
Abstract
To date, two responsible genes for the development of Dent disease have been identified: CLCN5 and OCRL1. In this study, genotype-phenotype correlations were studied in patients with Dent disease and those with Lowe syndrome. Among the 12 boys with a phenotype typical of Dent disease, nine had a mutation in CLCN5 (Dent disease 1), two had a mutation in OCRL1 (Dent disease 2), and one had no mutations in either gene. All seven boys with a clinical diagnosis of Lowe syndrome had a mutation in OCRL1. Patients with Lowe syndrome showed more frequent hypophosphatemia/rickets and more prominent tubular proteinuria than patients with Dent disease 1, and patients with Dent disease 2 had higher degree of tubular proteinuria and hypercalciuria than patients with Dent disease 1. Additionally, one patient with Dent disease 2 showed a mild degree of developmental delay, elevated serum muscle enzyme levels, and cryptorchidism. In this study, the genetic heterogeneity in Dent disease and the phenotypic heterogeneity in Lowe syndrome were confirmed. In patients with Dent disease, the presence of the above-mentioned extrarenal manifestations indicates that it is more likely that the patient is affected by Dent disease 2 than by Dent disease 1.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dent disease is an X-linked proximal tubulopathy with characteristic abnormalities that include low-molecular-weight (LMW) proteinuria, hypercalciuria, and other features of Fanconi syndrome, such as glycosuria, aminoaciduria, and phosphaturia [1–4]. Although some patients may develop nephrocalcinosis, nephrolithiasis, progressive renal failure, and hypophosphatemic rickets, patients with Dent disease typically do not have proximal renal tubular acidosis or extrarenal manifestations [1–4]. During the last decade, loss-of-function mutations of the CLCN5 gene, which is located in Xp11.22 and encodes a renal chloride/proton antiporter (ClC-5), have been reported consistently in patients with Dent disease [5]. However, some patients with clinical features typical of Dent disease do not have mutations of the CLCN5 gene [6, 7]. In 2005, Hoopes et al. [8] confirmed the genetic heterogeneity of Dent disease by detecting OCRL1 mutations in five probands of 13 families who met the strict criteria for Dent disease but lacked mutations in the CLCN5 gene, and these findings have since been confirmed by two other studies [9, 10]. The OCRL1 gene encodes a phosphatidylinositol 4,5 bisphosphate (PIP2) 5-phosphatase located in the trans-Golgi network [11] and is also responsible for the development of oculocerebrorenal syndrome of Lowe (OMIM #309000). Lowe syndrome is a rare X-linked disorder characterized by bilateral congenital cataracts, renal Fanconi syndrome, and mental retardation [12]. Therefore, classic Dent disease caused by mutations of the CLCN5 gene is classified as Dent disease 1 (OMIM #300009), whereas Dent disease caused by mutations of the OCRL1 gene is classified as Dent disease 2 (OMIM #300555).
This study was conducted to confirm genetic heterogeneity in cases of Dent disease and phenotypic heterogeneity in cases of Lowe syndrome. To accomplish this, mutational analyses of the CLCN5 and OCRL1 genes were correlated with genotype–phenotype observations in 12 unrelated boys who had a phenotype typical of Dent disease and seven unrelated boys who were clinically diagnosed with Lowe syndrome, and the results were then compared with those of three similar studies conducted by others [8–10]. In addition, the renal and extrarenal manifestations of patients with Dent disease 1 and Dent disease 2 were compared.
Patients and methods
The medical records of 12 boys who had a phenotype typical of Dent disease and seven boys who had been clinically diagnosed with Lowe syndrome were reviewed. All participants were Korean, and none were related to each other. Criteria for clinical diagnosis of Dent disease were as follows: (1) LMW proteinuria, (2) hypercalciuria, and (3) none of the diagnostic findings of Lowe syndrome listed below. Clinical diagnosis of Lowe syndrome was based on the presence of all three of the following criteria: (1) bilateral congenital cataracts, (2) renal Fanconi syndrome, and (3) mental retardation. The definitions of renal manifestations adopted in this study are listed in Table 1.
CLCN5 gene analysis was conducted as previously described [14]. For genetic analysis of the OCRL1 gene, genomic DNA was isolated from peripheral blood nucleated cells. All 22 exons and flaking introns of the OCRL1 gene were then amplified from the genomic DNA by polymerase chain reactions (PCR) and directly sequenced. It is still unknown whether the 1st, 18th, or 20th methionine (Swiss-Prot entry Q01968) of the OCRL gene is the initiation codon; therefore, in this study, the 18th methionine was chosen as amino acid number 1 in accordance with three similar studies conducted previously [8–10]. Our studies were conducted with approval from the Ethics Committee of the Seoul National University Hospital, Seoul, Korea, and informed consent for the genetic analysis was obtained from all patients or their parents.
Results
Median onset age of the 12 boys with a phenotype typical of Dent disease was 6.4 years (range, 1 month−13 years). The presenting manifestations of patients with Dent disease included urinary abnormalities detected during school screening (six patients), chance proteinuria (five patients), and bowlegs due to rickets (one patient). Five patients had been tentatively diagnosed with glomerular diseases prior to the genetic diagnosis of Dent disease and subsequently underwent renal biopsy, which revealed no glomerular lesions. As shown in Table 2, genetic analysis of the CLCN5 gene revealed seven different mutations in nine patients with Dent disease (Dent disease 1), which included three nonsense mutations (p.W95X, p.E609X, and p.R637X, which was detected in three patients), two missense mutations (p.C101Y and p.S545N), and two 1-base pair insertions (c.444insC resulting in p.L148PfsX172 and c.2141insA resulting in p.T694NfsX741). In addition, two different OCRL1 mutations were detected in two of the three patients who did not have mutations of the CLCN5 gene (Dent disease 2). One of these patients, who had a c.455delA mutation (p.Q152RfsX167) in exon 7 of the OCRL1 gene (patient D10 in Table 2), showed a mild degree of developmental delay and elevated serum creatine kinase and lactate dehydrogenase levels, as well as cryptorchidism, which is a frequent manifestation of Lowe syndrome [12]; however, this patient did not have cataracts or acidosis. The other patient, who had a p.F226S mutation in exon 9 of the OCRL1 gene (patient D11 in Table 2), had no extrarenal manifestations. The remaining patient (patient D12 in Table 2), who had no mutations in either CLCN5 or OCRL1 genes, presented with hypophosphatemic rickets at the age 3.5 years and had borderline acidosis (serum bicarbonate levels that fluctuated between 18 and 24 mmol/L without alkali supplementation) and generalized proximal tubulopathy. However, this patient did not have other features of Lowe syndrome, such as cataracts and mental retardation.
Median age of the seven patients at clinical diagnosis of Lowe syndrome was 8 months (range 2 months–6 years). Three of these patients showed urologic manifestations such as cryptorchidism, dysplastic testes, and inguinal hernia, and one also showed chronic thrombocytopenia. Genetic analysis of the OCRL1 gene revealed six different mutations in seven patients with Lowe syndrome, including two missense mutations (p.S374P and p.Q260E), three nonsense mutations (p.R646X, p.R678X, and p.R805X), and one short deletion (c.2117_2124delTGGATGAA resulting in p.L706WfsX709) (Table 2).
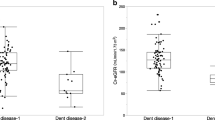
Renal phenotypes of patients with Dent disease and those with Lowe syndrome are compared in Table 3. None of the patients with Dent disease revealed renal functional insufficiency during follow-up periods. There were four affected male adult family members of patients with Dent disease, two of whom were in their 40s, one in his 30s and one in his 60s. All affected family members had normal renal function despite massive tubular proteinuria and hypercalciuria. One patient with Lowe syndrome (patient L6 in Table 2) developed renal insufficiency (serum creatinine 1.4 mg/dL) at the age of 8 months. None of the patients with Lowe syndrome had male adult family members who had clinical features of Lowe syndrome or chronic renal insufficiency. Hypophosphatemia and rickets occurred more frequently, and more prominent LMW proteinuria was observed in patients with Lowe syndrome than in patients with Dent disease 1. In addition, the degree of LMW proteinuria and hypercalciuria observed in patients with Dent disease 2 was comparable with that of patients with Lowe syndrome and higher than that of patients with Dent disease 1. However, statistical analyses were not conducted due to the small number of patients with Dent disease 2 included in this study. For the same reason, the frequency of other renal manifestations in patients with Dent disease 1 and patients with Dent disease 2 were not compared.
Discussion
In this study, we confirmed the genetic heterogeneity of Dent disease and the phenotypic variability of Lowe syndrome. We evaluated 12 patients clinically diagnosed with Dent disease and found that nine had mutations of the CLCN5 gene, two had mutations in the OCRL1 gene, and one had no mutations in either gene. We also found that the incidence of patients with CLCN5 mutations was higher and the incidence of patients with no mutation in either gene was lower than that observed in three similar studies previous conducted [8–10] (Table 4). Although the number patients included in our study was too small for an accurate interpretation to be made, the difference in the results of our study and those of previous studies may have been due, at least in part, to the use of different inclusion criteria for patients with Dent disease. An Italian study adopted three diagnostic criteria of Dent disease, including LMW proteinuria, hypercalciuria, and at least one of the following: nephrocalcinosis, kidney stones, hypophosphatemia, renal failure, aminoaciduria, rickets, or a positive family history [15]. In that study, CLCN5 mutations were detected in 21 of 24 patients (87.5%) who met all three criteria, but only in three of 16 patients (18.8%) who met only two of the three criteria. In addition, all previously conducted studies included some patients who had a phenotype typical of Dent disease but did not have mutations of the CLCN5 and OCRL1 genes, which is similar to the findings of our study. Taken together, these results suggest that there is a third gene responsible for the development of Dent disease.
Although both Dent disease and Lowe syndrome involve similar manifestations of proximal tubular dysfunction, the characteristics of their dysfunctions are not identical. The most striking difference is the absence of renal tubular acidosis in patients with Dent disease, which is one of the cardinal manifestations of Lowe syndrome. Although an extreme degree of LMW proteinuria is consistently found in patients with either disease [2, 16], the other features of proximal tubular dysfunction, such as renal glycosuria, aminoaciduria, and phosphaturia, are detected more frequently in patients with Lowe syndrome than in patients with Dent disease. In our study, patients with Lowe syndrome showed more frequent hypophosphatemia/rickets and more prominent tubular proteinuria than did patients with Dent disease 1, and patients with Dent disease 2 had higher degree of tubular proteinuria and hypercalciuria than did patients with Dent disease 1. Although progressive renal failure is common in both diseases, patients with Dent disease usually develop chronic renal failure in late adulthood, whereas it generally develops between the age 10 and 30 years in patients with Lowe syndrome [2, 12]. Additionally, although hypercalciuria associated with nephrocalcinosis/nephrolithiasis is common in Dent disease, normal levels of urinary calcium excretion have been reported in earlier studies of Lowe syndrome [17]. However, several later studies described a frequent association of hypercalciuria and nephrocalcinosis in patients with Lowe syndrome [18]. Accordingly, in our study, the degree of hypercalciuria and frequency of nephrocalcinosis/nephrolithiasis of patients with Lowe syndrome were comparable with that of patients with Dent disease 1. Take together, our data suggest that proximal tubular dysfunction is more generalized and more severe in patients with Lowe syndrome than in patients with Dent disease 1, whereas patients with Dent disease 2 show intermediate features.
To date, 18 patients from 15 families with Dent disease 2 associated with OCRL1 mutations have been reported, including two patients identified in this study [8–10]. Renal manifestations observed in all of these patients were reportedly virtually identical to those observed in patients with Dent disease 1 who had CLCN5 mutations. However, some patients with Dent disease 2 had extrarenal manifestations, such as mildly elevated serum muscle enzyme levels without overt muscle weakness, cognitive or behavioral impairment, and growth retardation without systemic acidosis, which have not been reported in patients with Dent disease 1. Although the elevation of muscle enzyme levels is also seen in patients with Dent disease 1, it occurs less frequently in those patients [9]. In addition, one of the two patients with Dent disease 2 in our study had cryptorchidism, and two of the seven patients with Lowe syndrome in our study exhibited urogenital anomalies, such as cryptorchidism and dysplastic testes, which are detected in approximately one third of patients diagnosed with Lowe syndrome [12]. From a clinical perspective, the presence of these extrarenal manifestations, including urogenital anomalies, may be useful for differentiation of Dent disease 2 from Dent disease 1. In our study, muscle enzyme levels in the serum (creatine kinase and lactate dehydrogenase) were only checked in one patient with Dent disease 2 and four patients with Lowe syndrome. However the levels were found to be elevated in all tested patients, with the exception of one patient with Lowe syndrome.
In this study, we found nine different mutations of the CLCN5 gene and six different mutations of the OCRL1 gene. Four CLCN5 mutations (p.C101Y, p.S545N, c.444insC, and c.2141insA) and five OCRL1 mutations (p.F226S, c.455delA, p.Q260E, p.S374P, and c.2117_2124del8) identified in this study are novel mutations. Among these novel mutations, two short insertions of the CLCN5 gene and two short deletions of the OCRL1 gene that resulted in frameshifts should be considered pathogenic mutations. Two novel missense mutations of CLCN5 and three novel missense of OCRL1 that involve highly conserved amino acid residues were not detected in 40 male and 40 female Korean control subjects (120 X chromosomes in total). In addition, all these missense mutations were predicted to affect protein function by one or both of the following computer programs: SIFT (http://blocks.fhcrc.org/sift/SIFT.html) and PolyPhen (http://genetics.bwh.harvard.edu/pph/). Taken together, these results indicate that these missense mutations are pathogenic.
Although the correlation of genotype to phenotype in patients with OCRL1 mutations has not been well studied, there have been several presumptive findings reported. To date, 12 different OCRL1 mutations, including two reported in this study, have been identified in association with Dent disease 2, and none of these 12 mutations has been found in association with Lowe syndrome [9]. All OCRL1 mutations, with the exception of gross gene deletions, detected in patients with Lowe syndrome, including seven patients in our study, are located in exons 8–23. In contrast, among the 12 OCRL1 mutations detected in patients with Dent disease 2, all seven frameshift mutations or splice defects leading to a premature stop codon cluster in exons 5–7 of the OCRL1 gene (including the c.455delA mutation in exon 7 in our study) and all five missense mutations (F226S in our study, I257T, R301C, Y462C, and R476W) are located in exons 9–15 of the OCRL1 gene.
The virtually identical renal manifestations that occur in patients with Dent disease 1 and 2 suggest that both ClC-5 and PIP2 5-phosphatase, despite their individual functions, are involved in the same or an overlapping network of cellular function in renal proximal tubular cells [9]. ClC-5 is primarily located in the endosomes of proximal tubular cells, as well as in the thick ascending limb of the loop of Henle and in collecting duct cells [19]. ClC-5 plays important roles in the acidification of the intraendosomal compartments and endosomal recycling, and dysfunctional ClC-5 results in defective membrane sorting and recycling between apical and endosomal compartments in patients with Dent disease and in ClC-5 knockout mice [20, 21]. PIP2 5-phosphatase is expressed ubiquitously in human tissues, including the eyes, kidneys, and brain (the main organs involved in Lowe syndrome), and its subcellular distribution is predominantly in the Golgi complex, lysosomes, and endosomes [11, 22]. Dysfunction of PIP2 5-phosphatase is believed to lead to perturbation of the trans-Golgi network trafficking and dysregulation of the actin dynamics [11, 22]. Therefore, although the pathophysiological mechanisms of Dent disease and Lowe syndrome are not fully understood, both ClC-5 and PIP2 5-phosphatase are expressed in endosomes in the proximal tubular cells and thought to be related to the recycling of multiligand receptors, i.e. megalin and cubilin [23], which may be commonly involved in both diseases [10].
To date, the reason for the restriction of the clinical manifestations of Lowe syndrome to only the kidneys, eyes, and brain have not been elucidated. In addition, it is currently unknown why OCRL1 mutations associated with Dent disease 2 cause only limited renal manifestation despite PIP2 5-phosphatase being expressed in nearly all human tissues [22]. Ocrl1 knockout mice show no evidence of cataracts, neurological abnormalities, or renal dysfunction. However, simultaneous deficiency of both the Ocrl1 and a highly homologous Inpp5b gene, which encodes phosphatidylinositol bisphosphate 5-phosphatase, results in an embryonic lethal phenotype in mice [24–26]. Taken together, these findings suggest that Inpp5b phosphatase can compensate for the absence of the Ocrl1 enzyme in mice. Occurrence of the same or a similar phenomenon in humans, coupled with variability among tissues and individuals in the expression of the compensating enzyme, could explain the phenotypic variability in patients with OCRL1 mutations [8, 26]. In addition, one of our patients with Lowe syndrome had thrombocytopenia. Because the human OCRL protein is 51% homologous with the phosphatidylinositol bisphosphate 5-phosphatase found in human platelets, and because there is functional overlap between these proteins [25], thrombocytopenia may be a clinical manifestation of Lowe syndrome associated with OCRL1 mutations.
In this study, the genetic heterogeneity in Dent disease and the phenotypic heterogeneity in Lowe syndrome were confirmed. Patients with Dent disease should be checked carefully to determine whether they have any extrarenal manifestations, such as mild elevation of muscle enzymes in serum, cognitive or behavioral impairment, growth retardation without systemic acidosis, and urogenital anomalies, such as cryptorchidism and dysplastic testes, because the presence of these symptoms indicates that a diagnosis of Dent disease 2 (OCRL1 mutations) as opposed to Dent disease 1 (CLCN5 mutations) should be considered. The clinical features associated with OCRL1 mutations vary widely between classic Lowe syndrome and typical Dent disease, and there are intermediate syndromes of various degrees. More studies should be conducted to determine whether a third gene exists that is responsible for the development of Dent disease. In addition, the phenotype–genotype correlations in Dent disease and Lowe syndrome still require elucidation.
References
Frymoyer PA, Scheinman SJ, Dunham PB, Jones DB, Hueber P, Schroeder ET (1991) X-linked recessive nephrolithiasis with renal failure. N Engl J Med 325:681–686
Wrong OM, Norden AG, Feest TG (1994) Dent’s disease; a familial proximal renal tubular syndrome with low-molecular-weight proteinuria, hypercalciuria, nephrocalcinosis, metabolic bone disease, progressive renal failure and a marked male predominance. Q J Med 87:473–493
Scheinman SJ (1998) X-linked hypercalciuric nephrolithiasis: clinical syndromes and chloride channel mutations. Kidney Int 53:3–17
Thakker RV (2000) Pathogenesis of Dent’s disease and related syndromes of X-linked nephrolithiasis. Kidney Int 57:787–793
Lloyd SE, Pearce SH, Fisher SE, Steinmeyer K, Schwappach B, Scheinman SJ, Harding B, Bolino A, Devoto M, Goodyer P, Rigden SP, Wrong O, Jentsch TJ, Craig IW, Thakker RV (1996) A common molecular basis for three inherited kidney stone diseases. Nature 379:445–449
Hoopes RR, Raja KM, Koich A, Hueber P, Reid R, Knohl SJ, Scheinman SJ (2004) Evidence for genetic heterogeneity in Dent’s disease. Kidney Int 65:1615–1620
Akuta N, Lloyd SE, Igarashi T, Shiraga H, Matsuyama T, Yokoro S, Cox JP, Thakker RV (1997) Mutations of CLCN5 in Japanese children with idiopathic low molecular weight proteinuria, hypercalciuria and nephrocalcinosis. Kidney Int 52:911–916
Hoopes RR Jr, Shrimpton AE, Knohl SJ, Hueber P, Hoppe B, Matyus J, Simckes A, Tasic V, Toenshoff B, Suchy SF, Nussbaum RL, Scheinman SJ (2005) Dent Disease with mutations in OCRL1. Am J Hum Genet 76:260–267
Utsch B, Bokenkamp A, Benz MR, Besbas N, Dotsch J, Franke I, Frund S, Gok F, Hoppe B, Karle S, Kuwertz-Broking E, Laube G, Neb M, Nuutinen M, Ozaltin F, Rascher W, Ring T, Tasic V, van Wijk JA, Ludwig M (2006) Novel OCRL1 mutations in patients with the phenotype of Dent disease. Am J Kidney Dis 48:942–954
Sekine T, Nozu K, Iyengar R, Fu XJ, Matsuo M, Tanaka R, Iijima K, Matsui E, Harita Y, Inatomi J, Igarashi T (2007) OCRL1 mutations in patients with Dent disease phenotype in Japan. Pediatr Nephrol 22:975–980
Pendaries C, Tronchere H, Plantavid M, Payrastre B (2003) Phosphoinositide signaling disorders in human diseases. FEBS Lett 546:25–31
McSpadden K (2000) Living with Lowe Syndrome: a guide for families, friends and professionals, 3rd edn. Lowe Syndrome Association, Inc
Matos V, van Melle G, Boulat O, Markert M, Bachmann C, Guignard JP (1997) Urinary phosphate/creatinine, calcium/creatinine, and magnesium/creatinine ratios in a healthy pediatric population. J Pediatr 131:252–257
Cheong HI, Lee JW, Zheng SH, Lee JH, Kang JH, Kang HG, Ha IS, Lee SJ, Choi Y (2005) Phenotype and genotype of Dent’s disease in three Korean boys. Pediatr Nephrol 20:455–459
Tosetto E, Ghiggeri GM, Emma F, Barbano G, Carrea A, Vezzoli G, Torregrossa R, Cara M, Ripanti G, Ammenti A, Peruzzi L, Murer L, Ratsch IM, Citron L, Gambaro G, D’Angelo A, Anglani F (2006) Phenotypic and genetic heterogeneity in Dent’s disease - the results of an Italian collaborative study. Nephrol Dial Transplant 21:2452–2463
Laube GF, Russell-Eggitt IM, van’t Hoff WG (2004) Early proximal tubular dysfunction in Lowe’s syndrome. Arch Dis Child 89:479–480
Lowe CU, Terry M, LacLachlan EA (1952) Organic aciduria, decreased renal ammonia production, hydrophthalmos, and mental retardation; clinical entity. Am J Dis Child 83:164–184
Sliman GA, Winters WD, Shaw DW, Avner ED (1995) Hypercalciuria and nephrocalcinosis in the oculocerebrorenal syndrome. J Urol 153:1244–1246
Devuyst O, Christie PT, Courtoy PJ, Beauwens R, Thakker RV (1999) Intra-renal and subcellular distribution of the human chloride channel, ClC-5, reveals a pathophysiological basis for Dent’s disease. Hum Mol Genet 8:247–257
Piwon N, Gunther W, Schwake M, Bosl MR, Jentsch TJ (2000) ClC-5 Cl−channel disruption impairs endocytosis in a mouse model for Dent’s disease. Nature 408:369–373
Wang SS, Devuyst O, Courtoy PJ, Wang XT, Wang H, Wang Y, Thakker RV, Guggino S, Guggino WB (2000) Mice lacking renal chloride channel, CLC-5, are a model for Dent’s disease, a nephrolithiasis disorder associated with defective receptor-mediated endocytosis. Hum Mol Genet 9:2937–2945
Lowe M (2005) Structure and function of the Lowe syndrome protein OCRL1. Traffic 6:711–719
Christensen EI, Devuyst O, Dom G, Nielsen R, Van der Smissen P, Verroust P, Leruth M, Guggino WB, Courtoy PJ (2003) Loss of chloride channel ClC-5 impairs endocytosis by defective trafficking of megalin and cubilin in kidney proximal tubules. Proc Natl Acad Sci USA 100:8472–8477
Attree O, Olivos IM, Okabe I, Bailey LC, Nelson DL, Lewis RA, McInnes RR, Nussbaum RL (1992) The Lowe’s oculocerebrorenal syndrome gene encodes a protein highly homologous to inositol polyphosphate-5-phosphatase. Nature 358:239–242
Zhang X, Jefferson AB, Auethavekiat V, Majerus PW (1995) The protein deficient in Lowe syndrome is a phosphatidylinositol-4,5-bisphosphate 5-phosphatase. Proc Natl Acad Sci USA 92:4853–4856
Janne PA, Suchy SF, Bernard D, MacDonald M, Crawley J, Grinberg A, Wynshaw-Boris A, Westphal H, Nussbaum RL (1998) Functional overlap between murine Inpp5b and Ocrl1 may explain why deficiency of the murine ortholog for OCRL1 does not cause Lowe syndrome in mice. J Clin Invest 101:2042–2253
Acknowledgment
This study was supported by a grant (04-2006-104-0) from Seoul National University Hospital.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cho, H.Y., Lee, B.H., Choi, H.J. et al. Renal manifestations of Dent disease and Lowe syndrome. Pediatr Nephrol 23, 243–249 (2008). https://doi.org/10.1007/s00467-007-0686-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-007-0686-9