
Abstract
Background
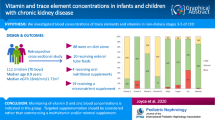
There are few recent data regarding blood micronutrient concentrations and supplementation in children on maintenance dialysis. We investigated micronutrient concentrations following dialysis commencement.
Methods
Retrospective review, including all children on maintenance dialysis (peritoneal dialysis, PD; intermittent haemodialysis, IHD), for nutritional blood concentrations measured over the first 12 months. Patients received pyridoxine and Dialyvit® daily with planned 3-monthly micronutrient concentration monitoring including selenium, manganese, copper, zinc, folate and vitamins A, D, B12 and E.
Results
We reviewed 47 children (24 girls) including 19 PD and 28 IHD, median age (IQR) 11.4 (2.8,14.4) years. 33 were white, 5 Asian, 5 black and 4 of other ethnic origins. Vitamin A, B12 and E concentrations were within range in 6%, 20% and 13% respectively, with all others above normal range. Serum folate and vitamin D concentrations were within the desired range of 55%, with the rest above or below target. For trace elements, 37%, 60%, 65% and 89% achieved normal ranges for zinc, manganese, copper and selenium respectively. Deficiencies were seen for zinc (43%), copper (28%), folate (6%) and selenium (4%), whereas 7%, 7%, 20% and 40% had copper, selenium, zinc and manganese levels above normal ranges. Despite standard pyridoxine supplementation, only 6 children were monitored during the study period.
Conclusions
Concentrations of several trace elements and vitamins were outside reference ranges. Response to systematic monitoring and targeted supplementation should be evaluated in future studies. Paediatric dialysis centres should consider undertaking routine nutritional bloods monitoring, particularly for vitamin D, zinc and copper.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Little is known about the micronutrient requirements and supplementation needs of children requiring long-term dialysis. It is acknowledged that patients with chronic kidney disease (CKD) and those on maintenance dialysis (peritoneal dialysis, PD; intermittent haemodialysis, IHD) are at risk of vitamin and mineral deficiencies as a result of abnormal renal metabolism, inadequate intake, poor gastrointestinal absorption and dialysis-related losses [1, 2]. As the most frequently observed vitamin disturbances are related to water-soluble vitamins, the K/DOQI guidelines recommend that children with CKD on dialysis receive a water-soluble vitamin supplement [2].
Several studies have evaluated the nutritional blood concentrations in children receiving maintenance dialysis. However, results and recommendations from these studies are not consistent [3,4,5,6]. It is likely that different dialysis modalities result in differential losses of micronutrients, but there are few data comparing these in children. Clinical practice with regards to micronutrient supplementation in the UK remains variable. A brief survey conducted by our department in early 2015, investigating practice in 13 paediatric dialysis units in the UK and Ireland, confirmed that only 4 units supplement with a multivitamin and 2 of these only supplemented patients on peritoneal dialysis (PD) and none on IHD. Supplementation of trace elements was not performed routinely in any unit (unpublished data).
At the time of this study, children on maintenance dialysis at the Evelina London Children’s Hospital (ELCH) received supplementation with pyridoxine (vitamin B6) and the renal nutritional supplement Dialyvit®. The latter contains pantothenic acid, folic acid (1 mg), biotin, copper (0.8 mg), zinc (8 mg) and vitamins B1, B2, B3, B6 (2 mg), B12 (1 μg), C, E (3 IU) and K. Children under 5 years received ½ caplet daily and those over 5 years received 1 caplet daily. We plan to monitor nutritional blood levels every 3 months and include measurement of selenium, manganese, copper, zinc, folate and vitamins A, D (25 hydroxy vitamin D), B12 and E. Our objective in this study was to describe the blood concentrations of trace elements and vitamins in children on maintenance dialysis.
Materials and methods
We performed a retrospective review of nutritional blood concentrations in children on maintenance dialysis over a recent 4-year period (2011–2014) at our unit. The average values of vitamin and trace element measurements performed over the first 12 months following commencement of dialysis during the study period were calculated for each patient. Additional data collected included patient demographics, primary renal diagnosis, modality at the start of dialysis and change in modality over the first 12 months following commencement of dialysis. All measurements were obtained using electronic patient records.
Data are displayed as mean (SD), median and interquartile (IQR) range as appropriate for all children on dialysis. The total number of measurements for reported vitamins and trace elements are recorded and shown as median (IQR) number of measurements in each child. For each child, the mean value of all measurements performed was calculated for each reported vitamin and trace element. The average (SD) values across all patients were calculated and reported as summary statistics. Values were reported as “above”, “within range” or “normal” and “below” for all reported micronutrients.
Results
There were a total of 47 patients on maintenance dialysis during the study period, with 28 of the 47 children starting on IHD. Six children changed modality, all from PD to IHD, 1 child <1 month, 3 children 3–6 months and 2 children 6–9 months following commencement of dialysis.
Twenty-three of the 47 children received either an oral nutritional supplement or an enteral feed either for part or during the entire duration of the study. Patient characteristics at the start of renal replacement therapy (RRT) are shown in Table 1.
Most children (n = 45) had ≥1 vitamin and/or trace element abnormality and 64% (n = 30) had both ≥1 vitamin and trace element abnormalities (n = 24, 51%, if vitamin D, which is often low in CKD, was excluded). Mean (SD) vitamin and trace element concentrations and the total number of measurements for each reported vitamin and trace element are shown in Table 2. The percentage of mean vitamin and trace element concentrations below, within and above their reference ranges are shown in Fig. 1. The laboratory reference ranges for vitamin and trace element concentrations used at our unit are shown in Table 3.

Percentage of mean vitamin and trace element concentrations that were below, within and above their reference ranges
Vitamin and trace element supplementation
Vitamin D concentrations (n = 44 out of 47) were within the desired range for 55% (n = 24 out of 44) of patients, the rest having deficient (n = 5, 11%) or insufficient (n = 15, 34%) concentrations. Information on vitamin D supplementation with cholecalciferol was available for 46 patients and 41% (n = 19 out of 46) of these were prescribed cholecalciferol at some point during the study period.
Apart from the patient who was taking Forceval® (containing 50 μg selenium and 3 mg manganese in each tablet), there was no evidence that any other patient was receiving a selenium- or manganese-containing supplement during the study period. This patient’s selenium blood concentration was within the normal range and received 111% of their RNI for selenium from the Forceval® supplement. There is no RNI for manganese.
The proportion of children taking micronutrient supplements and their distribution by dialysis modality across the low, medium, and high blood micronutrient concentrations are shown in Table 4 and Fig. 2 respectively. Dialyvit® provided between 83 and 250% of the RNI for vitamin B12 and 5 to 20 times the RNI for folic acid in children with high concentrations of these vitamins. Three of the children (RNI 70 μg to 200 μg per day) with high folate concentrations were taking folic acid (2.5 mg to 10 mg once daily) in addition to Dialyvit®.

Percentage of mean vitamin and trace element concentrations, which were below, within and above their reference ranges for haemodialysis (HD) and peritoneal dialysis (PD) patients
Most patients (n = 36 out of 47) were prescribed pyridoxine (5 mg to 12.5 mg daily). Blood concentrations were available for only 6 of these patients and all exceeded their RNIs for vitamin B6 from pyridoxine alone.
In the children with zinc deficiency who were taking Dialyvit®, this supplement provided between ~84 and 200% of their RNI (4–9 mg/day) and 4 of these children were also taking Solvazinc® (one tablet three times per week to one tablet daily). Each Solvazinc® tablet contained the equivalent of 45 mg elemental zinc. Although two others were not taking Dialyvit®, they were receiving either Solvazinc® (one tablet three times per week, equivalent to ~19 mg/day zinc with an RNI of 6.5 mg/day) or Wellbaby multivitamin liquid® (5 ml daily, which contained 2.5 mg zinc, equivalent to 50% of the RNI for zinc). Dialyvit® provided 84–114% of the RNI for zinc in the children with high zinc concentrations.
Three-quarters of patients with low copper concentrations (n = 9 out of 12) were prescribed Dialyvit®, which provided 80–100% RNI. Another child was taking one Forceval® daily (2,000 μg copper), which provided 250% of their RNI.
Discussion
In this study of children on maintenance dialysis, we observed abnormal vitamin and mineral concentrations. Most of the patients displayed high blood concentrations of vitamins A (94%), E (87%), B12 (80%) and folate (39%). Three children were taking a vitamin A-containing supplement (Forceval®/Wellbaby multivitamin liquid®/ABIDEC®) during the study period; however, vitamin A concentrations were not available for these children. It is known that vitamin A is not removed by dialysis and high levels can lead to hypercalcaemia, anaemia and hyperlipidaemia [2]. Excess vitamin E has been associated with bleeding and impaired leukocyte function, and previous data have highlighted the low levels of α-tocopherol in dialysis effluent [2].
The effect of excess vitamin B12 levels is unknown [2]. The K/DOQI [2] reports that studies in paediatric dialysis patients have demonstrated normal cobalamin levels regardless of whether they receive supplements or not, and noted further studies that show that dietary intake meets or exceeds requirements in most cases. Our results also demonstrated high vitamin B12 (80%) concentration levels regardless of whether patients were receiving micronutrient supplements containing vitamin B12 or not.
Most patients (77%) were prescribed pyridoxine. However, only 6 patients had vitamin B6 monitoring during the study period and all had high vitamin B6 concentrations. Excess vitamin B6 is known to cause neuropathy and photosensitivity [2]. Following this study, we investigated vitamin B6 levels in our current dialysis group. Fourteen patients had vitamin B6 levels blood concentrations available, 12 of whom were prescribed pyridoxine. Most (n = 12 out of 14) had levels above the reference range, which in 4 patients were 4–5 times (442.9–616.7 nmol/L) above the reference range.
Folate concentrations were high in 39% of our patients and all were receiving a supplement containing folate (Dialyvit®/folic acid). Rees and Shaw [7] reported that daily recommended intakes of vitamin B6 and folate may be met from food, feeds and nutritional supplements and highlighted the importance of assessing dietary contribution before routinely giving supplements. It is acknowledged that vitamin D deficiency is common in children with CKD [2]. Only 55% of our patients had sufficient vitamin D concentrations.
A small paediatric study (n = 12) by Don et al. [6] reported adequate dietary intakes of vitamins B1, B2, B6 and B12 with normal to high blood concentrations in their dialysis patients. They concluded that supplementation of B vitamins was not indicated. Kriley and Warady [3] examined the vitamin status of 8 children receiving PD who were also prescribed a multivitamin containing vitamins B1, B2, B6, B12, C and folate. From diet alone, most met the recommended daily allowance (RDA) for height/age for vitamins B6 (97%), B1 (93%), A (130%), B2 (82%), C (131%), B12 (210%) and folate (169%). Despite the combination of diet and supplementation exceeding the RDA for numerous micronutrients, including vitamin C (259%), B1 (245%), B2 (232%), vitamin B12 (735%), vitamin B6 (893%) and folate (1072%) and increased vitamin stores compared with controls (n = 6, no medical issues), the authors recommended vitamin supplementation, as there were no clinical signs of vitamin toxicity.
Low serum levels of zinc are known to result from its removal by dialysis and deficiency can result in anorexia, impaired wound healing and faltering growth [2, 8]. The K/DOQI [2] recommends that children should receive the recommended dietary zinc intakes and only supplement for the treatment of clinical manifestations of deficiency confirmed by the laboratory. Although 43% of our patients had zinc deficiency, 90% (n = 18 out of 20) were receiving zinc or a zinc-containing supplement, without which their zinc levels could have been lower.
It is known that selenium is normally excreted by the kidney and not removed by dialysis [2]. In our study, most had adequate selenium blood concentrations (89%) and only 2 patients had low selenium concentrations. Copper deficiency can have a negative impact upon growth [2]. The K/DOQI [2] noted that assessment of serum copper levels may be beneficial when clinical signs of overload or deficiency are present. Deficient copper levels were seen in 28% (n = 12 out of 43) of our patients despite most (n = 9 out of 12) receiving the copper-containing supplement Dialyvit®. Given the result of this study, regular blood levels may be beneficial to help guide if and when copper supplementation is required.
Our results showed that 40% had high manganese blood levels. It has been reported previously that the homeostatic mechanisms regulating manganese excretion may not be fully developed in children [9]. It has also been reported that children with iron deficiency anaemia have higher blood concentrations of manganese, although the underlying reasons for this association remain unclear [10, 11]. Anaemia and iron deficiency are highly prevalent in children on dialysis [12], but as we did not collect any data on this in our study cohort we are unable to comment on this further.
It is important to highlight that although reported here, RNI apply to the healthy general population and it may be misleading to compare children on dialysis against these suggested intakes [2]. In this report, we did not include diet assessment retrospectively, as reliance on dietary recall as a method of assessing micronutrient intake has numerous limitations. These include misreporting of food portion sizes, errors in the recall of the child’s food intake and parents often lack knowledge of their child’s dietary intake outside of the home setting. Furthermore, prolonged recording may be required to characterize the intakes of many nutrients in children, for example, >20 days of records are often required to capture habitual vitamin intake [13, 14].
There are several limitations to our study findings beyond those inherent in retrospective data analysis, and include: 1. We did not collect data regarding tolerance of prescribed feeds; in the youngest children with ESRD, who often experience most feeding difficulties, this may be of most relevance. 2. Several micronutrients have age-specific ranges that make interpretation of concentrations as shown difficult. Although age standardization would be useful, we were not aware of reference data that would allow this to be done. 3. It would be of interest to measure changes in concentrations over time. 4. Variability in adherence to prescribed micronutrient supplements and different haemodialysis membranes may also have contributed to variability in measured levels. 5. Most of our results relate to haemodialysis with more limited patient numbers and data in those on PD making it difficult to compare findings between modalities.
Conclusions
The results of this study show that most patients displayed high blood concentrations of vitamins A and B12, that monitoring of vitamin D, zinc and copper is required owing to the low levels seen in this group, and that routine vitamin B6 supplementation is currently not indicated in our dialysis patients. Reasons for the variations in the nutritional blood concentrations may include differences in diet, micronutrient supplementation, micronutrient content in enteral/oral feeds and the impact of dialysis and modality on micronutrient clearance. Further research is required to assess the response to systematic monitoring and targeted supplementation of micronutrients following commencement of dialysis and whilst on longer term dialysis, and to investigate the impact of different dialysis techniques and modalities. Paediatric dialysis centres should consider undertaking routine monitoring of nutritional bloods, particularly for vitamin D, zinc and copper.
References
Locatelli F, Fouque D, Heimburger O, Drüeke TB, Cannata-Andía JB, Hörl WH, Ritz E (2002) Nutritional status in dialysis patients: a European consensus. Nephrol Dial Transplant 17:563–572
National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) (2009) Clinical practice guideline for nutrition in children with CKD: 2008 update. Am J Kidney Dis 53 [Suppl 2]:S1–124
Kriley M, Warady BA (1991) Vitamin status of pediatric patients receiving long term peritoneal dialysis. Am J Clin Nutr 53:1476–1479
Coleman JE, Watson AR (1992) Micronutrient supplementation in children on continuous cycling peritoneal dialysis (CCPD). Adv Perit Dial 8:396–401
Warady BA, Kriley M, Alon U, Hellerstein S (1994) Vitamin status of infants receiving long-term peritoneal dialysis. Pediatr Nephrol 8:354–356
Don T, Friedlander S, Wong W (2010) Dietary intakes and biochemical status of B vitamins in a group of children receiving dialysis. J Ren Nutr 20:23–28
Rees L, Shaw V (2007) Nutrition in children with CRF and on dialysis. Pediatr Nephrol 22:1689–1702
Tamura T, Vaughn WH, Waldo FB, Kohaut EC (1989) Zinc and copper balance in children on continuous ambulatory peritoneal dialysis. Pediatr Nephrol 3:309–313
Oulhote Y, Mergler D, Bouchard MF (2014) Sex- and age-differences in blood manganese levels in the U.S. general population: national health and nutrition examination survey 2011–2012. Environ Health 13:1–10
Kim Y, Park S (2014) Iron deficiency increases blood concentrations of neurotoxic metals in children. Korean J Pediatr 57:345–350
Smith EA, Newland P, Bestwich KG, Ahmed N (2013) Increased whole blood manganese concentrations observed in children with iron deficiency anaemia. J Trace Elem Med Biol 27:65–69
Babitt JL, Lin HY (2012) Mechanisms of anaemia in CKD. J Am Soc Nephrol 23:1631–1634
Rutishauser IHE (2005) Dietary intake measurements. Public Health Nutr 8:1100–1107
Livingstone MBE, Robson PJ, Wallace JMW (2004) Issues in dietary intake assessment of children and adolescents. Br J Nutr 92(S2):S213–S222
Acknowledgements
The author MDS acknowledges financial support from the Department of Health via the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s & St Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College Hospital NHS Foundation Trust.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors confirmed that as this was a retrospective analysis evaluating results of clinical investigations no consent from patients was indicated.
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Joyce, T., Court Brown, F., Wallace, D. et al. Trace element and vitamin concentrations in paediatric dialysis patients. Pediatr Nephrol 33, 159–165 (2018). https://doi.org/10.1007/s00467-017-3773-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-017-3773-6