
Abstract
Background
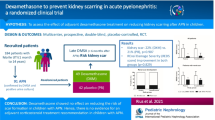
Numerous factors may contribute to renal tissue injury after urinary tract infection. We have evaluated the effects of vitamins A or E supplementation in combination with antibiotics for the prevention of renal scarring in acute pyelonephritis.
Methods
A simple non-blind randomized clinical trial was conducted on 61 children aged 1 month to 10 years between 2004 and 2006. The inclusion criteria were positive urine culture, clinical findings, and 99mTc-dimercaptosuccinic acid (DMSA) scintigraphy-based evidence in favor of acute pyelonephritis. The children were randomized into three treatment groups: 10-day treatment with only antibiotics (control group; n = 25) and 10-day treatment with supplements of vitamin A (n = 17) or vitamin E (n = 18) in addition to antibiotics during the acute phase of infection. The final analysis was performed after excluding male patients. Each patient was evaluated twice by 99mTc-DMSA scintigraphy performed at least 6 months apart. P < 0.05 was considered to be statistically significant.
Results
The analysis included 108 kidney units. The frequency of inflammation at the beginning of therapy was not significantly different in the three groups (63.3 % in vitamin A, 61 % in vitamin E, and 76.2 % in the control group). A worsening of lesions, based on the second 99mTc-DMSA scan, was observed in 42.5, 0, and 23.3 % of the control, vitamin E, and vitamin A patients, respectively (LR = 26.3, P < 0.001).
Conclusion
Vitamins A or E supplements were effective in reducing renal scarring secondary to acute pyelonephritis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Risk factors for renal parenchymal damage in urinary tract infections (UTI) are the presence of vesicoureteral reflux (VUR) [1], obstructive uropathy, the numbers of flares of acute pyelonephritis (APN), and delay in treatment of acute infection. However, a recent multicenter observational study demonstrates that the incidence of renal scars detected by 99mTc-Dimercaptosuccinic acid (DMSA) scintigraphy is about 30 % despite early or late antibiotic therapy [2]. Severe renal scarring has also been reported after the first episode of APN [3]. The pathogenesis of APN is related to bacterial virulence, immune response, tissue factors, apoptosis, and the production of free radicals that lead to fibrosis and renal scarring [4]. Animal models show that the rate of scarring is reduced by the co-administration of antioxidant or anti-inflammatory agents [5–11]. Therefore, we have studied the effect of vitamin A as an anti-inflammatory and vitamin E as an antioxidant on prevention of renal scarring in children with APN.
Subjects and methods
A simple non-blind open-label randomized clinical trial was conducted on 61 children (aged 1 month to 10 years) with APN between September 2004 and October 2006. The inclusion criteria were positive urine culture, positive clinical findings, and evidence of APN on 99mTc-DMSA scans. Children with neurogenic bladder, systemic hypertension, obstructive uropathy, and high grade vesicoureteral (grade 4–5) were excluded from study. The study was conducted in accordance with the guidelines of the declaration of Helsinki and Tokyo for human research. It was also approved by the Institutional Human Experimentation Committee of Tehran University of Medical Sciences. Informed consent was obtained from all parents. The IRCT registration number is IRCT201103256102N1, and a description is available at the following websites: http://www.irct.ir/searchresult.php?id=6102&number=1 and http://apps.who.int/trialsearch/trial.aspx?trialid=IRCT201103256102N1.
The diagnosis of APN was based on the presence of high grade fever (>38.5 °C), with or without vomiting, malaise, loin pain, or tenderness of costovertebral angle, and the absence of other sources for fever on physical examination.
Positive urine culture was defined as the isolation of >105 colony forming units (cfu)/ml of a single bacterium from the midstream urine sample taken from a continent child, the isolation of bacteria (per ml) from a suprapubic urine sample, or the isolation of >1,000 colonies of a single organism from the catheter urine sample.
The radioisotopic renal cortical scan was performed on the second day of hospitalization. Following the injection of 37 MBq of 99mTc-DMSA intravenously, multiple projection images (anterior, posterior, left posterior oblique, and right posterior oblique) were taken 3–4 h later. Any photopenic lesion (unilateral vs. bilateral/small vs. large/single vs. multiple) visible on the posterior view without volume loss was defined as APN. The lesions were classified further as mild (25 %), moderate (25–50 %), or severe (>50 %) based on renal involvement. The second 99mTc-DMSA scan was performed at least 6 months later. The primary outcome was the persistence of the photopenic lesions with or without volume loss on second 99mTc-DMSA scan [12, 13]. The activity of each kidney unit, as shown on the 99mTc-DMSA scan, was recorded separately. The 99mTc-DMSA scans were evaluated by a physician who was completely blinded to the method and the outcome of therapy. The final outcome was categorized into worsening and persistence or improvement of lesions.
All children with a diagnosis of APN were admitted to the nephrology department. Urinalysis and urine culture were sent to the laboratory prior to the initiation of therapy. Blood samples were taken for cell blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (qualitative), and blood culture.
All children received cephalothin or ampicillin (100 mg/kg/day four times daily) and amikacin (15 mg/kg/day three times daily) for 10 days. Treatment method was affected by the antibiogram profile. Based on the file number, children were assigned in parallel and randomized to three groups (n = 20 cases in each group) sequentially. The first group received only antibiotic therapy (control group), and the second and third groups received antibiotics in combination with oral supplements of either vitamin A (1,500 U/kg/day; capsules 50,000 IU; CO.Tolid daru, Iran) or vitamin E (20 IU/day; capsules 100 IU; CO. Daroopakhsh, Iran), respectively, during the acute phase of infection for 10 days. Renal ultrasound and voiding cystouretrogram were performed for all children during hospitalization.
Secondary outcomes were the incidence of acute kidney injury, intolerance to vitamins, and no response to antibiotic therapy. These outcomes were evaluated by daily measurements of urine output, serum creatinine, and blood pressure, by daily clinical observation of the patient’s general condition, measurement of temperature for fever, and by repeating the urine culture after 3 days of treatment.
The follow-up included a monthly urine culture, prophylactic antibiotic treatment (cephalexin at one-third of therapeutic dosage) at nighttime, and a follow-up 99mTc-DMSA scan after a minimum of 6 months.
Due to the small number of male children enrolled in the study and the higher rate of primary scarring among these children, all data pertaining to male children were excluded from the final analysis (Fig. 1).

CONSORT flow diagram for the randomized clinical trial with vitamin A or vitamin E in children with acute pyelonephritis. DMSA 99mTc-Dimercaptosuccinic acid scintigraphy
Sample size was calculated by using Altman nomogram with a power of 80 %. Student’s t test and analysis of variance were used to compare means. Non-parametric tests for several independent samples were used to compare the median. Frequency and relationship were analyzed by chi-square and Pearson correlation tests, respectively. Data were analyzed according to the pre-designated protocol. P < 0.05 was considered to be statistically significant.
Results
As shown in Fig. 1, three children in the vitamin A group and one child in the vitamin E group refused to take vitamins. For the data analysis, these children were therefore considered to have received only the antibiotic therapy and added to the control group. Negative urine cultures and males were excluded from the final analysis. Table 1 shows the basic demographic data and clinical findings at the time of hospitalization. Table 2 depicts the laboratory results at the time of hospitalization for all three groups.
The most frequent complaints were fever (100 %), followed by poor feeding (31 patients, 57.4 %), irritability (21, 39 %), vomiting (20, 37 %), frequency(21, 39 %), dysuria (16, 29.6 %). Additional other symptoms included foul smelling urine (10 patients, 18.5 %), flank pain (10, 18.2 %), diarrhea (8, 15 %), constipation (4, 7.4 %), incontinency (4, 7.4 %), dribbling (3, 5.6 %), secondary enuresis (3, 5.6 %), suprapubic pain (2, 3.7 %), and abdominal pain (2, 3.7 %).
The summary of the 99mTc-DMSA scan evaluations are given in Table 3. The second 99mTc-DMSA scan was performed after a mean period of 7.07 months (range 5–19 months). Of the 11 kidney units in the vitamin A group with no sign of inflammation, three (27.6 %) showed lesion worsening in the second 99mTc-DMSA scan. In the vitamin E group, 14 kidney units showed no signs of inflammation on both the first and second 99mTc-DMSA studies. In the control group, ten kidney units were assessed to be normal in the first study, and five (50 %) showed lesion worsening on the second 99mTc-DMSA scan. In terms of the study outcome, 42.5 % (17 patients) of control patients showed lesion worsening in the photopenic region at least 6 months later. In contrast, of the children who received the antibiotic therapy in combination with vitamin E or A supplements at the time of acute inflammation, 10.6 % (7 patients) showed evidence of worsening lesions in the photopenic region at follow-up (relative risk 4.1, 95 % confidence interval 1.5–9.4, P = 0.001). The condition of the photopenic lesions had not changed in 32.5 % (13 patients) of control patients, 3.8 % (5) of vitamin E-treated patients, and 10 % (3) of vitamin A-treated patients (P = 0.004). None of the kidney units in the vitamin E-treated patients group showed worsening lesions, in comparison to 26.3 % of those of the vitamin A-treated patients (P = 0.003). The number of need to treat (NNT) for vitamin A was 5.1, for vitamin E 2.32, and for both supplements in general 2.5. In terms of the secondary outcomes, no adverse effect was reported during treatment (Table 4).
Discussion
The results of this study show that vitamin E or A supplements were effective in reducing renal scarring secondary to acute pyelonephritis. In contrast, infants who were only treated with antibiotic showed a higher rate of scar formation. The risk factors for developing renal scars after acute pyelonephritis are high grade VUR, voiding dysfunction, and recurrent UTI. In a multicenter study, the early or late administration of antibiotics was shown to have no effect on the prevalence of renal scar formation in children with acute pyelonephritis [2]. Experimental studies have demonstrated that hypoperfusion due to the aggregation of inflammatory cells and subsequent reperfusion induces the production of free radicals, thereby partly explaining tissue damage in acute pyelonephritis [14–16]. One theory which has emerged is that an adjuvant might be needed to prevent renal scar formation at the time of inflammation [6]. The role of vitamins, nonsteroidal anti-inflammatory drugs (NSAIDs), and steroids in reducing renal cortical scar formation after acute pyelonephritis has been studied experimentally [5–11]. An early study showed that at the time of acute infection, there is a depletion of vitamin A and an increase in the rate of renal retinol excretion [17]. In a rat model with UTI, treatment with vitamin A decreases the risk of cortical scar formation [5–7]. Using this rat model, it has also been shown that following the inoculation of bacteria inducing UTI, vitamin A can prevent renal fibrosis formation independent of the treatment routes and times of prescription and that this effect has no correlation with beta carotene level [7, 8]. In their study, Ayazi et al [18]. administered a therapeutic dosage of vitamin A intramuscularly to 25 children aged less than 24 months and found a higher percentage of abnormalities on the repeat 99mTc-DMSA scans of the controls (no vitamin A injection) after 3 months. We found that the duration of 3 months after UTI is not a sufficient time for scar formation and that the repeated 99mTc-DMSA scan should be delayed until least 6 months or longer to evaluate the establishment of the newly formed renal scars.
Our study has two main advantages. First, we prescribed a physiologic dosage of vitamin A orally and, second, the repeat 99mTc-DMSA scan was performed at least 6 months after the first scan. Despite a similarity of renal involvement in the initial renal 99mTc-DMSA scan and a similar frequency of mild to moderate VUR in both groups, the follow-up 99mTc-DMSA study revealed that 23.3 % of patients in vitamin A group had a worsening of lesions compared to 42.5 % in controls.
Bennette et al. reported that vitamin E supplement reduces the degree of kidney inflammation in the rat model of pyelonephritis [6]. Emamghorashi et al. [9] evaluated the effectiveness of gentamicin therapy alone, vitamin (C and E) co-treatment with gentamicin, and vitamin(s) treatment without antibiotic administration in rat models of APN. Their study of renal pathology among these three groups demonstrated mild or no scar formation in the vitamin-treated groups regardless of antibiotic therapy but moderate to severe scar in the antibiotic group. The effect of antioxidants, including allopurinol and vitamin E, has also been evaluated in the rat model of acute pyelonephritis. The pathological results of that study show that the groups treated with antioxidant during the acute phase of inflammation had lower fibrosis, a lower apoptotic index, and lower levels of transforming growth factor-beta [10]. In our study, children who received supplements of vitamin E, despite having higher ESR and leukocytosis, had less renal scarring compared to the vitamin A group and controls.
A study by Haraoka et al. [11] shows that treatment with prednisolone during inflammation prevents renal scar formation in rats with pyelonephritis even if there is a delay initiating antibiotic therapy [11]. The same clinical experience was noted in children with pyelonephritis treated with dexamethasone in the acute phase of inflammation: the levels of urinary interleukin 8 (as a marker of inflammation) and interleukin 6 (as a marker of fibrosis) markedly decreased within 72 h after the injection of dexamethasone compared to those who were only treated with antibiotic [19].
The cumulative rate of renal scar formation after first UTI in females has been reported to be 11.3 % [20]. In that study, persistent photopenic lesion was considered to be a renal parenchymal scar, and the controls had a significantly higher incidence rate (77 %) of scar formation than the vitamin-treated groups. This figure is not compatible with the incidence rate of scar development after acute pyelonephritis observed in our study. This difference between the studies may be explained by following comments: Firstly, about 60–80 % of the children with febrile UTI meet the 99mTc-DMSA scan criteria for the diagnosis of acute pyelonephritis at the beginning of a study and the remaining children have normal DMSA scan results [21–23]. This is in contrast to our study prerequisite of at least one kidney unit having to satisfy the criteria for APN. Second, in many previous studies, the follow-up 99mTc-DMSA scans were taken at longer intervals (2–11 years) in comparison to our method. The incidence of renal parenchymal photopenic changes has been found to fall from 86 to 24 % when the repeat 99mTc-DMSA scan is performed after a longer interval [21]. Orellana et al. studied 269 patients with febrile UTI and assessed the risk of renal scar formation by comparing 99mTc-DMSA scans at 1- and 6- months intervals. These authors found renal parenchymal damage in one-third of children without VUR, in 72 % with VUR, in 60 % at the first episode of UTI, and in 73 % with recurrent UTI [24]. The third explanation for this high rate of renal damage in controls can be the false positive reporting of persistent mild photopenic region at the poles, which can be a limitation of our study.
The low power of the study, the absence of blindness on drug administration, and the simple method of randomization according to the file number are major limitations of our study. The absence of serum vitamin E and A measurements prior to treatment os another limitation. Confirmation of the benefits of vitamin A and E supplements is reducing renal scar formation in acute pyelonephritis needs larger randomized clinical trials.
Conclusion
Vitamins A and E supplements may be effective in reducing renal scar development secondary to acute pyelonephritis, and vitamin E may be more beneficial in the prevention of renal scar formation.
References
Shaikh N, Ewing AL, Bhatnagar S, Hoberman A (2010) Risk of renal scarring in children with a first urinary tract infection: a systematic review. Pediatrics 126:1084–1091
Hewitt IK, Zucchetta P, Rigon L, Maschio F, Molinari PP, Tomasi L, Toffolo A, Pavanello L, Crivellaro C, Bellato S, Montini G (2008) Early treatment of acute pyelonephritis in children fails to reduce renal scarring: data from the Italian Renal Infection Study Trials. Pediatrics 122:486–490
Leroy S, Chalumeau M, Ulinski T, Dubos F, Sergent-Alaoui A, Merzoug V, Ducou-le-Pointe H, Audry G, Gendrel D, Bensman A (2010) Impressive renal damage after acute pyelonephritis in a child. Pediatr Nephrol 25:1365–1368
Jahnukainen T, Chen M, Celsi G (2005) Mechanisms of renal damage owing to infection. Pediatr Nephrol 20:1043–1053
Soylu A, Kavukçu S, Sarioğlu S, Astarcioğlu H, Türkmen M, Büyükgebiz B (2001) The effect of vitamin A on the course of renal ablation nephropathy. Pediatr Nephrol 16:472–476
Bennett RT, Mazzaccaro RJ, Chopra N, Melman A, Franco I (1999) Suppression of renal inflammation with vitamins A and E in ascending pyelonephritis in rats. J Urol 161:1681–1684
Kavuckcu S, Soylu A, Turkmen M, Sarioglu S, Buyukgebiz R, Gure A (1999) The role of vitamin A in preventing renal scarring secondary to pyelonephritis. BJU Int 83:1055–1059
Kavukçu S, Türkmen M, Sevinç N, Soylu A, Derebek E, Büyükgebiz B (1998) Serum vitamin A and beta-carotene concentrations and renal scarring in urinary tract infections. Arch Dis Child 78:271–272
Emamghorashi F, Owji SM, Motamedifar M (2011) Evaluation of effectiveness of vitamin C and E on prevention of renal scar due to pyelonephritis in rat. Adv Urol. doi:10.1155/2011/489496
Sadeghi Z, Kajbafzadeh AM, Tajik P, Monajemzadeh M, Payabvash S, Elmi A (2008) Vitamin E administration at the onset of fever prevents renal scarring in acute pyelonephritis. Pediatr Nephrol 23:1503–1510
Haraoka M, Matsumoto T, Takahashi K, Kubo S, Tanaka M, Kumazawa J (1994) Suppression of renal scarring by prednisolone combined with ciprofloxacin in ascending pyelonephritis in rats. J Urol 151:1078–1080
Rushton HG (1997) The evaluation of acute pyelonephritis and renal scarring with technetium 99m-dimercaptosuccinic acid renal scintigraphy: evolving concepts and future directions. Pediatr Nephrol 11:108–120
Patel K, Charron M, Hoberman A, Brown MI, Rogers KD (1993) Intra-and interobserver variability in interpretation of DMSA scans using a set of standardized criteria. Pediatr Radiol 23:506–509
Roberts JA (1992) Vesicoureteral reflux and pyelonephritis in the monkeys: a review. J Urol 148:1721–1725
Roberts JA, Roth JK Jr, Domingue G, Lewis RW, Kaack B, Baskin G (1982) Immunology of pyelonephritis in the primate model, V. Effect of superoxide dismutase. J Urol 128:1394–1400
Okur H, Köse O, Kula M, Oztürk F, Muhtaroğlu S, Sümerkan B (2003) The role of infection and free oxygen radical damage in reflux nephropathy: an experimental study. J Urol 169:1874–1877
Stephensen CB, Alvarez JO, Kohatsu J, Hardmeier R, Kennedy JI, Gammon RB (1994) Vitamin A is excreted in urine during acute infection. Am J Clin Nutr 60:388–392
Ayazi P, Moshiri SA, Mahyar A, Moradi M (2011) The effect of vitamin A on renal damage following acute pyelonephritis in children. Eur J Pediatr 170:347–350
Sharifian M, Anvaripour N, Karimi A, Fahimzad A, Mohkam M, Dalirani R, Gholikhani F, Rafiee MA (2008) The role of dexamethasone on decreasing urinary cytokines in children with acute pyelonephritis. Pediatr Nephrol 23:1511–1516
Coulthard MG, Lambert HJ, Keir MJ (1997) Occurrence of renal scars in children after their first referral for urinary tract infection. Br Med J 315:918–919
Jakobsson B, Berg U, Svensson L (1994) Renal scarring after acute pyelonephritis. Arch Dis Child 70:111–115
Vernon SJ, Coulthard MG, Lambert HJ, Keir MJ, Matthews JN (1997) New renal scarring in children who at age 3 and 4 years had had normal scans with dimercaptosuccinic acid: follow up study. Br Med J 315:905–908
Montini G, Zucchetta P, Tomasi L, Talenti E, Rigamonti W, Picco G, Ballan A, Zucchini A, Serra L, Canella V, Gheno M, Venturoli A, Ranieri M, Caddia V, Carasi C, Dall’amico R, Hewitt I (2009) Value of Imaging studies after a first febrile urinary tract infection in young children: data from Italian renal infection study 1. Pediatrics 123:e239–e246
Orellana P, Baquedano P, Rangarajan V, Zhao JH, Eng ND, Fettich J, Chaiwatanarat T, Sonmezoglu K, Kumar D, Park YH, Samuel AM, Sixt R, Bhatnagar V, Padhy AK (2004) Relationship between acute pyelonephritis, renal scarring, and vesicoureteral reflux. Results of a coordinated research project. Pediatr Nephrol 19:1122–1126
Hooman N, Sobouti B, Movahed M (2011) The effect of vitamin E or vitamin A on prevention of renal scarring according to DMSA finding in children with acute pyelonephritis (abstract). Pediatr Nephrol 26:1590
Acknowledgments
The study is based on a thesis approved by Tehran University of Medical Sciences (reference no. 2198) during 2004–2006. The abstract of the study was orally presented at the 44th annual scientific meeting of the European Society for Pediatric Nephrology (ESPN) 14–17 September 2011 in Dubrovnik, Croatia [25].
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sobouti, B., Hooman, N. & Movahed, M. The effect of vitamin E or vitamin A on the prevention of renal scarring in children with acute pyelonephritis. Pediatr Nephrol 28, 277–283 (2013). https://doi.org/10.1007/s00467-012-2308-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-012-2308-4