
Abstract
Background
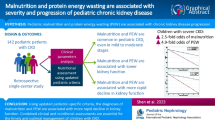
In adults with chronic kidney disease (CKD), protein-energy wasting (PEW) is a risk factor for hospitalization and death. However, PEW in children with CKD is not well characterized or defined.
Methods
Using data from the Chronic Kidney Disease in Children study, we assessed three alternate definitions of PEW using biochemical parameters, body and muscle mass measurements, and reported appetite as described in adults: (1) a minimal PEW definition (≥2 of the four criteria); (2) a standard PEW definition (≥3 of the four criteria); (3) a modified PEW definition (≥3 of the four criteria plus a pediatric-focused criterion of short stature or poor growth).
Results
Of the 528 children analyzed in this study (median age 12 years, median glomerular filtration rate 45 mL/min/1.73 m2, 39 % female, 18 % African American), 7–20 % met the spectrum of definitions for PEW. The unadjusted incidence rates for incident hospitalizations were 1.9-, 2.1-, and 2.2-fold higher for those children diagnosed with PEW using the minimal, standard, and modified definitions, respectively (P = 0.08, 0.09 and 0.03). Following adjustment, only the modified PEW definition, which added short stature or poor growth as a criterion, showed modest significance (P = 0.06).
Conclusions
The inclusion of a criterion based on growth may augment the definition of PEW and improve risk discrimination in children with CKD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In adults with chronic kidney disease (CKD), especially end-stage renal disease (ESRD), protein-energy wasting (PEW) is highly prevalent and has been implicated as a risk factor for death and accelerated atherosclerotic cardiovascular disease. Using classic measures of nutritional status, evidence of wasting is present in 18–75 % of adult maintenance dialysis patients [1]. PEW occurring in adults with CKD is characterized by four primary components: biochemical criteria such as low serum albumin or low cholesterol, reduced body mass, reduced muscle mass, and decreased protein intake [2]. Although several lines of evidence suggest PEW also exists in the pediatric CKD population, the syndrome is less well characterized in children. Low serum albumin is associated with higher all-cause mortality in children with ESRD [3] as it is with all-cause mortality and cardiovascular disease in adults [4–6]. Low body mass as assessed by the body mass index (BMI) has been associated with higher mortality in children with ESRD [7] and in adult CKD patients [8–10]. In a cross-sectional study of children at various stages of CKD by Foster et al., body composition assessed by dual-energy X-ray absorptiometry (DEXA) demonstrated significant deficits in leg lean mass in children with advanced CKD on dialysis [11].
Although evidence from these studies is suggestive of a syndrome of PEW in childhood CKD similar to that in adults, criteria for diagnosing this syndrome in children have not been evaluated. We therefore sought to assess the clinical components thought to be important for diagnosing PEW and compare the performance of three classifications of PEW in predicting clinical outcomes in a prospective cohort of children with CKD.
Methods
Study participants and design
The Chronic Kidney Disease in Children (CKiD) study has been described previously [12]. Briefly, children with mild to moderate CKD (30–90 mL/min per 1.73 m2) based on the original Schwartz formula [13–15] were recruited from 43 participating pediatric nephrology centers. Eligible subjects were those aged 1–16 years who had never been dialyzed or undergone organ transplant. Demographic characteristics and clinical measurements were collected at annual visits. Glomerular filtration rate (GFR) was determined from plasma iohexol disappearance curves at baseline, 1 year later, and every other year thereafter, following methods that have been previously described [16]. GFR values unattainable through direct measurement were estimated using the CKiD equation [17, 18]. Baseline for the current analysis was the second annual visit.
Anthropometry and tanner staging
Age- and sex-specific Z scores for height and weight were calculated using National Center for Health Statistics 2000 Center for Disease Control growth data [19]. BMI-for-height-age and sex Z scores were also calculated, as recommended in the 2008 National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) nutrition guidelines [20]; height-age is the age at which the child’s height is at the 50th percentile. The mid-upper arm circumference (MUAC) was taken as the mean of three measurements when available and expressed relative to height-age- and sex-stratified norms obtained from the National Health and Nutrition Examination Survey 2007–2008 sample [21]. Skinfold thickness data were not available from the cohort, but very few of the patients had clinically significant edema (N = 15, 3 %) at the second annual visit. Pubertal status was dichotomized into Stage 1 and >Stage 1, with the stages defined by Tanner [22].
Biomarker assays
At the study visit where the iohexol GFR was measured, an intravenous line or butterfly needle was used to administer 5 ml of iohexol. A second intravenous line was saline locked and used for obtaining blood samples for biomarker measurements. Blood samples were collected at four time points (10, 30, 120, and 300 min) following the infusion of iohexol (GE Healthcare, Amersham Division, Princeton, NJ) with the iohexol concentration determined by high-performance liquid chromatography. Body surface area for GFR standardization was determined using the formula of Haycock et al. [23]. Inflammation was assessed with wide-range C-reactive protein (CRP). Cystatin C was measured using a Siemens BN II nephelometer (Siemens Diagnostics, Tarrytown NY), and serum creatinine (enzymatic) and serum total cholesterol (TC) were analyzed—following an overnight fast—at a central location (CKiD laboratory at the University of Rochester Medical Center) on a Bayer Advia 2400 (Siemens Diagnostics). Assay results were entered by the Central Biochemistry Laboratory into a web-based data management system (Nephron) developed by the Data Coordinating Center of the University of Rochester.
Defining PEW
Using data from the first two annual visits of the study, indicators for PEW were created based upon the International Society of Renal Nutrition and Metabolism diagnostic criteria [1] with modifications and additions to provide greater applicability to children [24]. The criteria for clinical diagnosis of PEW included the following:
-
(1)
Biochemical: TC <100 mg/100 mL; serum albumin <3.8 g/100 mL, which was approximately the 5th percentile of the data; serum transferrin <140 mg/dL [25]; CRP >3 mg/L
-
(2)
Reduced body mass: defined by a BMI for height-age and sex of less than the 5th percentile at entry into CKiD or a decrease in BMI for height-age and sex percentile of ≥10 % between the first and second annual visits from an initial BMI for height-age and sex percentile of <80th
-
(3)
Reduced muscle mass: MUAC for height-age and sex of <5th percentile or a decrease in MUAC for height-age and sex percentile of ≥10 % between the first and second annual visits;
-
(4)
Decreased appetite as a surrogate for dietary protein intake: fair, poor, or very poor appetite reported over the week prior to the study visit.
We also evaluated the improvement in prediction gained with using a pediatric-specific metric:
-
(5)
Poor growth: defined as either short stature (a height for age and sex percentile of <3 % [26]) or poor growth velocity (a decrease in height for age and sex percentile of ≥10 % between the first and second annual visits).
Using combinations of the indicators described above, three definitions of PEW were created: a minimal PEW definition requiring any positive test in ≥2 of categories (1) through (4) to be met; a standard PEW definition requiring any positive test in ≥3 of categories (1) through (4); a modified PEW definition requiring any positive test in ≥3 of categories (1) through (5), such that poor growth was also included as a separate indicator category.
Statistical analysis
To avoid a loss of information on those with incomplete data on some indicators, multiple imputation was used to complete missing laboratory and self-report data of PEW indicators integral to classifying the participants. Missing values were imputed five times based on the distribution of covariates (Tanner stage, BMI percentile, height percentile, serum creatinine, serum transferrin, cystatin C, hemoglobin, bicarbonate, albumin, urine creatinine, urine protein, low-density lipoprotein cholesterol, CRP, appetite score, GFR, MUAC, and low birth weight) using a Markov chain Monte Carlo method [27, 28] and assuming multivariate normality. Non-fasting lipid measurements were also assumed to be missing and imputed. Established methods for combining estimates from each imputed dataset were used to appropriately adjust standard errors [27, 28]. Trends across categories of imputed variables were tested using linear or logistic regression, assuming an ordinal relationship between the independent variable and the categorical dependent variable.
Using longitudinal data on the GFR trajectory of the children following the second annual visit, the annual percentage change in GFR was estimated using a segmented linear mixed effects model with a random intercept and slope. The model estimated the effect on the GFR slope separately for the period from baseline to 2 years and after 2 years to examine both proximate and longer term effects of PEW on CKD progression. In addition to progression of kidney dysfunction, self-reported incident hospitalization events were also examined. Poisson regression was used to assess the association between definitions of PEW (defined at the second annual visit) and the rate of incident hospitalizations within 2 years after the PEW assessment, with each definition assessed in a separate model. Generalized estimating equations were used to account for repeated reports of hospitalization from a single individual [29]. Models were adjusted for age (as continuous), CKD stage (45< = GFR<60, 30< = GFR<45, GFR<30, as indicator variables) glomerular diagnosis, a urine protein to creatinine ratio of >2, anemia (hemoglobin level <5th percentile for age and sex), and low birth weight (birth weight <2,500 g).
Results
There were 528 children who contributed to the analysis. Of these, data were missing on TC laboratory measurements, including non-fasting measurements, from 61 (12 %) children, on albumin measurements from 23 (4 %) children, on serum transferrin from 254 (48 %) children, on CRP from 78 (15 %) children, on BMI for height-age and sex percentile at one or both of the first two annual visits from 67 (13 %) children, on MUAC for height-age and sex percentile at one or both of the first two annual visits from 94 (18 %) children, on appetite information from 43 (8 %) children, and on height for age and sex percentile at one or both of the first two annual visits from 87 (16 %) children. The demographic and disease characteristics of the 528 children are shown in Table 1. The overall cohort had a median age of 12 years and a median GFR of 45 mL/min/1.73 m2; 39 % were female and 18 % were African American.
Using the data augmented through multiple imputation, we compared the characteristics of those who met each definition of PEW with the overall cohort (Table 1). Children meeting the minimal PEW definition represented 20 % [95 % confidence interval (CI) 16, 24] of the cohort. These children were more likely to have a lower median BMI for height-age and sex Z score (P = 0.02), a lower MUAC height-age and sex Z score (P = 0.02), and a higher urine protein to creatinine ratio (P = 0.04). Children meeting the standard PEW definition represented 7 % (95 % CI 5, 10) of the cohort. These children were more likely to have a lower median BMI for height-age and sex Z score (P < 0.001) and a lower MUAC height-age and sex Z score (P < 0.001). Children meeting the modified PEW definition represented 15 % (95 % CI 12, 18) of the cohort. They were more likely to have a lower median weight for age and sex Z score (P = 0.03), a lower BMI for height-age and sex Z score (P = 0.02), a lower MUAC height-age and sex Z score (P = 0.02), and a higher percentage of children with a protein to creatinine ratio of >2 (P = 0.03).
When the prevalence of the various indicators of PEW were examined in the overall cohort and by CKD stage, the data suggested trends towards higher prevalence with lower GFR in hypoalbuminemia (P trend = 0.04), decreased appetite (P trend < 0.001), reduced muscle mass (P trend = 0.20), and reduced body mass (P trend = 0.16), although only hypoalbuminemia and decreased appetite were significant by a linear trend (Fig. 1). Low transferrin and TC levels were virtually non-existent in the cohort. The prevalence of high CRP appeared to increase with increasing GFR category but was not significant (P trend = 0.28). There was no statistically significant increase in the prevalence of PEW with CKD stage regardless of definition (Fig. 2). Notable increases in prevalence of PEW were only seen in patients with a GFR of <30 mL/min and PEW appeared to be stable in earlier stages of CKD. Collapsing the GFR categories to focus on the threshold of 30 mL/min, the odds of having PEW based on a GFR of <30 mL/min versus a GFR of ≥30 mL/min were 1.5 (95 % CI 0.7, 2.8) 1.4 (95 % CI 0.5, 3.5), and 1.5 (95 % CI 0.8, 2.9), respectively, by the minimal, standard, and modified definitions.

The prevalence of indicators of protein-energy wasting (PEW) used to form the three definitions. The prevalence is presented stratified by chronic kidney disease (CKD) stage GFR>=60, 45<=GFR<60, 30<=GFR<45, and GFR<30 ml/min/1.73 m2 and also overall. CRP C-reactive protein

The prevalence of protein-energy wasting (PEW) as classified using the three definitions adopted in this study: minimal PEW, defined as that requiring at least one test in ≥2 of the four original categories; standard PEW, defined as that requiring at least one test in ≥3 of the four original categories; modified PEW, defined as that requiring at least one test in ≥3 of the five categories (4 original plus poor growth). The prevalence is presented stratified by chronic kidney disease (CKD) stage GFR>=60, 45<=GFR<60, 30<=GFR<45, and GFR<30 ml/min/1.73 m2 and also overall
We were primarily interested in longitudinal risk associations with CKD progression and hospitalization to establish whether any of the definitions of PEW were predictive of clinically important endpoints. First we looked at the annual GFR percentage decline to see if meeting the criteria for one or more of the PEW definitions at baseline (the second annual CKiD visit) was associated with faster kidney function decline. GFR decline was assessed in both the first 2 years after PEW assessment and thereafter, which included data up to 7 years after baseline (V2) with an interquartile range (IQR) of 1–4 years of follow-up. From segmented linear mixed effects models broken at 2 years from baseline, the cohort experienced approximately a 3.5 % annual decline in overall GFR level, and there was no evidence that children meeting any of the PEW definitions experienced greater declines (Table 2). The annual percentage decline was approximately 2.7 % per year after 2 years from baseline, suggesting a modest deceleration in decline on average. Again there was no evidence of a difference in the rate of decline among children meeting any of the PEW definitions. Age, CKD stage, urine protein to creatinine ratio of >2, and anemia (hemoglobin level <5th percentile for age and sex) were significantly associated with lower GFR in the multivariate models.
Secondly, we examined the incidence rate of hospitalization during the 2 years following baseline using Poisson regression analysis. The unadjusted estimated incidence rate ratios were 1.9-, 2.1-, and 2.2-fold higher for those children classified as PEW using the minimal, standard, and modified definitions, respectively (P = 0.08, 0.09, and 0.03, respectively). Following adjustment, the estimates became 1.8, 2.1, and 2.0, respectively, with the modified PEW definition maintaining modest significance (P = 0.06). The estimates are compared in Fig. 3. We also examined poor growth as a predictor of hospitalization and found it to be less predictive in adjusted models than the modified PEW definition, of which it was one component (incidence rate ratio 1.8; P = 0.11). In the multivariate models with PEW, only CKD stage was a significant predictor of hospitalization in the adjusted models (P = 0.05 in all models).

The unadjusted and adjusted incidence rate ratios for hospitalization within the 2 years from baseline comparing the three protein-energy wasting (PEW) definitions used in this study
Discussion
There is a dearth of studies examining the occurrence of PEW in children with CKD. Wasting/cachexia syndrome is very common in ESRD in adult populations (30–75 %) and consists of anorexia, increased energy expenditure, decreased protein stores, and loss of weight and muscle mass [30]. While this syndrome in its various forms (PEW vs. cachexia which has been considered a more severe state of PEW) has been described for adults, and diagnostic criteria have been proposed [1, 8], the applicability of these clinical features to children with CKD has not been established. In this study we examined the prevalence of adult diagnostic criteria as well as pediatric focused indicators of PEW in a pediatric CKD cohort and assessed the degree to which varying definitions using these criteria predict incident hospitalizations and CKD progression. We found that the incidence of PEW ranged from 7 to 20 % in the overall cohort depending upon the definition, and an increase in prevalence (corresponding to an odds ratio of 1.5) was suggested in advanced CKD stages 4 and 5, although the increase was not statistically significant. The lack of statistical significance may be the result of relatively small numbers of children meeting any one PEW definition in our cohort. Several of the indicators of PEW tended to increase with decreasing GFR, with hypoalbuminemia and poor appetite having the strongest association. These results may suggest that, of the four laboratory measures assessed, hypoalbuminemia is the most sensitive indicator of PEW in our pediatric cohort. Both low transferrin and cholesterol levels were exceedingly rare. It is possible that low transferrin and cholesterol levels may be more valuable indicators in children with more severe disease or those on dialysis. In contrast to what has been reported in adult studies of CKD, high CRP in the CKiD cohort seemed to be more common in children with milder disease. While PEW is thought to be a process driven by inflammation, a recent report by Foster et al. [11] examining children with more advanced CKD also reported a lack of association between markers of inflammation and wasting based on leg lean mass Z scores, as measured by DEXA scans, except in the most advanced stages of CKD in children. Notably, these authors reported no significant skeletal muscle wasting in children with CKD stages 2–3.
There is no clinical consensus as to the optimal assessment of PEW in children. We used both baseline and longitudinal information to classify participants in terms of their muscle mass, body mass, and growth status. As multiple prior studies have implicated short stature and poor growth as predictors of adverse outcomes in children with CKD, we included an assessment of growth status in our modified definition of PEW. However, the sensitivity of this poor growth measure may be compromised if small but non-wasted children are captured in the definition. Similarly, using decreasing BMI percentiles, may capture overweight children who have intentionally lost body mass. In addition, BMI is an imperfect surrogate of lean mass. BMI can result in questionable measurements of wasting in CKD, which is ideally defined as diminished lean body mass. Fluid overload, which is common in CKD, confounds BMI and lean/skeletal mass measurements [31]. Furthermore, calorie supplementation, which is commonly prescribed in CKD children with a weight deficit or linear growth failure, may not correct true lean mass deficits in CKD and may instead increase body weight by increasing fat mass and water content. Rashid et al. [32] measured body composition by DEXA scan in growth-retarded children with advanced CKD on energy supplementation and showed that a normal BMI can be associated with reduction in lean mass and that reduced BMI can be associated with increased fat mass in these children.
The most important test of a PEW definition is the prediction of clinical outcomes. The modified definition of PEW, which included criteria for poor growth specific to a pediatric context, was the only definition associated with incident hospitalizations within 2 years of classification. This finding suggests that growth may be a better standard for diagnosing PEW in children than weight-based criteria. Adding poor growth to the definition also increased the prevalence of PEW from 7 to 15 %. Indeed, the Society for Cachexia and Wasting Disorders (SCWD), which includes participants with diverse backgrounds encompassing many of the diseases states that result in cachexia (such as cancer, human immunodeficiency virus infection, heart failure, CKD, and chronic obstructive pulmonary disease), identified growth failure as the most important clinical feature of cachexia in children [33].
There are limitations to our analysis that should be noted. The CKiD cohort comprised children with moderate CKD and, therefore, the prevalence of PEW was relatively low, limiting our ability to look at associations with outcomes and discriminate between PEW definitions. In addition, a direct measurement of GFR was not available every year by study design, and thus estimated GFRs were used in intervening years to supplement iohexol GFR measurements. Estimated GFRs from CKiD’s internally derived equation have shown good agreement with iohexol GFR measurements [18]. However, using estimated and directly measured GFR interchangeably could result in bias in estimated GFR decline over time.
In summary, our results suggest that diagnosing PEW syndrome in children with CKD requires pediatric-specific criteria. The addition of an indicator of growth failure or poor growth velocity added to the existing adult criteria improved the prediction of hospitalizations. Clinicians should consider growth in their assessment of children at risk for PEW.
References
Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Trevino-Becerra A, Wanner C (2008) A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int 73:391–398
Kovesdy CP, Kalantar-Zadeh K (2009) Why is protein-energy wasting associated with mortality in chronic kidney disease? Semin Nephrol 29:3–14
Wong CS, Hingorani S, Gillen DL, Sherrard DJ, Watkins SL, Brandt JR, Ball A, Stehman-Breen CO (2002) Hypoalbuminemia and risk of death in pediatric patients with end-stage renal disease. Kidney Int 61:630–637
Menon V, Greene T, Wang X, Pereira AA, Marcovina SM, Beck GJ, Kusek JW, Collins AJ, Levey AS, Sarnak MJ (2005) C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int 68:766–772
Muntner P, He J, Astor BC, Folsom AR, Coresh J (2005) Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: results from the atherosclerosis risk in communities study. J Am Soc Nephrol 16:529–538
Weiner DE, Tighiouart H, Elsayed EF, Griffith JL, Salem DN, Levey AS, Sarnak MJ (2008) The relationship between nontraditional risk factors and outcomes in individuals with stage 3 to 4 CKD. Am J Kidney Dis 51:212–223
Wong CS, Gipson DS, Gillen DL, Emerson S, Koepsell T, Sherrard DJ, Watkins SL, Stehman-Breen C (2000) Anthropometric measures and risk of death in children with end-stage renal disease. Am J Kidney Dis 36:811–819
Evans M, Fryzek JP, Elinder CG, Cohen SS, McLaughlin JK, Nyren O, Fored CM (2005) The natural history of chronic renal failure: results from an unselected, population-based, inception cohort in Sweden. Am J Kidney Dis 46:863–870
Kovesdy CP, Anderson JE, Kalantar-Zadeh K (2007) Paradoxical association between body mass index and mortality in men with CKD not yet on dialysis. Am J Kidney Dis 49:581–591
Kwan BC, Murtaugh MA, Beddhu S (2007) Associations of body size with metabolic syndrome and mortality in moderate chronic kidney disease. Clin J Am Soc Nephrol 2:992–998
Foster BJ, Kalkwarf HJ, Shults J, Zemel BS, Wetzsteon RJ, Thayu M, Foerster DL, Leonard MB (2011) Association of chronic kidney disease with muscle deficits in children. J Am Soc Nephrol 22:377–386
Furth SL, Cole SR, Moxey-Mims M, Kaskel F, Mak R, Schwartz G, Wong C, Muñoz A, Warady BA (2006) Design and methods of the Chronic Kidney Disease in Children (CKiD) prospective cohort study. Clin J Am Soc Nephrol 1:1006–1015
Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A (1976) A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 58:259–263
Schwartz GJ, Gauthier B (1985) A simple estimate of glomerular filtration rate in adolescent boys. J Pediatr 106:522–526
Schwartz GJ, Brion LP, Spitzer A (1987) The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin N Am 34:571–590
Schwartz GJ, Furth S, Cole SR, Warady B, Munoz A (2006) Glomerular filtration rate via plasma iohexol disappearance: pilot study for chronic kidney disease in children. Kidney Int 69:2070–2077
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, Furth SL, Munoz A (2012) Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82:445–453
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
KDOQI Work Group (2009) KDOQI clinical practice guideline for nutrition in children with CKD: 2008 update. Executive summary (2009). Am J Kidney Dis 53:S11–S104
Centers for Disease Control and Prevention (CDC)/ National Center for Health Statistics (NCHS) (2008) National health and nutrition examination survey data. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Hyattsville. Available at: http://www.cdc.gov/nchs/nhanes/nhanes2007-2008/nhanes07_08.htm
Tanner JM (1962) Growth at adolescence. Blackwell Scientific Publication, Oxford
Haycock GB, Schwartz GJ, Wisotsky DH (1978) Geometric method for measuring body surface area: a height–weight formula validated in infants, children, and adults. J Pediatr 93:62–66
Mak RH, Cheung WW, Zhan JY, Shen Q, Foster BJ (2012) Cachexia and protein-energy wasting in children with chronic kidney disease. Pediatr Nephrol 27:173–181
Kalantar-Zadeh K, Kleiner M, Dunne E, Ahern K, Nelson M, Koslowe R, Luft FC (1998) Total iron-binding capacity-estimated transferrin correlates with the nutritional subjective global assessment in hemodialysis patients. Am J Kidney Dis 31:263–272
Furth SL, Abraham AG, Jerry-Fluker J, Schwartz GJ, Benfield M, Kaskel F, Wong C, Mak RH, Moxey-Mims M, Warady BA (2011) Metabolic abnormalities, cardiovascular disease risk factors, and GFR decline in children with chronic kidney disease. Clin J Am Soc Nephrol 6:2132–2140
Little RJA, Rubin DB (2002) Statistical analysis with missing data, 2nd edn. Wiley, New York
Schafer JL (1997) Analysis of incomplete multivariate data. Chapman and Hill, New York
Liang KY, Zeger SL (1986) Longitudinal data analysis using generalized linear models. Biometrika 73:13–22
Mak RH, Ikizler AT, Kovesdy CP, Raj DS, Stenvinkel P, Kalantar-Zadeh K (2011) Wasting in chronic kidney disease. J Cachex Sarcopenia Muscle 2:9–25
Cheung WW, Mak RH (2012) Melanocortin antagonism ameliorates muscle wasting and inflammation in chronic kidney disease. Am J Physiol Ren Physiol 303:F1315–F1324
Rashid R, Neill E, Smith W, King D, Beattie TJ, Murphy A, Ramage IJ, Maxwell H, Ahmed SF (2006) Body composition and nutritional intake in children with chronic kidney disease. Pediatr Nephrol 21:1730–1738
Evans WJ, Morley JE, Argiles J, Bales C, Baracos V, Guttridge D, Jatoi A, Kalantar-Zadeh K, Lochs H, Mantovani G, Marks D, Mitch WE, Muscaritoli M, Najand A, Ponikowski P, Rossi FF, Schambelan M, Schols A, Schuster M, Thomas D, Wolfe R, Anker SD (2008) Cachexia: a new definition. Clin Nutr 27:793–799
Acknowledgments
The authors would like to acknowledge the efforts of Derek Ng and Rachel Zack in the analysis of the data presented in this manuscript. Data in this manuscript were collected by the Chronic Kidney Disease in children prospective cohort study (CKiD) with clinical coordinating centers (Principal Investigators) at Children’s Mercy Hospital and the University of Missouri–Kansas City (Bradley Warady, MD) and Children’s Hospital of Philadelphia (Susan Furth, MD, Ph.D.), data coordinating center at the Johns Hopkins Bloomberg School of Public Health (Alvaro Muñoz, PhD), and the Central Biochemistry Laboratory at the University of Rochester (George J. Schwartz, MD). The CKiD is funded by the National Institute of Diabetes and Digestive and Kidney Diseases, with additional funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Heart, Lung, and Blood Institute (U01 DK82194, U01-DK-66143, U01-DK-66174, and U01-DK-66116). The CKID website is located at http://www.statepi.jhsph.edu/ckid.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abraham, A.G., Mak, R.H., Mitsnefes, M. et al. Protein energy wasting in children with chronic kidney disease. Pediatr Nephrol 29, 1231–1238 (2014). https://doi.org/10.1007/s00467-014-2768-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-014-2768-9