
Abstract
Background
The correlation between complement activation and severity of hemolytic uremic syndrome related to Shiga toxin–producing Escherichia coli (STEC-HUS) has been examined in few studies, with conflicting results. We investigated whether C3 levels on admission are associated with worse acute outcomes.
Methods
Demographic, clinical, and laboratory variables were compared between dialyzed and non-dialyzed patients and between those with or without extrarenal complications. Univariate and multivariate analyses were performed; odds ratio (OR) and 95% confidence interval (95%CI) were calculated. C3 concentrations were correlated with dialysis length (Spearman test) and ROC curves with area under the curves (AUC) were calculated to identify C3 concentrations able to discriminate patients with dialysis requirements and complicated course.
Results
Among 49 children, 33 had normal and 16 had decreased C3 concentrations. Higher hemoglobin, lactic dehydrogenase, urea and creatinine and lower albumin, sodium, and C3 and C4 concentrations at admission were associated with dialysis requirement; only creatinine remained significant (p = 0.03, OR 2.1, 95%CI 1.34–2.7) by multivariate analysis. Patients with a complicated course presented higher leukocyte count, hemoglobin and lactic dehydrogenase and lower albumin, sodium, and C3 and C4. In the multivariate analysis, leukocyte count (p = 0.02, OR 2.6, 95%CI 1.4–4.3) and C3 concentration (p = 0.039, OR 1.7, 95%CI 1.1–2.73) were independently associated with a complicated disease. C3 levels correlated with dialysis length (r = − 0.42, p = 0.002); nevertheless, they were unable to discriminate dialysis requirement (AUC = 0.25, 95%CI 0.11–0.38) and extrarenal complications (AUC = 0.24, 95%CI 0.11–0.4).
Conclusions
Our study suggests that decreased C3 levels at admission are associated with a more complicated STEC-HUS episode.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hemolytic uremic syndrome related to Shiga toxin–producing Escherichia coli (STEC-HUS) is characterized by the triad of microangiophatic hemolytic anemia, thrombocytopenia, and renal injury [1]. In children, it represents one of the most common etiologies of acute kidney injury; death occurs in 1–5% of patients and around 30% of the survivors demonstrate long-term renal sequelae [1,2,3].
The primary pathogenetic mechanism of the disease is endothelial damage caused by Shiga toxin (Stx) [4]; however, there is increasing evidence for complement activation as a contributing factor for organ damage [5]. Several decades ago, low plasma C3 concentrations and augmented degradation complement products were noticed in children likely to have had STEC-HUS [6,7,8,9]. In 2009, Orth et al. [10] have shown in vitro that high doses of Stx2, far above the concentrations measured in patients [11], induce direct activation of complement alternative pathway (AP), and bind factor H decreasing its activity on the cell surface. In addition, Morigi et al. demonstrated experimentally that Stx triggers complement-dependent microvascular thrombosis [12]. Complement activation was also inferred by the presence of circulating microvesicles derived from platelets, monocytes, and red blood cells bearing C3 and C9 in STEC-HUS patients [13, 14]. More recently, C5b-9 deposits were found in the human kidney during the disease and additional studies revealed that Stx induces complement-mediated injury in glomerular endothelial cell and podocyte [15,16,17].
Despite this substantial amount of findings, only a few clinical studies have correlated complement system activation with clinical course. Furthermore, they presented conflicting results and most of them consisted of small series, or even included patients without microbiological diagnosis [18,19,20,21,22,23,24]. Since 2010, we have incorporated serum C3 determination into the initial laboratory profile in patients with STEC-HUS; thus, we aimed to further explore the association between C3 concentrations on admission and acute outcomes in a large cohort of patients with proven STEC infection.
Material and methods
In this retrospective single-center study, we included patients treated at the Hospital General de Niños Pedro de Elizalde between 2010 and 2017 who met the following criteria: (1) diagnosis of HUS with confirmed STEC infection; (2) age under 18 years old; and (3) C3 levels tested at admission. Exclusion criteria were (1) recurrent or family history of hereditary HUS; (2) HUS associated with systemic diseases such as organ transplantation, systemic lupus erythematosus, pneumococcal infection, or HIV infection; and (3) pre-existing renal disease.
We recorded duration of prodromal phase, demographic characteristics (age, gender, body weight and height), and microbiological test results. Blood laboratory determinations performed at admission and analyzed included white blood cell count (WBC), hemoglobin, platelets count, urea, creatinine, C3 and C4 levels, lactic dehydrogenase (LDH), albumin, and sodium. The C3 and the C4 concentrations were measured by nephelometry (IMMAGE Beckman Coulter, Brea, CA, USA) and the normal reference values ranged within 90–180 mg/dl and 10–40 mg/dl, respectively. To assess the severity of the disease, the following data on care needs was collected: blood product administration, the need for and duration of dialysis, treatment with antihypertensive drugs and intensive care unit admission. Extrarenal complications evaluated were severe bowel or central nervous system (CNS) injury, multiple organ failure, cardiac involvement, pancreatic compromise (pancreatitis and/or diabetes mellitus), and/or death. Additionally, clinical notes were examined at 6 months after the acute phase in order to evaluate long-term renal outcomes. All patients were managed by the same nephrology team according to standard recommendations [1].
Definitions
HUS diagnosis was based on the triad composed by thrombocytopenia (< 150,000/mm3), microangiopathic hemolytic anemia (schistocytes in blood smear), and serum creatinine concentration greater than the upper limit of normal for age (at admission or during the course of the disease) with proteinuria and/or hematuria [1, 25]. STEC infection was evidenced by at least one of these three laboratory criteria: screening by polymerase chain reaction/isolation of STEC, detection of free Stx in stools and, in the last years, by the detection of anti-lipopolysaccharide antibodies O157, O145, and O121 [26]. Indications for dialysis were anuria lasting > 24 h, refractory electrolyte abnormalities, and hypervolemia [27]. Antihypertensive drugs were indicated if the child developed high blood pressure according to the Task Force standards [28]. Major CNS involvement was defined as any symptoms involving seizures, focal deficits, and/or coma [29]. Severe bowel injury was referred to the presence of prolonged bloody diarrhea associated with abdominal distension, pain, tenderness, and cramps usually associated with radiologic or ultrasonographic abdominal abnormalities or pathology findings, such as bowel wall necrosis [30]. Multiple organ failure was defined as the concurrent dysfunction of two or more systems and cardiac involvement as the presence of myocarditis, pericarditis, and arrhythmia [31]. Diagnosis of acute pancreatitis required at least two of three criteria: (1) abdominal pain suggestive of or compatible with acute pancreatitis (i.e., abdominal pain of acute onset, especially in the epigastric region, usually with nausea and vomiting), (2) serum amylase and/or lipase activity at least three times greater than the upper limit of normality, and (3) imaging findings compatible with acute pancreatitis [32]. Diabetes mellitus was defined as hyperglycemia on consecutive days treated with insulin [33]. Chronic kidney disease (CKD) was defined as the presence of at least one of the following findings: estimated glomerular filtration rate < 90 mL/min/1.73 m2 (calculated by the Schwartz formula), abnormal proteinuria or microalbuminuria, or hypertension at 6 months of follow-up [34].
Statistical analysis
Continuous variables were non-normally distributed (Shapiro–Wilk test) and therefore, they were expressed as median values (range) while categorical data was presented as absolute figures and percentages. We have analyzed the association between C3 concentrations at admission and disease severity, considering two main outcomes: (1) the need for dialysis and (2) the presence of extrarenal complications, including death. Univariate analysis was performed in order to identify factors associated with each outcome of interest, using the Wilcoxon test for continuous variables and by chi-square test or Fisher exact test for categorical data. Then, a multivariate logistic regression analysis was performed with those variables previously identified as significant and odds ratio (OR) and 95% confidence intervals (95%CI) were calculated. In addition, the C3 levels were correlated with dialysis length with the Spearman test. Finally we explored by receiver operator curve (ROC) analysis and area under the curve (AUC) determination, with their respective 95%CI, if there was a C3 concentration able to discriminate patients who needed dialysis and who developed a complicated disease form. A p value < 0.05 (two tailed) was considered statistically significant. Data were analyzed using Statistix ver. 7 (IBM version; Analytical Software, Tallahassee, FL) and Medcalc ver. 9.3.2.0 (MedCalc Software, Mariakerke, Belgium).
Results
During the study period, 79 patients were admitted with postdiarrheal HUS, all of them having C3 dosage at admission. None had family or recurrent HUS history or specific causes associated with the disease development. In 49 patients, the STEC infection was evidenced; thus, they constituted the study sample (Fig. 1). The demographic, laboratory, and clinical features of the acute illness of this subgroup were comparable with those with no proven STEC infection and also to the full cohort (data not shown). Two patients were diagnosed with STEC-HUS based on the presence of diarrhea followed by renal injury, microangiopathic hemolytic anemia, and evidence of STEC infection, despite the absence of thrombocytopenia criterion. The clinical courses of these two patients have been extensively described; of note, one of them needed dialysis and their biopsy findings showed signs of thrombotic microangiopathy [35].

Flow of patient selection
Median age of patients was 2.16 years and 24 (49%) were females. Time from first symptoms to STEC-HUS diagnosis was 6 days (1–21); bloody diarrhea was found in 73.4% of cases. By stool culture and/or anti-lipopolysaccharide antibodies, serogroup O157:H7 accounted for 21 cases and O145 and O121 for 3 each. Stx type 2 was positive in 23 children while type 1 was identified in only 1 case.
Patients were grouped according to whether they needed dialysis (n = 28) or not (n = 21). In univariate analysis, demographics characteristics were comparable; in contrast, hemoglobin, urea, creatinine, LDH, albumin, sodium, and C3 and C4 concentrations were significantly different between both groups. In multivariate analysis, only serum creatinine concentration remained significant (Table 1).
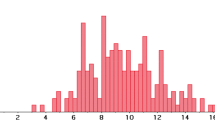
Regarding the treatment received, patients with hypocomplementemia required more acute care needs including red blood cell transfusions, intensive care unit admission, and dialysis requirements (Table 2). They also needed longer periods of dialysis; however, despite having observed a good correlation between the C3 levels and the dialysis length (r = − 0.42, p = 0.002) (Fig. 2), it was not possible to identify an optimal cutoff concentration of C3 (AUC = 0.25, 95%CI 0.11–0.38) able to predict the need for dialysis.

Correlation between C3 levels and dialysis duration in children with Shiga toxin–related hemolytic uremic syndrome
Patients with (n = 16) or without (n = 33) extrarenal complications were also similar in demographics characteristics. Conversely, the former presented a significantly higher WBC count and hemoglobin value at the time of diagnosis and lower albumin, sodium, and C3 and C4 concentrations. By multivariate analysis, WBC count (p = 0.02, OR 2.6, 95%CI 1.4–4.3) and C3 concentrations (p = 0.039, OR 1.7, 95%CI 1.1–2.73) were independently associated with a worse STEC-HUS episode (Table 3). In detail, those with decreased C3 concentrations were more likely to have extrarenal complications, including multiple organ failure and severe CNS and intestinal injury. Patients with cardiac (n = 1; C3 76 mg/dl), pancreatic (n = 1, C3 68 mg/dl), or who died (n = 2, C3 81 mg/dl and 29 mg/dl each) also had reduced C3. However, we did not find a difference between groups which could be related to the sample size, given the rare frequency of these complications. Moreover, they did indeed show CKD more frequently at 6 months of follow-up (Table 2). We have additionally explored the ability of C3 levels to determine a complicated form of the disease, but the AUC was very low (AUC = 0.24, 95%CI 0.11–0.4). Finally, 4 out of 45 children whose C4 levels were measured showed reduced values (all of them had low C3 concentrations also); they had severe extrarenal complications (3 required intensive care and 1 of them died).
Survivor patients normalized the C3 and C4 levels within 1 month after disease onset, except for a girl with persistent low C3 levels for 3 months. In this particular case, thrombotic thrombocytopenic purpura was excluded with a normal ADAMTS 13 activity (104%, normal range: 40–130%), and screening for mutations in the genes encoding complement regulatory proteins (CFH, CFI, CFB, C3, MCP, CFHR 1–5, DGKE, and THBD) and testing for anti-CFH antibodies were negative.
Discussion
Despite the increasing understanding of the role of complement in STEC-HUS physiopathology, clinical data on whether complement activation can influence the course of illness are still scarce. Moreover, a closer analysis of major pediatric studies linking complement activation and disease evolution shows conflicting results (Table 4) [18,19,20,21,22,23,24]. While some of them reported a relationship between elevated activity of complement AP and poor prognosis, other groups either failed in demonstrating such association, showed mixed results (i.e., complement activation predicted dialysis but not CNS injury), or just observed trends towards more severe disease but without reaching statistically significant differences [18,19,20,21,22,23,24]. In the last cases, the small samples analyzed may be responsible for those inconclusive results. It should also be pointed out that in most of the abovementioned studies, biological confirmation of STEC infection was not required to enter in the investigation.
The main result of our study is that decreased C3 concentrations were significantly associated with dialysis requirement and extrarenal complications. Remarkably, hypocomplementemia was an independent determinant of a worse STEC-HUS episode. This finding supports that the clinical outcome depends not only of the direct effects of Stx but also on secondary effects induced by an activated complement system [5, 21]. Consistently, the subset of patients with low C3 levels presented a complicated course and subsequently required more care needs. Similarly to C3 concentrations, multivariate analysis also identified leukocytosis independently associated with a poor prognosis, as already known [36, 37]. Moreover, early work by Robson et al. found an inverse significant correlation between white blood cell count and C3 levels [18]. In univariate analysis, patients with a complicated course exhibited a greater hemoglobin concentration, a surrogate marker of dehydration, a finding repeatedly associated with adverse outcomes [25, 38, 39]. Likewise, they had lower serum sodium levels, a predictor of death recently identified in a multicentric study involving 466 children [26]. The presence of hypoalbuminemia is a common finding in STEC-HUS [40]; nevertheless, in complicated patients, it may also reflect hypercatabolism. Regarding dialysis requirement, dialyzed patients presented lower C3 concentrations compared with those non-dialyzed. However, by multivariate analysis, only creatinine values were independently associated with dialysis. In addition, patients with hypocomplementemia needed dialysis for longer periods. Consistent with this observation, Ferraris and coworkers found higher levels of sC5b-9 and Bb levels in patients presenting with oligoanuira when compared with those non-oliguric [20]. In the same line, in a preliminary study, Karnisova et al. recently reported a significant correlation between the initial C3 concentration and the duration of renal replacement therapy [23], a finding corroborated in our series (Fig. 1). Interestingly, they also identified that patients with C3 < 82.5 mg/dl were more likely to need renal replacement therapy and to have extrarenal complications [23]. In contrast, as also noted by Thurman et al. [19], among our patients, no cutoff value for C3 could be defined in order to discriminate which would require dialysis or suffer complications. Finally, patients with low C3 levels were more likely to develop CKD after 6 months of follow-up; an expected finding since they required longer dialysis, which is the main predictor of renal sequelae [41].
Reduced concentrations of C3 levels were transient returning to normal during convalescent phase, as noted by other authors [19, 20]. It is interesting to stand out that hyperactivation of complement was not found in all subjects. In fact in our patients, this accounts for 32.6%. Earlier studies revealed C3 consumption in half of the patients [8, 9], contrasting with more recent reports, where the percentage was lower. Robson and Alesteil Grunow found a rate of 19% each [18, 21], while others reported a consumption of 28% [22]. In addition, Westra et al. noted decreased C3 levels in 6 (5 slightly and one markedly) out of 22 patients with STEC-HUS (26%), but the median concentration of the full cohort was not significantly different from those of healthy pediatric age-matched controls [42]. Otherwise, Ferraris et al. found elevated C3 levels as well as Frémeaux-Bacchi, the latter also comparing with healthy controls [20, 24]. Here it is worth recognizing that our study lacks data on the complement values provided by a control group. It must also be mentioned that in studies where the breakdown products were assayed, markers of AP activation were seen in a higher proportion of patients [19, 20]. Furthermore, AP activation was detected even when the C3 levels were normal [7, 21, 22].
We additionally noted low concentrations of C4 together with reduced C3 values, in 4 out of 45 patients in whom it was measured. Although decreased C4 levels have been occasionally documented in some patients [9, 21], its significance remains unclear given that currently there is no evidence of activation of classical and/or lectin pathways in STEC-HUS [5, 12, 20]. Alternatively, as these 4 patients were severely affected and C4 is activated in response to infection [43], it could be speculated that they had a greater infection load than others.
In recent years, mutation in the complement genes responsible for atypical HUS has also been detected in STEC-HUS patients. However, the role of these abnormalities has not been completely elucidated yet [21, 42]. Ahlenstiel-Grunow identified a mutation in 3/25 (12%) and Westra in 7/25 (28%) of children with STEC-HUS [21, 42]. In a larger study, Frémeaux-Bacchi identified a rare variant in 12 out of 75 (16%) pediatric Stx-positive patients with HUS, but only 5% of these patients carried a pathogenic variant that is known to impair the complement regulatory activity [24]. In addition, the genetic background did not significantly affect the severity of the acute phase and incident CKD during follow-up [24]. Currently, genetic screening does not seem justified for all patients with postdiarrheal HUS, but should be considered among those who progressed rapidly to end-stage kidney disease or had a relapsing episode or family story of HUS [24]. In our series, none of the patients presented recurrent or familial forms of the disease. Moreover, in a girl with late normalization of C3 level mutation, screening for atypical HUS resulted negative.
So far, treatment of the disease is mainly symptomatic. The involvement of complement AP provided the rationale for terminal complement blockade by eculizumab in this form of thrombotic microangiopathy [2]. This monoclonal antibody effectively blocks cleavage of complement factor C5 inhibiting the formation of the terminal complement complex (C5b-9) [1]. However, as data regarding its efficacy arose from uncontrolled studies with conflicting results, prospective studies are awaited to define whether it might be a therapeutic option [2, 44, 45].
Although our study represents one of the larger series of children with STEC-HUS diagnosed microbiologically that investigate the association between C3 concentrations and disease outcomes, some limitations deserve consideration. The association noted here did not imply causality. In fact, patients with decreased C3 also presented higher hemoglobin reflecting dehydration [25, 38, 39], which could be responsible for the worse disease course. Nevertheless, C3 remained associated with a severe evolution even after the multivariate analysis. Moreover, C3 consumption may indicate complement hyperactivation, which could have biologic plausibility as a contributing factor for such clinical evolution [10, 12,13,14,15,16,17]. Also, as we have measured C3 level rather than complement pathway fragments, it is possible that complement system hyperactivity has not been noticed in some patients. Furthermore, C3 dosages along the disease trajectory were not performed. However, the data presented here could be useful since the C3 determination is readily available in most laboratories facilitating its clinical use.
Conclusion
Our data suggests that children with STEC-HUS with decreased C3 concentrations at admission are more likely to need dialysis and are at increased risk of having serious extrarenal complications.
Change history
30 October 2019
Due to an unfortunate error during the processing of the article, the spelling of the second author name was incorrect.
References
Grisaru S (2014) Management of hemolytic-uremic syndrome in children. Int J Nephrol Renovasc Dis 7:231–239
Percheron L, Gramada R, Tellier S, Salomon R, Harambat J, Llanas B, Fila M, Allain-Launay E, Lapeyraque AL, Leroy V, Adra AL, Bérard E, Bourdat-Michel G, Chehade H, Eckart P, Merieau E, Piètrement C, Sellier-Leclerc AL, Frémeaux-Bacchi V, Dimeglio C, Garnier A (2018) Eculizumab treatment in severe pediatric STEC-HUS: a multicenter retrospective study. Pediatr Nephrol 33(8):1385–1394
Keir LS, Saleem MA (2014) Current evidence for the role of complement in the pathogenesis of Shiga toxin haemolytic uraemic syndrome. Pediatr Nephrol 29(10):1895–1902
Poolpol K, Orth-Höller D, Speth C, Zipfel PF, Skerka C, de Córdoba SR, Brockmeyer J, Bielaszewska M, Würzner R (2014) Interaction of Shiga toxin 2 with complement regulators of the factor H protein family. Mol Immunol 58(1):77–84
Orth-Höller D, Würzner R (2014) Role of complement in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome. Semin Thromb Hemost 40(4):503–507
Kaplan BS, Thomson PD, MacNab GM (1973) Letter: serum-complement levels in haemolytic-uraemic syndrome. Lancet 2(7844):1505–1506
Monnens L, Molenaar J, Lambert PH, Proesmans W, van Munster P (1980) The complement system in hemolytic-uremic syndrome in childhood. Clin Nephrol 13(4):168–171
Cameron JS, Vick R (1973) Letter: plasma-C3 in haemolytic-uraemic syndrome and thrombotic thrombocytopenic purpura. Lancet 2(7835):975
Monnens L, Hendrickx G, van Wieringen P, van Munster P (1974) Letter: serum-complement levels in haemolytic-uraemic syndrome. Lancet 2(7875):294
Orth D, Khan AB, Naim A, Grif K, Brockmeyer J, Karch H, Joannidis M, Clark SJ, Day AJ, Fidanzi S, Stoiber H, Dierich MP, Zimmerhackl LB, Würzner R (2009) Shiga toxin activates complement and binds factor H: evidence for an active role of complement in hemolytic uremic syndrome. J Immunol 182(10):6394–6400
He X, Quiñones B, Loo MT, Loos S, Scavia G, Brigotti M, Levtchenko E, Monnens L (2015) Serum Shiga toxin 2 values in patients during acute phase of diarrhoea-associated haemolytic uraemic syndrome. Acta Paediatr 104(12):e564–e568
Morigi M, Galbusera M, Gastoldi S, Locatelli M, Buelli S, Pezzotta A, Pagani C, Noris M, Gobbi M, Stravalaci M, Rottoli D, Tedesco F, Remuzzi G, Zoja C (2011) Alternative pathway activation of complement by Shiga toxin promotes exuberant C3a formation that triggers microvascular thrombosis. J Immunol 187(1):172–180
Ståhl AL, Sartz L, Karpman D (2011) Complement activation on platelet-leukocyte complexes and microparticles in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome. Blood 117(20):5503–5513
Arvidsson I, Ståhl AL, Hedström MM, Kristoffersson AC, Rylander C, Westman JS, Storry JR, Olsson ML, Karpman D (2015) Shiga toxin-induced complement-mediated hemolysis and release of complement-coated red blood cell-derived microvesicles in hemolytic uremic syndrome. J Immunol 194(5):2309–2318
Arvidsson I, Rebetz J, Loos S, Herthelius M, Kristoffersson AC, Englund E, Chromek M, Karpman D (2016) Early terminal complement blockade and C6 deficiency are protective in enterohemorrhagic Escherichia coli-infected mice. J Immunol 197(4):1276–1286
Zoja C, Buelli S, Morigi M (2019) Shiga toxin triggers endothelial and podocyte injury: the role of complement activation. Pediatr Nephrol 34(3):379–388
Ehrlenbach S, Rosales A, Posch W, Wilflingseder D, Hermann M, Brockmeyer J, Karch H, Satchell SC, Würzner R, Orth-Höller D (2013) Shiga toxin 2 reduces complement inhibitor CD59 expression on human renal tubular epithelial and glomerular endothelial cells. Infect Immum 81(8):2678–2685
Robson WL, Leung AK, Fick GH, McKenna AI (1992) Hypocomplementemia and leukocytosis in diarrhea-associated hemolytic uremic syndrome. Nephron 62(3):296–299
Thurman JM, Marians R, Emlen W, Wood S, Smith C, Akana H, Holers VM, Lesser M, Kline M, Hoffman C, Christen E, Trachtman H (2009) Alternative pathway of complement in children with diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol 4(12):1920–1924
Ferraris JR, Ferraris V, Acquier AB, Sorroche PB, Saez MS, Ginaca A, Mendez CF (2015) Activation of the alternative pathway of complement during the acute phase of typical haemolytic uraemic syndrome. Clin Exp Immunol 181(1):118–125
Ahlenstiel-Grunow T, Hachmeister S, Bange FC, Wehling C, Kirschfink M, Bergmann C, Pape L (2016) Systemic complement activation and complement gene analysis in enterohaemorrhagic Escherichia coli-associated paediatric haemolytic uraemic syndrome. Nephrol Dial Transplant 31:1114–1121
Ağbaş A, Göknar N, Akıncı N, Yıldırım ZY, Taşdemir M, Benzer M, Gökçe İ, Candan C, Küçük N, Uzuner S, Özçelik G, Demirkol D, Sever L, Çalışkan S (2018) Outbreak of Shiga toxin-producing Escherichia-coli-associated hemolytic uremic syndrome in Istanbul in 2015: outcome and experience with eculizumab. Pediatr Nephrol 33(12):2371–2381
Karnisova L, Hradsky O, Blahova K, Fencl F, Dolezel Z, Zaoral T, Zieg J (2018) Complement activation is associated with more severe course of diarrhea-associated hemolytic uremic syndrome, a preliminary study. Eur J Pediatr 177(12):1837–1844
Frémeaux-Bacchi V, Sellier-Leclerc AL, Vieira-Martins P, Limou S, Kwon T, Lahoche A, Novo R, Llanas B, Nobili F, Roussey G, Cailliez M, Ulinski T, Deschênes G, Alberti C, Weill FX, Mariani P, Loirat C (2019) Complement gene variants and Shiga toxin-producing Escherichia coli-associated hemolytic uremic syndrome: retrospective genetic and clinical study. Clin J Am Soc Nephrol 14(3):364–377
Balestracci A, Martin SM, Toledo I, Alvarado C, Wainsztein RE (2012) Dehydration at admission increased the need for dialysis in hemolytic uremic syndrome children. Pediatr Nephrol 27(8):1407–1410
Alconcher LF, Coccia PA, Suarez ADC, Monteverde ML, Perez Y, Gutiérrez MG, Carlopio PM, Missoni ML, Balestracci A, Principi I, Ramírez FB, Estrella P, Micelli S, Leroy DC, Quijada NE, Seminara C, Giordano MI, Hidalgo Solís SB, Saurit M, Caminitti A, Arias A, Rivas M, Risso P, Liern M (2018) Hyponatremia: a new predictor of mortality in patients with Shiga toxin-producing Escherichia coli hemolytic uremic syndrome. Pediatr Nephrol 33(10):1791–1798
Balestracci A, Meni Battaglia L, Toledo I, Martin SM, Alvarado C (2018) Blood urea nitrogen to serum creatinine ratio as a prognostic factor in diarrhea-associated hemolytic uremic syndrome: a validation study. Eur J Pediatr 177:63–68
Flynn JT, Kaelber DC, Baker-Smith CM, SUBCOMMITTEE ON SCREENING AND MANAGEMENT OF HIGH BLOOD PRESSURE IN CHILDREN et al (2017) Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140(3):e20171904
Nathanson S, Kwon T, Elmaleh M, Charbit M, Launay EA, Harambat J, Brun M, Ranchin B, Bandin F, Cloarec S, Bourdat-Michel G, Piètrement C, Champion G, Ulinski T, Deschênes G (2010) Acute neurological involvement in diarrhea-associated hemolytic uremic syndrome. Clin J Am Soc Nephrol 5(7):1218–1228
Rahman RC, Cobeñas CJ, Drut R, Amoreo OR, Ruscasso JD, Spizzirri AP, Suarez Adel C, Zalba JH, Ferrari C, Gatti MC (2012) Hemorrhagic colitis in postdiarrheal hemolytic uremic syndrome: retrospective analysis of 54 children. Pediatr Nephrol 27(2):229–233
Goldstein B, Giroir B, Randolph A, International Consensus Conference on Pediatric Sepsis (2005) International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 6(1):2–8
Srinath AI, Lowe ME (2013) Pediatric pancreatitis. Pediatr Rev 34(2):79–90
Suri RS, Clark WF, Barrowman N, Mahon JL, Thiessen-Philbrook HR, Rosas-Arellano MP, Zarnke K, Garland JS, Garg AX (2005) Diabetes during diarrhea-associated hemolytic uremic syndrome: a systematic review and meta-analysis. Diabetes Care 28(10):2556–2562
KDIGO CKD Work Group (2013) KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl:1–150
Balestracci A, Toledo I, Meni Battaglia L, de Lillo L, More N, Cao G, Alvarado C (2017) Postdiarrhoeal haemolytic uraemic syndrome without thrombocytopenia. Nefrologia 37(5):508–514
Oakes RS, Siegler RL, McReynolds MA, Pysher T, Pavia AT (2006) Predictors of fatality in postdiarrheal hemolytic uremic syndrome. Pediatrics 117:1656–1662
Mody RK, Gu W, Griffin PM, Jones TF, Rounds J, Shiferaw B, Tobin-D’Angelo M, Smith G, Spina S, Hurd S, Lathrop S, Palmer A, Boothe E, Luna-Gierke RE, Hoekstra RM (2015) Post diarrheal hemolytic uremic syndrome in United States children: clinical spectrum and predictors of in-hospital death. J Pediatr 166:1022–1029
Ardissino G, Daccò V, Testa S, Civitillo CF, Tel F, Possenti I, Belingheri M, Castorina P, Bolsa-Ghiringhelli N, Tedeschi S, Paglialonga F, Salardi S, Consonni D, Zoia E, Salice P, Chidini G (2015) Hemoconcentration: a major risk factor for neurological involvement in hemolytic uremicsyndrome. Pediatr Nephrol 30(2):345–352
Grisaru S, Xie J, Samuel S, Hartling L, Tarr PI, Schnadower D, Freedman SB, Alberta Provincial Pediatric Enteric Infection Team (2017) Associations between hydration status, intravenous fluid administration, and outcomes of patients infected with Shiga toxin-producing Escherichia coli: a systematic review and meta-analysis. JAMA Pediatr 171(1):68–76
Serebruany VL, Christenson MJ, Pescetti J, McLean RH (1993) Hypoproteinemia in the hemolytic-uremic syndrome of childhood. Pediatr Nephrol 7(1):72–73
Spinale JM, Ruebner RL, Copelovitch L, Kaplan BS (2013) Long-term outcomes of Shiga toxin hemolytic uremic syndrome. Pediatr Nephrol 28(11):2097–2105
Westra D, Volokhina EB, van der Molen RG, van der Velden TJ, Jeronimus-Klaasen A, Goertz J, Gracchi V, Dorresteijn EM, Bouts AH, Keijzer-Veen MG, van Wijk JA, Bakker JA, Roos A, van den Heuvel LP, van de Kar NC (2017) Serological and genetic complement alterations in infection-induced and complement-mediated hemolytic uremic syndrome. Pediatr Nephrol 32(2):297–309
Charchaflieh J, Rushbrook J, Worah S, Zhang M (2015) Activated complement factors as disease markers for Sepsis. Dis Markers 2015:382463
Lapeyraque AL, Malina M, Fremeaux-Bacchi V, Boppel T, Kirschfink M, Oualha M, Proulx F, Clermont MJ, Le Deist F, Niaudet P, Schaefer F (2011) Eculizumab in severe Shiga-toxin-associated HUS. N Engl J Med 364(26):2561–2563
Keenswijk W, Raes A, Vande Walle J (2018) Is eculizumab efficacious in Shigatoxin-associated hemolytic uremic syndrome? A narrative review of current evidence. Eur J Pediatr 177(3):311–318
Acknowledgments
The authors thank Mrs. Susana Basavilbaso for her kind assistance while conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics
The study was performed in accordance with the ethical standards of the institutional research and ethics committee (IRB 186/18).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Balestracci, A., Meni Bataglia, L., Toledo, I. et al. C3 levels and acute outcomes in Shiga toxin–related hemolytic uremic syndrome. Pediatr Nephrol 35, 331–339 (2020). https://doi.org/10.1007/s00467-019-04334-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-019-04334-3