
Abstract
Background
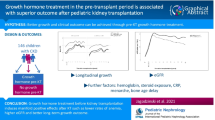
Growth retardation is a considerable clinical problem in children with chronic kidney disease (CKD). Optimization of metabolic and nutritional parameters does not always lead to improved growth. Recombinant human growth hormone (rhGH) treatment has been used to improve height. Several studies in the literature have shown increased growth velocity, although data on the final height (FH) reached are scarce.
Aims
We assessed the effect of rhGH on FH standard deviation score (SDS) in children with CKD following renal transplantation (RTx), comparing it with patients who did not receive rhGH (control group) but were treated with the same protocol and followed up in a single Center.
Methods
Thirty-three patients received rhGH treatment until FH. Fourteen who refused rhGH therapy were included in the controls. Prognostic factors for FH and changes in glomerular filtration rate (GFR) during follow-up were also analyzed
Results
FH SDS in rhGH-treated patients was significantly higher than in controls (−1.88 ± 1.14 vs −3.48 ± 1.19 SDS, respectively, p <0.05). In both groups, a similar reduction in GFR was observed. Height (SDS) at onset of rhGH treatment was the only statistically significant variable useful to predict response to treatment (p = 0.001).
Conclusion
Our findings confirm that rhGH is effective to improve FH in CKD RTx patients, without affecting kidney function.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Growth retardation is a common and significant clinical problem that is not adequately managed in children with chronic kidney disease (CKD). The etiology of growth retardation in these patients is multifactorial. Age at CKD onset, primary kidney disease, tubular defects, metabolic acidosis, kidney osteodystrophy, undernourishment, and impairment of the somatotrophic axis [growth hormone (GH), insulin-like growth factor (IGF), IGF binding proteins] are among the main factors identified to cause growth retardation. Successful renal transplantation (RTx) does not in itself correct growth retardation, especially when RTx is performed after 6 years of age, the graft does not achieve optimal function, and high doses of glucocorticosteroids are administered for immunosuppressive therapy [1]. Recombinant human growth hormone (rhGH) therapy has been used to improve growth velocity and final height in children with CKD [2–5] after RTx [6–9]. Increased growth velocity in post-RTx CKD children on rhGH has been well documented; however, the effect of this treatment on final height (FH) has not been clearly determined.
Haffner et al. [10] reported that long-term rhGH treatment induces persistently improved growth with attainment of target adult height in the majority of patients. Studies from the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) have reported that rhGH treatment is effective in improving growth velocity and final height in pediatric renal allograft recipients [11, 12]. In this study, we assessed the efficacy of rhGH treatment in a group of RTx patients and compared it with the spontaneous growth of a RTx group who were not treated with rhGH but who were followed with the same protocol and in the same center. Our findings show that rhGH treatment prevented further height loss and improved FH standard deviation scores (SDS) without affecting kidney function.
Materials and methods
Thirty-three patients (27 male, six female) aged 13.24 ± 3 years who had undergone RTx because of CKD at Garrahan Pediatric Hospital of Buenos Aires during the last 15 years and who received rhGH treatment for ≥36 months, reaching FH, were included in the study (rhGH group). Inclusion criteria were the following: 18 months post-RTx, stable renal function over the 6 months prior to treatment onset, and growth velocity <25th percentile during the year previous to treatment onset or a height ≤−2 SDS. Exclusion criteria were all patients with kidney rejection within the first 2 years after RTx, cumulative hydrocortisone-equivalent dose therapy >25 mg/m²/day, serum hemoglobin <10 g/dl, serum bicarbonate <22 mEq/l, and serum parathyroid hormone (PTH) >200 pg/ml. All patients received rhGH at a dose of 10 mg/m2 body surface/week, subcutaneously, divided into seven doses until reaching FH. Mean duration of rhGH treatment was 3.53 ± 1 year (range 3.0–5.6 years). Patients were examined at the onset of rhGH treatment and at 3-month intervals thereafter. Evaluation of auxological parameters was carried out every 6 months. After discontinuing rhGH therapy, patients were evaluated every 6 months until FH. At treatment onset, 15 patients were prepubertal, and the remaining 18 were at Tanner’s stage 2–3 of sexual development. Mean ± SDS chronological age was 13.24 ± 3 years, bone age was 8.6 ± 2.6 years, height (H) SDS was −3.28 ± 1.2, and difference between initial height (IH) and target height (TH) was −3.02 ± 1.3 (Table 1). The etiology of CKD was as follows: obstructive uropathy, reflux or renal dysplasia/ hypoplasia (n = 20), hemolytic uremic syndrome (n = 5), hereditary nephropathy (n = 3), and glomerulopathy (n = 5).
Fourteen patients (eight males and six females; eight prepubertal and six pubertal), who had undergone RTx refused rhGH therapy but could be followed until FH (controls). Inclusion and exclusion criteria were the same as in the treatment group. Chronological age, age at RTx, bone age, TH SDS, IH SDS – TH SDS, creatinine clearance (CrCl), and cumulative hydrocortisone equivalent doses (CD) were similar in both groups (Table 1). In controls, etiologies of CKD were also similar: obstructive uropathy, reflux or renal dysplasia/ hypoplasia (n = 7), hemolytic uremic syndrome (n = 1), hereditary nephropathy (n = 3), and glomerulopathy (n = 3). The patients were assessed according to the same protocol as those in the rhGH-treated group.
Anthropometry was performed on wall- and table-mounted stadiometers to determine height and sitting height. SDS and differences (∆) between scores were calculated. Optimization of FH was assessed by comparing it with TH. TH (in cm) was determined according to the following method: [paternal height + (maternal height + 12.5)]/2 for boys, and [(paternal height – 12.5) + maternal height]/2 for girls. Decreasing growth velocity to <1 cm/year, and/or a bone age >16 years in boys and >15 years in girls was considered as evidences of FH . H was expressed as SDS according to chronological age and gender based on Tanner’s criteria for healthy children [13]. Bone age was assessed by the same observer using the Greulich and Pyle method [14]. Glomerular filtration rate (GFR) was calculated with the Schwartz formula based on plasma creatinine concentration [15]. The protocol was approved by the Institutional Review Board of the Hospital de Pediatría Garrahan of Buenos Aires.
Statistical analysis
Statistical analysis was performed using Statistix 7 (Analytical Software, Tallahassee, FI, USA). For comparison of study variables of both groups as a function of time, one-way analysis of variance (ANOVA) was used, and multiple comparisons were performed with the Bonferroni method. Comparisons between treatment and control groups were carried out with Student’s t test for unpaired samples. To determine the best predictor parameter of FH, the best subset regression was used, and multiple regression analysis of different variables was carried out. Values are expressed as mean ± standard deviation (SD). A p ≤ 0.05 α level was considered to be statistically significant.
Results
FH in the rhGH patients was significantly greater than in controls [−1.88 ± 1.14 vs -3.48 ± 1.19 SDS, respectively (p = 0.017)]. In Fig. 1, height at baseline and final height in both groups are shown. Baseline height was below the lower quartile in 77.8% of boys and 100% of girls in the rhGH group and in 75% and 83.3% of boys and girls, respectively, in controls.

Growth curves (height): boys; girls. In red, initial height (IH) and in green final height (FH) for the recombinant human growth hormone (rhGH)-treated group. In black, IH and in blue FH for the control group
However, final height was below the lower quartile in only 37% of boys and 33.3% of girls in the rhGH group but was 87.5% in boys and 100% of girls in controls. In the rhGH group, a significant H SDS gain (∆H SDS: + 1.18 ± 0.7, p = 0.001) was observed, whereas in controls, a significant loss of H SDS (∆H SDS: −0.52 ± 0.22, p = 0.033) was found (Fig. 2).

Evaluation of final height (FH) in the recombinant human growth hormone (rhGH)-treated (gray bars) and control (black bars) groups. a Comparison between initial height (IH) and FH. Height is expressed as X ± standard error (SE) *p= 0.000, **p = 0.017. b Comparison between IH minus target height (TH) and between FH minus TH. *p = 0.001, **p = 0.02
IH–TH SDS was similar in both groups. FH–TH SDS in comparison with IH–TH SDS was significantly less in the rhGH group only (−1.8 ± 1.24 vs. −3.0 ± 1.3, p = 0.001, respectively), whereas in the control group, a tendency to increased difference between IH–TH SDS and FH–TH SDS (−2.41 ± 1 and -2.9 ± 1.5; ns) was observed (Fig. 1). In addition, in the rhGH group, FH–TH SDS was significantly lower than in controls; p = 0.02 (Fig. 2).
A multiple predictor model (Best Subset Regression analysis) of FH was used to identify the best parameters associated with response to rhGH treatment (Table 2). We analyzed the following variables: TH, time spent on dialysis before RTX, duration of rhGH treatment, chronological age at RTx, CrCl, cumulative hydrocortisone equivalent doses, chronological age, and H SDS at the onset of rhGH treatment. H SDS at the onset of rhGH treatment was the best parameter associated with good response to treatment (cp = -0.4, R² = 0.36, p = 0.0001).
At FH, a similar drop in GFR was found in both groups (rhGH from 75.7 ± 17.2 to 67 ± 14.7; controls from 72.6 ± 19.2 to 56.9 ± 9.3 ml/min/m²surface area). In addition, in both groups, similar CrCls were observed during the entire follow-up.
Discussion
Despite advances in the management of children with chronic renal insufficiency (CRI), low stature continues to be a condition that is difficult to manage and that causes significant comorbidity in these patients. Multiple studies have demonstrated the efficacy of rhGH treatment in RTx recipients. However, rhGH is still not used frequently in this pathology, and reports on the impact on FH are scarce. This study shows that rhGH treatment resulted in an increase in FH of 1.18 SDS in these pediatric RTx recipients. Similar results were found in other published series [10, 11, 16]. Haffner et al. [10] described the impact of rhGH treatment for 5 years in a group of CRI patients compared with patients who did not receive the treatment. Although this study concludes that rhGH induces a persistent increase of growth velocity resulting in normal adult height in the majority of patients, the study mixed patients receiving conservative treatment, dialysis, or renal transplantation, making it difficult to assess the effect of rhGH treatment on growth in RTx patients. In the 2005, in a NAPRTCS report, Fine et al. [11] described that rhGH was effective in improving FH in RTx patients. In this study, results of a data base including several centers in the United States were shown. The large size of the series (n = 669) supported the relevance of the results obtained in our study, as our patients were followed up in a single center using the same protocol. In 2009, Seikaly et al. [12] reported an update on this data base and clearly demonstrated the benefits of rhGH in terms of increased growth velocity compared with a nontreated age-matched control group. Nissel et al. [17] described persistently increased growth velocity with rhGH treatment in prepubertal as well as pubertal patients. H SDS gain in RTx recipients was similar to that observed in our patients.
According to our results, the variable that best predicted FH was H at onset of treatment, and a similar finding was reported by Nissel et al. [17]. In contrast with our study, Nissel et al. [16] also observed that rhGH treatment duration was correlated with FH gain. However, Berard et al. [18] and Haffner et al. [10] described additional factors that influence FH, such as duration of treatment and growth velocity previous to treatment onset [18], as well as greater initial height deficit, male gender, longer duration of the prepubertal and pubertal observation periods, and a lower percentage of time spent on dialysis [10]. Again, as in both studies patients receiving conservative treatment, dialysis, and had received RTx were included, it is difficult to specifically analyze growth outcome of RTx recipients only.
According to our results, although different predictive factors of FH have been reported [10, 17, 18], IH was a common determining factor for predicting improved FH. Even though it has been described in an animal model that rhGH through increased IGF-1 production [16] produces renal hyperfiltration followed by glomerulosclerosis and a decreased GFR, our study showed that the long-term use of rhGH in RTx recipients does not affect GFR. Indeed, the fall in GFR was similar in treatment and control groups. Similar findings have been reported in other series [6–10, 14].
Conclusion
In this study, efficacy of rhGH treatment was analyzed in a cohort of RTx recipients followed at a single center with the same protocol. Our findings confirm that rhGH is effective in improving FH in RTx recipients without affecting kidney function. Finally, rhGH treatment proved to be more effective in improving FH when the loss of IH SDS was less marked at onset of treatment. Yearly growth velocity checking is important, as it alerts physicians not to delay initiation of rhGH therapy.
References
Seikaly MG, Salhab N, Gipson D, Yiu V, Stablein D (2006) Stature in children with chronic kidney disease: analysis of NAPRACS database. Pediatr Nephrol 21:793–799
Hokken-Koelega AC, Stijnen T, de Ridder MA, de Muinck Keizer-Schrama SM, Wolff ED, Jong MC, Donckerwolcke RA, Groothoff JW, Blum WF, Drop SL (1994) Growth hormone treatment in growth-retarded adolescents after renal transplant. Lancet 28:343(8909):1313-1317
Hokken-Koelega AC, Stijnen T, De Jong MC, Donckerwolcke RA, De Muinck Keizer-Schrama SM, Blum WF, Drop SL (1994) Double blind trial comparing the effects of two doses of growth hormone in prepubertal patients with chronic renal insufficiency. J Clin Endocrinol Metab 79:1185–1190
Powell DR, Liu F, Baker BK, Hintz RL, Lee PD, Durham SK, Brewer ED, Frane JW, Watkins SL, Hogg RJ (1997) Modulation of growth factors by growth hormone in children with chronic renal failure. The Southwest Pediatric Nephrology Study Group. Kidney Int 51:1970–1979
Hokken-Koelega A, Mulder P, De Jong R, Lilien M, Donckerwolcke R, Groothof J (2000) Long-term effects of growth hormone treatment on growth and puberty in patients with chronic renal insufficiency. Pediatr Nephrol 14:701–706
Hokken-Koelega AC, Stijnen T, de Jong RC, Donckerwolcke RA, Groothoff JW, Wolff ED, Blum WF, de Muinck Keizer-Schrama SM, Drop SL (1996) A placebo-controlled, double-blind trial of growth hormone treatment in prepubertal children after renal transplant. Kidney Int Suppl 53:S128–S134
Guest G, Berard EH, Crosnier H, Chevallier T, Rappaport R, Broyer M (1998) Effects of growth hormone in short children after renal transplantation. French Society of Pediatric Nephrology, Pediatr transplantation. French Society of Pediatric Nephrology. Pediatr Nephrol 12:437–446
Maxwell H, Rees L, British Association for Pediatric Nephrology (1998) Randomized controlled trial of recombinant human growth hormone in prepubertal and pubertal renal transplant recipients. Arch Dis Child 79:481-487
Fine RN, Stablein D, Cohen AH, Tejani A, Kohaut E (2002) Recombinant human growth hormone post-renal transplantation in children: a randomized controlled study of the NAPRTCS. Kidney Int 62:688–696
Haffner D, Schaefer F, Nissel R, Wühl E, Tónshoff B, Mehls O, German Study Group for growth hormone treatment in chronic renal failure (2000) Effect of growth hormone treatment on the adult height of children with chronic renal failure. N Engl J Med 343:923–930
Fine R, Stablein D (2005) Long-term use of recombinant human growth hormone in pediatric allograft recipients: a report of the NAPRTCS Transplant Registry. Pediatr Nephrol 20:404–408
Seikaly M, Waber P , Warady B , Stablein D (2009) The effect of rhGH on height velocity and BMI in children with CKD: a report of the NAPRTCS registry. Pediatr Nephrol 24:1711–1717
Tanner JM, Whitehouse RH, Takaishi M (1966) Standards from birth to maturity for height, weight, height velocity, and weight velocity: British children. Arch Dis Child 219:454–471
Guerlich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press, Stanford, California
Schwartz GJ, Brion LP, Spitzer A (1987) The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am 34:571–590
Kopple JD, Hirschberg R (1990) Physiological effects of growth hormone and insulin-like growth factor I on the kidney. Miner Electrolyte Metab 16:82–88
Nissel R, Lindberg A, Mehls O, Haffner D, Pfizer International Growth Database (KIGS) International Board (2008) Factors predicting the near-final height in growth hormone-treated children and adolescents with chronic kidney disease. J Clin Endocrinol Metab 93:1359–1365
Bérard E , André JL, Guest G , Berthier F,l Afanetti A, Cochat P, Michel Broyer M (2008) On behalf of the French Society for Pediatric Nephrology. Long-term results of rhGH treatment in children with renal failure: experience of the French Society of Pediatric Nephrology. Pediatr Nephrol 23:2031–2038
Acknowledgments
Supported by grants from Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), Fondo para la Investigación Científica y Tecnologica (FONCYT), Argentina
Author information
Authors and Affiliations
Corresponding author
Additional information
Elisa Vaiani and Gabriela Guercio share second authorship of the article
Rights and permissions
About this article
Cite this article
Gil, S., Vaiani, E., Guercio, G. et al. Effectiveness of rhGH treatment on final height of renal-transplant recipients in childhood. Pediatr Nephrol 27, 1005–1009 (2012). https://doi.org/10.1007/s00467-011-2090-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-011-2090-8