
Abstract
Background
Correction of nutritional vitamin deficiency is recommended in children with chronic kidney disease (CKD). The optimal daily dose of vitamin D to achieve or maintain vitamin D sufficiency is unknown.
Methods
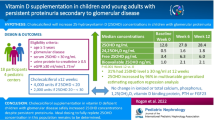
We conducted a phase III, double-blind, randomized trial of two doses of vitamin D3 in children ≥ 9 years of age with CKD stages 3–5 or kidney transplant recipients. Patients were randomized to 1000 IU or 4000 IU of daily vitamin D3 orally. We measured 25-hydroxvitamin D (25(OH)D) levels at baseline, 3 months and 6 months. The primary efficacy outcome was the percentage of patients who were vitamin D replete (25(OH)D ≥ 30 ng/mL) at 6 months.
Results
Ninety-eight patients were enrolled: 49 randomized into each group. Eighty (81.6%) patients completed the study and were analyzed. Baseline plasma 25(OH)D levels were ≥ 30 ng/mL in 12 (35.3%) and 12 (27.3%) patients in the 1000 IU and 4000 IU treatment groups, respectively. At 6 months, plasma 25(OH)D levels were ≥ 30 ng/mL in 33.3% (95% CI: 18.0–51.8%) and 74.4% (95% CI: 58.8–86.5%) in the 1000 IU and 4000 IU treatment groups, respectively (p = 0.0008). None of the patients developed vitamin D toxicity or hypercalcemia.
Conclusions
In children with CKD, 1000 IU of daily vitamin D3 is unlikely to achieve or maintain a plasma 25(OH)D ≥ 30 ng/mL. In children with CKD stages 3–5, a dose of vitamin D3 4000 IU daily was effective in achieving or maintaining vitamin D sufficiency.
Clinical Trial Registration: ClinicalTrials.gov identifier: NCT01909115
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vitamin D has a critical role in bone mineral metabolism [1, 2]. In addition, there is evidence that vitamin D may have an important role in many other areas, including cardiovascular health, immune function, and prevention of autoimmune diseases and certain malignancies [1, 3,4,5,6,7].
In patients with chronic kidney disease (CKD), there are a variety of abnormalities in mineral metabolism that lead to bone disease [8, 9]. Nutritional vitamin D deficiency is widespread in the general population [7, 10] and patients with CKD, with prevalence rates of 60–80% in predialysis children with CKD [3, 11,12,13,14,15]. Observational studies suggest that vitamin D therapy may confer a significant survival advantage for dialysis patients [16,17,18,19].
Guidelines recommend measurement of serum 25-hydroxyvitamin D (25(OH)D) in patients with CKD stages 2 to 5 biannually or annually and correcting nutritional vitamin D deficiency [20, 21]. These guidelines suggest maintaining vitamin D sufficiency, defined as a 25(OH)D level ≥ 30 ng/mL [20, 21]. A variety of different strategies have been utilized for correcting nutritional vitamin D insufficiency or maintaining vitamin D sufficiency in patients with CKD [5, 12, 22]. Many patients do not maintain 25(OH)D levels ≥ 30 ng/mL with current strategies and thus require resource utilization to monitor and treat vitamin D insufficiency.
We hypothesized that a higher proportion of children with CKD stages 3–5 would achieve or maintain 25(OH)D levels ≥ 30 ng/mL on 4000 IU daily of vitamin D compared to 1000 IU daily. We tested this hypothesis in a phase III, single-center, controlled, double-blind, randomized trial.
Methods
We conducted a phase III, single-center, controlled, double-blind, randomized trial comparing 1000 IU with 4000 IU of vitamin D3 per day to determine the proportion of children with CKD stages 3–5 who have vitamin D sufficiency (ClinicalTrials.gov identifier: NCT01909115). The study was funded by a Children’s Healthcare of Atlanta Friends Grant. The Institutional Review Boards of Emory University and Children’s Healthcare of Atlanta approved this study. Patients were recruited from the CKD, transplant, peritoneal dialysis and hemodialysis clinics at Children’s Healthcare of Atlanta. The total treatment period was 6 months, with visits at baseline, 3 months and 6 months.
The inclusion criteria were age 9–21 years, estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 or recipient of a kidney transplant, and ability to swallow pills. The eGFR was determined by the modified Schwartz formula [23]. The exclusion criteria were liver failure, malabsorption, current calcium level > 10.5 mg/dL, hypercalcemia (serum calcium > 11 mg/dL) during the preceding 6 months, current treatment with a medication that may affect vitamin D metabolism (e.g., phenobarbital, phenytoin, rifampin), history of hypervitaminosis D (25(OH)D > 100 ng/mL), on 2000 IU or more of daily vitamin D or completion of a course of high dose vitamin D in the preceding 2 months. We obtained informed written consent from the caregiver or the patient (if ≥ 18 years old) and assent when appropriate.
Patients were allocated in equal proportions to the two treatment arms using a permuted block randomization procedure with variable block sizes of 4, 6, and 8. The sequence was created by the study statistician and shared only with the research pharmacist, who distributed vitamin D to the patient. The vitamin D3 (Bio-Tech Pharmacal, Fayetteville, Arkansas, USA) was repackaged into containers of identical size. The vitamin D3 capsules were of slightly different size, but none of the study personnel opened the containers, and the patients were blinded to this size difference. Patients were asked to stop taking their current vitamin D supplement or vitamin D-containing multivitamins if applicable.
Blood samples for measurement of 25(OH)D were obtained at each study visit. Plasma was stored at –80 C until measurement. Plasma 25(OH)D was measured in a laboratory that participated in the vitamin D external quality assessment schema (DEQAS) using the Immunodiagnostic Systems iSYS automated chemiluminescent system (Gaithersburg, MD). The inter assay CVs of the 25(OH)D measurements in the range of 25(OH)D values for this study was 9.0–9.3% per the manufacturer.
Serum creatinine, calcium, phosphorus, parathyroid hormone, and albumin concentrations were measured in the clinical laboratory. Corrected calcium concentration was calculated using the following formula: corrected calcium (mg/dL) = measured calcium (mg/dL) + 0.8 × [4-measured albumin (g/dL)]. Demographic information, weight and height were obtained from the chart.
The primary outcome was the percentage of patients who were 25-D replete at the 6-month evaluation (defined as a 25(OH)D level ≥ 30 ng/ml). Secondary outcomes were the percentage of patients who were 25(OH)D replete at 3 months, change in 25(OH)D at 3 and 6 months between the groups, and side effects, including hypercalcemia and hypervitaminosis D.
Statistical analysis
We estimated that 70% in the group receiving 4000 IU of vitamin D and 30% in the group receiving 1000 IU of vitamin D would have a 25(OH)D level ≥ 30 ng/mL at 6 months. A sample size of 36 patients in each arm using a two-sided z test with alpha = 0.05 has a power of 90% to detect a difference. Our sample size allowed for 10% drop out.
Statistical significance was set at p < 0.05. For descriptive analysis, continuous data were presented as mean (standard deviation) and categorical data were presented as frequency (percentage). Differences in demographic data between the two treatment arms were assessed using t-tests for continuous data and chi-squared tests (or Fisher’s exact test when appropriate) for categorical data. At each time point, the treatment group differences were examined using chi-squared tests for vitamin D status and t-test for 25(OH)D level and corrected calcium level.
For categorical efficacy response measures of 6 months vitamin D status compared between two treatment groups, a 2-sided Cochran–Mantel–Haenszel test was used, controlling for the baseline vitamin D status. To further understand the association between the change in outcome over time and by treatment, we fitted two linear mixed regression models for outcome 25(OH)D level and corrected calcium as continuous dependent variables, respectively. The model contained fixed effects for measurement time points and treatment, as well as random intercept for each individual to accommodate repeated measurements. We also assessed the interaction between treatment and follow-up time in the longitudinal model to examine whether the difference between treatment changes over time. Statistical analysis and graphics display were performed using R (R version 4.0.2).
The high dose (4000 IU) in this study is the upper limit of dosing recommended by the Institute of Medicine for patients 9 or older [24]. Serum calcium, phosphorus, and albumin (to calculate corrected total calcium level) concentrations were measured at each visit to monitor for vitamin D toxicity. In addition, we measured 25(OH)D level at 3 months to screen for hypervitaminosis D. The study protocol dictated that patients who developed clinical or laboratory evidence of vitamin D toxicity should to be withdrawn from the study.
Results
Ninety-eight subjects were recruited and randomized (49 per treatment arm). We over-enrolled the study due to a higher than expected dropout rate. Eighty (81.6%) patients completed the study and were included in the data analysis. There were 18 patients who did not complete the study, with 13 patients from the 1000 IU group and 5 patients from the 4000 IU group (Fig. 1). None of the 18 patients had follow-up 25(OH)D levels measured.

Patient Flowchart. IU indicates international unit; vitamin D3, cholecalciferol
The analyzed study population had a mean age of 14.5 years and of which 29 were females (36.2%). There were 36 (45%) African American and 31 (38.8%) Caucasian patients (Table 1). The most common etiologies of CKD were congenital anomalies of the kidney and urinary tract (40%) and glomerular disease (35%). The mean baseline 25(OH)D level was 26.8 ng/mL (SD: 10.1 ng/mL), and 24 (30.8%) of the subjects were vitamin D sufficient at baseline, with a 25(OH)D level of ≥ 30 ng/mL. At baseline, 12 (35.3%) and 12 (27.3%) patients in the 1000 IU and 4000 IU groups had 25(OH)D level ≥ 30 ng/mL, respectively (p = 0.607). There were no statistically significant baseline differences in the demographic and laboratory characteristics between the two groups.
The primary outcome, the percentage of patients with 25(OH)D ≥ 30 ng/mL at 6 months, was present in 12 (33.3% (CI: 18.0–51.8%)) and 33 (74.4% (CI: 58.8–86.5%)) patients in the 1000 IU and 4000 IU treatment groups, respectively (Fig. 2; p = 0.0008). At 3 months, 25(OH)D levels were ≥ 30 ng/ml in 40% (CI: 22.7–59.4%) and 75% (CI: 57.8–87.9%) of the patients in the 1000 IU and 4000 IU treatment groups, respectively (Fig. 2; p = 0.009). When comparing 25(OH)D status between 6 months and baseline, there is significant difference between treatments using the Cochran–Mantel–Haenszel test (p = 0.001). Stratifying by the baseline status, the estimated common odds ratio of achieving vitamin D repletion with the 4000 IU versus 1000 IU (95% CI) is 5.25 (1.94–14.22).

Vitamin D Status over Time. Efficacy outcomes are shown according to the study group. The raw percentage (95% confidence interval) of patients who are vitamin D replete (25-hydroxyvitamin D level ≥ 30 ng/mL) are shown at each time point. Note: chi-square test was used. *** Represents p-value < 0.001; ** Represents p-value < 0.01
The 4000 IU treatment group had significantly higher 25(OH)D levels at each visit post-baseline (Fig. 3). The linear mixed regression model for 25(OH)D revealed the significant difference in 25(OH)D levels at 3 months and 6 months between the treatment groups after taking the change of outcome over time into consideration (Table 2). The patients receiving 1000 IU had an increase of 1.10 ng/mL (95% CI: -4.39–6.59, p = 0.695) and 2.02 ng/mL (95% CI: -3.32–7.35, p = 0.459) in 25(OH)D after 3 and 6 months, respectively. A higher increase was observed among patients receiving 4000 IU where it was 15.01 ng/mL (95% CI: 10.08–19.93, p < 0.001) and 14.08 ng/mL (95% CI: 9.42–18.75, p < 0.001) at 3 and 6 months, respectively (Fig. 3).

Vitamin D Levels over Time. Efficacy outcomes are shown according to the study group. The raw mean 25-vitamin D level (95% confidence interval) of patients are shown at each time point. 25(OH)D indicates 25-hydroxyvitamin D. Note: Two sample t-test was used. *** Represents p-value < 0.001; ** Represents p-value < 0.01
There is no significant difference of corrected calcium level between treatment groups observed at any visit post baseline. We removed the interaction between treatment and follow-up time due to insignificance in linear mixed regression model for corrected calcium, indicating that the change of corrected calcium across time was not significantly different between the two groups, with an increase of 0.14 mg/dL (95% CI: -0.10–0.38, p = 0.250) and 0.02 (95% CI: -0.31–0.25, p = 0.868) after 3 and 6 months, respectively. The corrected calcium levels were 0.05 mg/dL higher on average for patients in the 4000 IU treatment group compared to those in the 1000 IU group (95% CI: -0.18–0.28, p = 0.687). We performed a safety check at the 3-month visit, and none of the patients developed a 25(OH)D level > 100 ng/mL.
Discussion
In this phase III, single-center, controlled, double-blind, randomized trial, we found that a daily dose of 4000 IU vitamin D3 resulted in a higher proportion of children with CKD stages 3–5 who had 25(OH)D level in the sufficiency range at 6 months compared to a daily dose of 1000 IU vitamin D3. Our study also suggests that a daily dose of 4000 IU of vitamin D3 is safe in children with CKD because none of the patients in our study developed vitamin D toxicity (25(OH)D level > 100 ng/mL) or hypercalcemia. This study is unique as it has the largest cohort of children with CKD undergoing a randomized controlled trial using two different daily doses of vitamin D therapy.
In our study, 69.2% of children had 25(OH)D insufficiency/deficiency at baseline. The prevalence of 25-D deficiency in adults with CKD 2–4 has been reported at 71–82% and is closely related to CKD stage [10]. There are limited data in children with CKD, but a prevalence of 39–83% has been reported in children with CKD, although differences by CKD stage have been described [11,12,13,14,15].
While the 1000 IU group had only minimal improvement in 25(OH)D levels at the 3- and 6-month visits, patients receiving 4000 IU had a significant increase in 25-D level at 3 months. However, no further increase in 25(OH)D level was noted at 6 months. It is unclear why there is no further increase in the mean 25(OH)D level from the 3-month to the 6-month visits in the 4000 IU group. It is possible that patients achieved a steady-state by 3 months, with degradation equaling intake. Alternatively, it is possible that adherence waned, potentially limiting ongoing increases.
There are few studies comparing different daily maintenance doses of vitamin D in children with CKD. Kari et al. [22] performed an uncontrolled vitamin D3 supplementation trial in vitamin D deficient (25(OH)D < 30 ng/ml) children with CKD stages 2–5 using a daily dose of 2000 IU for 6 months and achieved a repletion rate of only 11%. This supports our results and suggests that doses > 2000 IU daily are needed.
There is also a randomized double-blinded, placebo-controlled study in vitamin D deficient children with CKD stages 2–4 using a dosing strategy per National Kidney Foundation’s 2008 K/DOQI guidelines in the treatment group [5]. They used intensive replacement therapy (based on 25(OH)D level) using vitamin D2 during the first 3 months followed by maintenance dose of 2000 IU daily for the next 3 months. Sixteen of 20 (80%) children achieved 25(OH)D levels in the normal range after intensive replacement treatment (month 3), whereas only 12 of 20 (60%) children continued to have normal 25(OH)D levels after maintenance treatment. In this study, it was more difficult to achieve and maintain normal 25(OH)D levels in CKD stages 3–4 compared with stage 2. This study also supports our findings, suggesting that doses greater than 2000 IU are needed in children with CKD.
A recent study that compared intensive therapy of 3000 IU daily of vitamin D3 with higher weekly and monthly doses for 3 months in patients with CKD stages 2–4 noted a median 25(OH)D level of 44.3 (interquartile range, 34.9, 59.2) at 3 months in the 3000 IU daily group [25]. This study achieved a comparable 25(OH)D level to our study, where the mean 25(OH)D level at 6 months was 40.8 ng/mL (95% CI: 34.4–47.2) in the 4000 IU group. Our study had 45% African Americans, while the above study was performed in South Asia, where there is likely more sun exposure and probably more endogenous vitamin D production in the skin. This might explain why the above study achieved a comparable repletion rate to our population with a lower daily dose of 3000 IU.
Our study has several limitations. Our dropout rate was 18.4%, which was higher than the 10% that we anticipated. However, we enrolled more patients than recommended by the power analysis and were thus still able to achieve statistically significant results. The majority of our patients were transplant recipients. We did not have sufficient patients to achieve statistical significance when analyzing different CKD patient groups, but the responses in dialysis, transplant and pre-dialysis patients were quite similar. This was also a single center study and thus the results may not be generalizable to other populations, especially given variations in sun exposure, skin pigmentation and diet.
We believe that our study and the extant literature suggests that maintenance doses of vitamin D3 ≤ 2000 IU daily are likely to be inadequate in the majority of children with CKD. Our study supports a starting dose of 4000 IU of vitamin D3 for correcting and maintaining normal levels of vitamin D in children with CKD, though monitoring to assure adequate levels is still necessary.
Data availability
De-identified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. The data will be available up to 3 years following article publication. Proposals should be submitted to Larry Greenbaum, MD at lgreen6@emory.edu.
Code availability
Not applicable.
References
Holick MF (2007) Vitamin D deficiency. N Eng J Med 357:266–281
Doyon A, Schmiedchen B, Sander A, Bayazit A, Duzova A, Canpolat N, Thurn D, Azukaitis K, Anarat A, Bacchetta J, Mir S, Shroff R, Yilmaz E, Candan C, Kemper M, Fischbach M, Cortina G, Klaus G, Wuttke M, Köttgen A, Melk A, Querfeld U, Schaefer F (2016) Genetic, environmental, and disease-associated correlates of vitamin d status in children with CKD. Clin J Am Soc Nephrol 11:1145–1153
Shroff R, Knott C, Rees L (2010) The virtues of vitamin D–but how much is too much? Pediatr Nephrol 25:1607–1620
Andress DL (2006) Vitamin D in chronic kidney disease: a systemic role for selective vitamin D receptor activation. Kidney Int 69:33–43
Shroff R, Wan M, Gullett A, Ledermann S, Knott C, Wells D, Aitkenhead H, Manickavasagar B, van't Hoff W, Rees L (2012) Ergocalciferol supplementation in children with CKD delays the onset of secondary hyperparathyroidism: a randomized trial. Clin J Am Soc Nephrol 7:216–223
von Scheven E, Burnham JM (2011) Vitamin D supplementation in the pediatric rheumatology clinic. Curr Rheumatol Rep 13:110–116
Kumar J, Muntner P, Kaskel FJ, Hailpern SM, Melamed ML (2009) Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001–2004. Pediatrics 124:e362–e370
Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL (2007) Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 71:31–38
Bacchetta J, Harambat J, Cochat P, Salusky IB, Wesseling-Perry K (2012) The consequences of chronic kidney disease on bone metabolism and growth in children. Nephrol Dial Transplant 27:3063–3071
LaClair RE, Hellman RN, Karp SL, Kraus M, Ofner S, Li Q, Graves KL, Moe SM (2005) Prevalence of calcidiol deficiency in CKD: a cross-sectional study across latitudes in the United States. Am J Kidney Dis 45:1026–1033
Belostotsky V, Mughal MZ, Berry JL, Webb NJ (2008) Vitamin D deficiency in children with renal disease. Arch Dis Child 93:959–962
Hari P, Gupta N, Hari S, Gulati A, Mahajan P, Bagga A (2010) Vitamin D insufficiency and effect of cholecalciferol in children with chronic kidney disease. Pediatr Nephrol 25:2483–2488
Menon S, Valentini RP, Hidalgo G, Peschansky L, Mattoo TK (2008) Vitamin D insufficiency and hyperparathyroidism in children with chronic kidney disease. Pediatr Nephrol 23:1831–1836
Seeherunvong W, Abitbol CL, Chandar J, Zilleruelo G, Freundlich M (2009) Vitamin D insufficiency and deficiency in children with early chronic kidney disease. J Pediatr 154:906-911.e901
Ali FN, Arguelles LM, Langman CB, Price HE (2009) Vitamin D deficiency in children with chronic kidney disease: uncovering an epidemic. Pediatrics 123:791–796
Kalantar-Zadeh K, Kuwae N, Regidor DL, Kovesdy CP, Kilpatrick RD, Shinaberger CS, McAllister CJ, Budoff MJ, Salusky IB, Kopple JD (2006) Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int 70:771–780
Teng M, Wolf M, Lowrie E, Ofsthun N, Lazarus JM, Thadhani R (2003) Survival of patients undergoing hemodialysis with paricalcitol or calcitriol therapy. N Eng J Med 349:446–456
Tentori F, Hunt WC, Stidley CA, Rohrscheib MR, Bedrick EJ, Meyer KB, Johnson HK, Zager PG (2006) Mortality risk among hemodialysis patients receiving different vitamin D analogs. Kidney Int 70:1858–1865
Wolf M, Shah A, Gutierrez O, Ankers E, Monroy M, Tamez H, Steele D, Chang Y, Camargo CA Jr, Tonelli M, Thadhani R (2007) Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int 72:1004–1013
KDOQI Work Group (2009) KDOQI clinical practice guideline for nutrition in children with CKD: 2008 update. Executive summary. Am J Kidney Dis 53(3 Suppl 2):S11-104
Shroff R, Wan M, Nagler EV, Bakkaloglu S, Fischer DC, Bishop N, Cozzolino M, Bacchetta J, Edefonti A, Stefanidis CJ, Vande Walle J, Haffner D, Klaus G, Schmitt CP (2017) Clinical practice recommendations for native vitamin D therapy in children with chronic kidney disease Stages 2–5 and on dialysis. Nephrol Dial Transplant 32:1098–1113
Kari JA, Eldesoky SM, Bagdadi OT (2012) Vitamin D insufficiency and treatment with oral vitamin D3 in children with chronic kidney disease. Saudi Med J 33:740–744
Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
Institute of Medicine, Food and Nutrition Board (2010) Dietary reference intakes for calcium and vitamin D. National Academies Press, Washington, DC
Iyengar A, Kamath N, Reddy HV, Sharma J, Singhal J, Uthup S, Ekambaram S, Selvam S, Rahn A, Fischer DC, Wan M, Shroff R (2020) Determining the optimal cholecalciferol dosing regimen in children with CKD: a randomized controlled trial. Nephrol Dial Transplant. https://doi.org/10.1093/ndt/gfaa369
Acknowledgements
The Pediatric Research Alliance Biostatistics Core of Emory University and Children’s Healthcare of Atlanta provided biostatistical support. This study was funded by the Friends Fund of Children’s Healthcare of Atlanta. We would also like to thank Priscilla Quach and Margaret Kamel for patient enrollment and research guidance, respectively.
Funding
This study was funded by Friends Grant, Children’s Healthcare of Atlanta.
Author information
Authors and Affiliations
Contributions
Dr. Nadeem conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript.
Drs. Tangpricha and Ziegler provided guidance in the study design, and provided critical review of the manuscript.
James Rhodes performed patient randomization, administered vitamin D medication, and performed critical review of the manuscript.
Dr. Traci Leong and Yijin Xiang organized the data, performed data analysis and provided critical review of the manuscript.
Dr. Greenbaum conceptualized and designed the study, performed data analysis, partially drafted the manuscript and provided critical review of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Approval was obtained from the ethics committee of Emory University and Children’s Healthcare of Atlanta. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from legal guardians and assent from participants when applicable.
Consent for publication
All authors approved the manuscript as submitted and agree to be accountable for all aspects of the work.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nadeem, S., Tangpricha, V., Ziegler, T.R. et al. Randomized trial of two maintenance doses of vitamin D in children with chronic kidney disease. Pediatr Nephrol 37, 415–422 (2022). https://doi.org/10.1007/s00467-021-05228-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-021-05228-z