healthy adults (Fliege et al. 2005)) and an increased risk for developing a burnout syndrome (Emotional Exhaustion Scale (MBI-EE) of the Maslach Burnout Inventory–General Survey (MBI-GS-D) (Büssing and Glaser 1998; Schaufeli et al. 1996) between 3.6 and 5.2). The program was carried out in Bad Aibling, the oldest moor spa in Bavaria, Germany. Details of study methodology, intervention, and results are given elsewhere (Stier-Jarmer et al. 2016). The study had institutional ethics committee approval (Ethics Committee of the Faculty of Medicine, Ludwig-Maximilians-University München) and included written informed consent.
Procedure
During the 3-week prevention program, participants received a total of seven moor applications, each consisting of a moor bath (42 °C, 20 min) followed by resting period (20 min). All baths were given in the afternoon between 02:30 and 05:20 p.m. The measurements for the embedded pilot study were taken before and after the first moor application in week 1 of the prevention program (T1 and T2) and before and after the penultimate moor application in week 3 (T3 and T4).
The moor applications were given by experienced professionals (state-examined masseurs/balneotherapists) in two local rehabilitation clinics and one spa treatment center.
Measures
Salivary cortisol was collected, blood pressure and heart rate were measured, and participants were asked to assess their mood state at all time points (T1–T4). All procedures were carried out by the clinical staff who had been instructed by study personnel prior to the beginning of the study. Baseline demographic and clinical characteristics of participants were collected at the beginning of the 3-week prevention program 1 to 4 days prior to the first moor bath.
Salivary cortisol
In order to prevent falsification of results, participants were instructed not to eat, drink, or smoke for an hour prior to collection and not to brush teeth prior to sampling. In addition, they should not drink alcohol until delivery of the final saliva sample on the days of sampling.
Salivary cortisol was measured in the standard unit of pg/ml (reference range for measurements in the morning: 2300–12,700 pg/ml and in the afternoon: 500–4200 pg/ml) and analyzed using the salivary test cortisol of medivere:diagnostics/GANZIMMUN DIAGNOSTICS AG, Mainz, Germany. Prior to the first saliva collection at each measurement, the participants had to rinse their mouth with water. Saliva was gathered in the mouth, and then was spat in plastic tubes using a drinking straw. The plastic tubes had to be at least half full of saliva. The samples were collected by study personnel and sent to the laboratory within 24 h after the final sampling.
Mood state
Mood state was measured using the German version of the Multidimensional Mood State Questionnaire (MDBF) (Hinz et al. 2012; Steyer et al. 1997). The long format of the questionnaire comprises 24 items which ask for the current mood (“At the moment, I feel …”). The items consist of simple adjectives such as “tired,” “happy,” and “nervous.” Each item is rated on a five-point scale ranging from 1 (not at all) to 5 (very). Three subscales can be calculated (good-bad mood [GB], alertness–tiredness [AT], and calmness–restlessness [CR]). The possible values for each scale range from 8 to 40, with higher values meaning better mood, greater alertness, and greater calmness.
Blood pressure (systolic/diastolic) and heart rate
Blood pressure and heart rate were measured before and after the two moor baths. Participants rested in a seated position for 5 min. Blood pressure was measured on the left upper arm. Heart rate was measured manually at the radial artery for 15 s and multiplied by 4.
Participant satisfaction
The satisfaction with the burnout prevention program including seven moor baths (Stier-Jarmer et al. 2016) was evaluated post-intervention using a self-developed questionnaire containing, for example, questions on the program in general, therapeutic components, and competence/performance of the staff. The questionnaire ends with open questions asking participants, among other topics, about the program components with which they were most satisfied.
Data analysis
Single missing items in the questionnaires were replaced, where appropriate, by the mean of the available values in the respective dimension.
Data analysis was performed for all participants who received both moor baths (weeks 1 and 3) and of which four cortisol samples were available.
All parameters were tested for normal distribution using the Kolmogorov-Smirnov test. For most parameters, a normal distribution was rejected; therefore, non-parametric methods were used for the analysis of change.
A non-parametric Friedman test of differences among repeated measures was conducted. In case of a significant Friedman test, post hoc analyses were performed using the Wilcoxon signed-rank test and a Bonferroni correction with p < 0.017 (0.05/3 comparisons).
Effect size r was calculated as the quotient of the test statistics Z divided by the square root of the number of cases.
SPSS Statistics 23.0 software was used for all analyses.
Results
Of the 90 initially enrolled study participants (Stier-Jarmer et al. 2016), a total of 80 participants eventually completed the burnout prevention program. Two of these participants had to be excluded from the data analysis of the moor study. The first did not receive the two moor baths due to migraine; in the second participant, the saliva samples at T1/T2 were insufficient.
Demographics and clinical variables of the remaining participants (N = 78) are presented in Table 1.
Changes in target parameters after moor baths
For most participants (61.5% in week 1, 46.2% in week 3), a meaningful reduction in cortisol concentration after the moor baths could be seen. Other participants (12.8% in week 1, 19.2% in week 3) remained largely unchanged. In nine persons (11 measurements), cortisol values exceeding the upper limit of the reference range occurred after the moor bath. Whereas two of these individuals achieved cortisol values above the upper reference value after both baths, the seven other participants had values within the normal range for the other cortisol measurements. In four male participants, at least one salivary cortisol value post-moor bath was extremely high exceeding twice the upper reference value.
The Friedman test found significant differences between the four time points (pre/post-moor bath in week 1, pre/post-moor bath in week 3) in salivary cortisol, systolic and diastolic blood pressure, heart rate, and in the three MDBF subscales MDBF-GB, MDBF-AT, and MDBF-CR (Table 2).
Post hoc analysis with Wilcoxon signed-rank test was conducted with a Bonferroni correction applied, resulting in a significance level set at p < 0.017. The median salivary cortisol concentration was 2434.5 pg/ml at T1, 1961.5 pg/ml at T2, 1588.5 pg/ml at T3, and 1357.5 pg/ml at T4 (Table 2 and Fig. 1). A significant decrease was seen between pre- and post-moor bath in week 1 (Z = −3.355, p = 0.0008) and between post-moor bath in week 1 and pre-moor bath in week 3 (Z = −2.622, p = 0.0087). A non-significant decrease was seen between pre- and post-moor bath in week 3 (Z = −1.399, p = 0.1617).

Salivary cortisol concentration before and after moor baths in week 1 and week 3 (N = 73; outliers exceeding twice the upper reference value (>8400 pg/ml) were trimmed). Wilcoxon test p (T2-T1) = 0.001, p (T4-T3) = 0.162. The bottom and top of each box are the first and third quartiles (25 and 75% percentiles). The band inside the box is the median. The lines extending vertically from the boxes (whiskers) characterize the largest and smallest value, which is not classified as an outlier or an extreme value. The distance of outliers from the 25 or the 75% percentile is between 1.5 times and 3 times the box height. Outliers are represented by circles. The distance of extreme values from the 25 or the 75% percentile is more than three times the box height. Extreme values are represented by asterisks
Effect sizes r ranged from small (−0.16) to medium (−0.38).
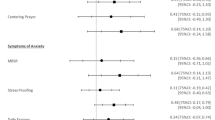
Blood pressure levels (systolic and diastolic) were significantly lower after the moor baths. Heart rate increased during the moor baths but the changes were not statistically significant. The heart rate in week 3, however, was significantly lower than in week 1. The post hoc analysis on mood state showed significant changes in all three subscales after both moor baths (MDBF-GB good mood increased, MDBF-AT tiredness increased, and MDBF-CR calmness increased) (Fig. 2).

Good/bad mood, alertness/tiredness, and calmness/restlessness before and after moor baths in week 1 and week 3 (N = 78). Wilcoxon test (good/bad mood) p (T2-T1) < 0.001, p (T4-T3) < 0.001. Wilcoxon test (alertness/tiredness) p (T2-T1) = 0.017, p (T4-T3) < 0.001. Wilcoxon test (calmness/restlessness) p (T2-T1) < 0.001, p (T4-T3) < 0.001. The bottom and top of each box are the first and third quartiles (25 and 75% percentiles). The band inside the box is the median. The lines extending vertically from the boxes (whiskers) characterize the largest and smallest value, which is not classified as an outlier or an extreme value. The distance of outliers from the 25 or the 75% percentile is between 1.5 times and 3 times the box height. Outliers are represented by circles. The distance of extreme values from the 25 or the 75% percentile is more than three times the box height. Extreme values are represented by asterisks
Participant satisfaction
In general, participant assessments of the overall program were clearly positive. Among the therapeutic elements, especially the moor applications received top ratings (90% “very good”). Fifty-five percent of participants said that they were particularly satisfied with the moor applications.
Discussion
We conducted an uncontrolled exploratory pilot study to examine the effects of two single therapeutic moor baths on physiological stress response and psychological state. This study was an embedded add-on to the core project, a randomized controlled study with waiting control group design evaluating a multimodal program for stress reduction and burnout prevention.
The two single moor baths followed by resting periods (20 min each) have shown to improve mood and to decrease salivary cortisol concentration and blood pressure in adults with an above-average level of perceived stress and an increased risk for developing a burnout syndrome.
Salivary cortisol concentration decreased significantly during the first moor bath in week 1, between post-moor bath in week 1 and pre-moor bath in week 3, and between pre-moor bath in week 1 and pre-moor bath in week 3. A non-significant decrease was seen between pre- and post-moor bath in week 3. Vasodilation induced by moor baths significantly decreased blood pressure and slightly increased heart rate. Significant improvement in mood and calmness after both moor baths could be observed.
The results of cortisol concentrations, illustrated in Fig. 1, reveal that the salivary cortisol levels seen in this pilot study reflect not only the effects of the single moor baths but also the effects of the entire 3-week prevention program, which has shown to be highly effective in reducing perceived stress and burnout symptoms as measured by self-report questionnaires (Stier-Jarmer et al. 2016). Salivary cortisol concentration prior to the moor bath in week 3 was significantly lower than cortisol concentrations before and after the first moor bath in week 1, indicating a substantial reduction in stress level due to participation in the multimodal prevention program for more than 2 weeks.
The same applies to mood state (Fig. 2). Prior to the first moor bath, mean scores of the three MDBF subscales in this study were considerably lower (between 2.3 and 4.8 points) compared to a reference group in the same age range and representative of the German population (Hinz et al. 2012), indicating the initially poor mental well-being of our study population. After the first moor bath, and even more markedly after the moor bath in week 3, the scores had improved and were between 3.1 and 5.2 points above the German reference values.
An exception to this is the alertness scale MDBF-AT which decreased after moor baths. Decreasing values indicate more tiredness and less alertness, which would usually be considered as negative mood (Steyer et al. 1997). However, this is a special case; warm moor baths provide beneficial relaxation, which leads to participants feeling, at least temporarily (see Fig. 2), more tired and sleepy. In this case, the decreasing MDBF-AT scores, therefore, should not be judged negatively, but can be considered as the natural consequence of a relaxing intervention.
Effectiveness of balneotherapy in reducing stress
Balneotherapy may be a stress-relieving measure, as supported also by several recently published studies (Matzer et al. 2014; Rapoliene et al. 2016; Toda et al. 2006). The aforementioned studies by Matzer et al. and Toda et al., for example, showed that bathing in warm thermal mineral water had a significant stress-relieving effect in healthy individuals as measured by physiological (e.g., salivary cortisol levels) and psychological (subjective perception of stress) response. A current randomized controlled questionnaire-based study by researchers from Lithuania found that 108 g/l salinity geothermal water baths administered to seamen for 2 weeks; five times a week; reduced stress, fatigue, and pain; improved mood; and proved to be more efficient for relieving stress and pain than music therapy (Rapoliene et al. 2016).
Study limitations and strengths
As our pilot study did not involve a control group, we do not know how much of the observed effect is due to the moor baths or simply due to 20-min warm bathing or resting while bathing or other potential stress-relieving factors. The lack of a control group was therefore the major limitation of this study.
Salivary cortisol is considered to be a valid and reliable indicator of the hypothalamus-pituitary-adrenal (HPA) stress activity. The advantages compared to serum cortisol are evident: easier to collect, non-invasive procedure which enables a less stressful handling of sampling, not dependent on the availability of a health care professional, lower costs, and the possibility of repeated sampling even in short time intervals (Kirschbaum and Hellhammer 1994; Marques et al. 2010). Samples are stable at room temperature for 1 to 2 days (Turpeinen and Hamalainen 2013).
Possible disadvantages are (a) participants may be stressed by dry mouth that is, in the case of our study, caused by the warm moor bath and leads to concerns of not having enough saliva for sampling. This may have been the case with a few of our participants. To prevent this, participants were encouraged to rinse out mouth with water immediately after moor bath before the 20-min resting period. (b) Falsely elevated cortisol values by contamination with blood (e.g., by bleeding gums, inflammation of the mouth, tongue or cheek bite injuries) sometimes cannot be avoided. However, this is usually checked by the laboratory, and the sample would not be evaluated in this case.
Salivary cortisol concentration follows a strong circadian rhythm (after a peak during the first hour after awakening, continuously decreasing for the rest of the day) with the highest levels in the morning and lowest at midnight (Heaney et al. 2012; Kirschbaum and Hellhammer 1994). Single assessments of cortisol are therefore dependent on the time of day. All samples in our study were taken within a 3-h window in the afternoon between 02:30 and 05:20 p.m. Despite this relatively tight time frame, a small diurnal variation cannot be completely excluded.
It is positive to note that the moor baths were given in a real-world clinical setting by experienced professionals in two local rehabilitation clinics and one spa treatment center, that the treatment was very positively received by the participants, and that both physiological and psychological responses were collected for all participants.
To our knowledge, the present study is the first to examine the stress-relieving effects of moor baths. The findings suggest that moor baths can have a positive, albeit small to moderate, effect on the stress levels of highly stressed adults. Accordingly, moor baths could be an effective therapeutic intervention for stress reduction as an integral part of multimodal burnout prevention programs.
Our study participants were selected based on their level of perceived stress and the extent of burnout symptoms. The group was composed mainly of women with a mean age of 50.5 years and was likely not representative of the general population. It is uncertain whether the results of this pilot study can be generalized to other populations. For our study population, however, we could show the positive effects of moor baths on level of stress and well-being.
Conclusion
This pilot study has provided initial evidence on the stress-relieving effects of two single moor baths, which have been shown to improve mood and to decrease salivary cortisol concentration in adults with an above-average level of perceived stress and an increased risk for developing a burnout syndrome. Moor baths can, therefore, be considered as a sensible and recommendable therapeutic element of multimodal stress-reducing prevention programs. However, this uncontrolled preliminary study was only a first step, which has helped to determine whether the intervention has the potential to make a difference. The full potential of moor baths still needs to be validated. The next step could be to conduct a randomized controlled trial comparing this balneotherapeutic approach against other types of stress reduction interventions of equal duration (e.g., warm immersion baths using tap water or medical mineral waters of different chemical composition, meditation, and resting), investigating the impact on salivary cortisol concentration and further stress-relevant parameters where appropriate.
References
Beer AM, Fetaj S, Lange U (2013) [Peloid therapy. An overview of the empirical status and evidence of mud therapy] Zeitschrift fur. Rheumatologie 72:581–589. doi:10.1007/s00393-013-1144-7
Büssing A, Glaser J (1998) Managerial stress und burnout, a collaborative international study (CISMS), die deutsche Untersuchung vol Bericht nr.44. Technische Universität, Lehrstuhl für Psychologie, München
Fliege H, Rose M, Arck P, Walter OB, Kocalevent R-D, Weber C, Klapp BF (2005) The Perceived Stress Questionnaire (PSQ) reconsidered: validation and reference values from different clinical and healthy adult samples. Psychosom med 67:78–88. doi:10.1097/01.psy.0000151491.80178.78
Gutenbrunner C, Bender T, Cantista P, Karagulle Z (2010) A proposal for a worldwide definition of health resort medicine, balneology, medical hydrology and climatology. Int J Biometeorol 54:495–507. doi:10.1007/s00484-010-0321-5
Heaney JL, Phillips AC, Carroll D (2012) Aging, health behaviors, and the diurnal rhythm and awakening response of salivary cortisol. Exp Aging res 38:295–314. doi:10.1080/0361073X.2012.672134
Hinz A, Daig I, Petrowski K, Brahler E (2012) Mood in the German population: norms of the Multidimensional Mood Questionnaire MDBF. Psychother Psychosom med Psychol 62:52–57. doi:10.1055/s-0031-1297960
Kanitz JL, Reif M, Rihs C, Krause I, Seifert G (2015) A randomised, controlled, single-blinded study on the impact of a single rhythmical massage (anthroposophic medicine) on well-being and salivary cortisol in healthy adults. Complementary Therapies in Medicine 23:685–692. doi:10.1016/j.ctim.2015.07.008
Kirschbaum C, Hellhammer DH (1994) Salivary cortisol in psychoneuroendocrine research: recent developments and applications. Psychoneuroendocrinology 19:313–333
Kraft K (2012) Das Moorbad, ein hochwirksames Modul der Rehabilitationstherapie. Zeitschrift fürPhytotherapie 33:182–184
Marques AH, Silverman MN, Sternberg EM (2010) Evaluation of stress systems by applying noninvasive methodologies: measurements of neuroimmune biomarkers in the sweat, heart rate variability and salivary cortisol. Neuroimmunomodulation 17:205–208. doi:10.1159/000258725
Matousek RH, Dobkin PL, Pruessner J (2010) Cortisol as a marker for improvement in mindfulness-based stress reduction. Complement Ther Clin Pract 16:13–19. doi:10.1016/j.ctcp.2009.06.004
Matzer F, Nagele E, Bahadori B, Dam K, Fazekas C (2014) Stress-relieving effects of short-term balneotherapy—a randomized controlled pilot study in healthy adults. Forschende Komplementarmedizin 21:105–110. doi:10.1159/000360966
Pawlow LA, Jones GE (2005) The impact of abbreviated progressive muscle relaxation on salivary cortisol and salivary immunoglobulin A (sIgA). Applied Psychophysiology and Biofeedback 30:375–387. doi:10.1007/s10484-005-8423-2
Rapoliene L, Razbadauskas A, Salyga J, Martinkenas A (2016) Stress and fatigue management using balneotherapy in a short-time randomized controlled trial evidence-based complementary and alternative medicine. eCAM 2016:9631684. doi:10.1155/2016/9631684
Schaufeli WB, Leiter MP, Maslach CSEJ (1996) Maslach Burnout Inventory-General Survey (MBI-GS). In: Maslach C, Jackson SE, Leiter MP (eds) Maslach burnout Inventory manual, 3rd edn. Consulting Psychologists Press, Palo Alto
Steyer R, Schwenkmezger P, Notz P, Eid M (1997) Der Mehrdimensionale Befindlichkeitsfragebogen (MDBF). Hogrefe, Göttingen
Stier-Jarmer M, Kus S, Frisch D, Sabariego C, Schuh A (2015) Health resort medicine in non-musculoskeletal disorders: is there evidence of its effectiveness? Int J Biometeorol 59:1523–1544. doi:10.1007/s00484-015-0953-6
Stier-Jarmer M, Frisch D, Oberhauser C, Berberich G, Schuh A (2016) The effectiveness of a stress reduction and burnout prevention program—a randomized controlled trial of an outpatient intervention in a health resort setting. Dtsch Arztebl Int 113:781–788. doi:10.3238/arztebl.2016.0781
Toda M, Morimoto K, Nagasawa S, Kitamura K (2006) Change in salivary physiological stress markers by spa bathing. Biomed res 27:11–14
Turpeinen U, Hamalainen E (2013) Determination of cortisol in serum, saliva and urine. Best Pract res Clin Endocrinol Metab 27:795–801. doi:10.1016/j.beem.2013.10.008
Acknowledgements
The study was funded by the Bavarian State Ministry of Health and Care (Grant No. K1-04-00014-2012-EA_BayGA). Applicants in this scheme, in this case the health resort administration of Bad Aibling (AibKur), have to provide a financial contribution of 30% of eligible expenditure. The costs of medical and therapeutic services were covered by Barmer GEK. The funding agencies had no influence on the planning and course of the study or on the evaluation and publication of its findings. We thank Catherine Mason for the linguistic finalization of our manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Stier-Jarmer, M., Frisch, D., Oberhauser, C. et al. Effects of single moor baths on physiological stress response and psychological state: a pilot study. Int J Biometeorol 61, 1957–1964 (2017). https://doi.org/10.1007/s00484-017-1385-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-017-1385-2