
Abstract
The primary causes of renal insufficiency in Albanian children are reflux nephropathy and obstructive uropathies. The poor availability and technical quality of conventional radiological imaging in detecting vesicoureteral reflux (VUR) and lower urinary tract obstruction stimulated this pilot study, with the aim of evaluating the diagnostic efficacy of voiding cystourethrosonography (CUS). The study included 34 patients (aged 0.1–14 years) with acute pyelonephritis, 7 of whom already had renal insufficiency. In 22 patients voiding cystourethrography (VCUG) was also performed and a diagnostic concordance of 66.6% between the two techniques was found. Overall CUS showed a sensitivity superior to VCUG in detecting VUR, partly due to technical problems in performing the fluoroscopic examination. For the same reasons, VCUG missed 1 diagnosis of posterior urethral valves, while CUS correctly identified all 4 patients with this diagnosis. In 34 patients, CUS diagnosed 55 cases of grade II–V VUR and 11 urinary tract malformations; 12 patients underwent surgical intervention, some of them on the basis of CUS only. The follow-up of 31–81 (mean 53) months after CUS was completed by 94% of patients, excluding complications due to missed diagnoses. CUS was demonstrated to be a safe, reliable, and reproducible imaging modality without X-ray hazards that could be useful in developing countries. The potential limiting factors of the technique include the operator’s training and experience and the costs of the contrast medium.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several large studies have proved the excellent sensitivity and specificity of cystosonography (CS) using a contrast medium containing stabilized microbubbles, when compared with voiding cystourethrography (VCUG) and isotopic cystography [1]. The characteristics of CS include its ability to detect vesicoureteral reflux (VUR) without X-ray exposure and its reproducibility without the need for high-quality ultrasonography (US) scanners [2]. The normal and the obstructive patterns of the male urethra during the voiding phase of CS have been recently described, using a transperineal US approach for their visualization [3, 4, 5, 6]. This new dynamic approach has extended the potential use of CS as the primary examination for the detection of VUR to male patients, completing the examination with the visualization of the lower urinary tract during voiding cystourethrosonography (CUS).
In Albania the diagnosis of VUR and obstructive uropathy with conventional imaging modalities (fluoroscopy and nuclear medicine) is either impossible, technically difficult, or unreliable, although some improvements have recently been introduced. In this country, reflux nephropathy and obstructive uropathies, in particular posterior urethral valves (PUV), are the primary causes of renal insufficiency [7]; therefore, a correct and prompt diagnosis is mandatory to provide surgical intervention. Conversely, the conservative medical treatment of VUR is rarely applicable for socio-economic, geographical, and practical reasons. Our experience with CS began in 1995, due to collaboration of our referral center with another Italian center. While waiting for improvements in the VCUG technique, we introduced CS after appropriate training in US, and our first diagnostic results in the detection of VUR with this technique appeared superior to the previous results obtained with fluoroscopic cystourethrography [8]. Finally, at the end of 2000 we were able to apply CUS to the visualization of the lower urinary tract of our patients.
Materials and methods
The pilot study with CS and CUS was performed by an Albanian pediatric nephrologist (R.X.) trained for 2 years in renal US and in contrast-enhanced cystosonographic examination by a pediatric nephrologist experienced in US and in particular CS (M.B.), who was present during all the investigations at the Tirana University Hospital Center.
The study was approved by the Pediatric Department, and written informed consent was obtained from a parent who was always present during the examinations. The procedure was explained to the oldest children to ensure their co-operation. The study included 34 patients (21 males, 13 females) referred to our center for investigation of VUR because of documented pyelonephritis. They were evaluated with contrast medium US according to its availability. Their renal function was documented at admission, and the presence of a urinary tract infection was excluded. All patients were prospectively followed after the diagnosis.
During the period 1995–1999, 22 children (aged 2 months to 14 years, mean 3.9 years) were investigated with CS, while a 12 further children (aged 3 months to 10 years, mean 2.5 years) were examined with CUS in October 2000. All patients were studied in the Pediatric Department at least 1 month after the treatment of pyelonephritis and were under antibiotic prophylaxis. There were 22 patients who also underwent fluoroscopic VCUG in the Radiological Department, on the same day or 2–5 days before or after CS/CUS, using ionic contrast media and an obsolete radiographic apparatus. No information about the results of the two techniques was exchanged between the examiners. The US examinations were performed in the first group of 22 patients with an obsolete US machine (Esaote Au 405) equipped with a 3.5-MHz linear transducer, while for CUS we used an Aloka 5000 portable US machine with a convex 3.5-MHz transducer. The findings were documented using a Sony videoprint 895. Each CS procedure was preceded by a standard accurate US examination of the bladder, kidneys, and the visible urinary tract, with the patient in the prone and supine position; thereafter, CS was performed accordingly to the method described previously [2]. The US contrast medium used for the first 10 examinations was a suspension of galactose (Echovist, Schering) at a concentration of 200 mg/ml, while all other echo-enhanced US examinations were performed using a suspension of 99.9% galactose and 0.1% palmitic acid diluted in sterile water (Levovist, Schering) at a concentration of 300 mg/ml. Through a 4-Fr transurethral catheter, small (0.5–1.0 ml/min) boluses of Echovist or Levovist were administered during the slow and progressive bladder filling with saline, in a quantity sufficient to detect the enhanced ultrasonographic signal in the urinary tract. The amount of Levovist used for the majority of the examinations was 4 ml, and according to the bladder capacity it was equal to 3%–6% of the total bladder content; therefore, an 8-ml vial was enough to study two patients in sequence. During bladder filling and voiding, the ureters and the pelvi-calyceal system were investigated for microbubbles. The international system of radiographic grading of reflux [9] was used to compare CS and VCUG findings according to the literature [1, 2]. During the CS study, a transabdominal suprapubic and a transpubic sagittal US approach was used in male patients to visualize the posterior urethra during micturition. Any dilatation detected in the proximal urethra was considered a possible sign of obstruction. The transperineal sagittal US approach for the visualization of the bladder and urethra was used for CUS in the second group of patients, according to a standardized technique able to distinguish the normal from abnormal male urethral shape during voiding [5, 6]. The residual urinary volume of the bladder was registered in all patients after micturition, and the kidneys were investigated in the prone position along with longitudinal and coronal sections. All possible adverse reactions to the examination were investigated. In addition, the opinion of the oldest children and the parents was sought regarding the procedure. An Italian-Albanian team of pediatric urologists performed the surgical interventions whenever required, based on the fluoroscopic and the US results. The surgery was still performed if the urinary malformations were detected only with US, such as in a case of PUV.
A clinical and US semi-annual follow-up was scheduled for each patient to document the renal growth and morphology, the occurrence of recurrent urinary tract infections and micturating patterns, as well as the compliance of the families. Whenever possible, a dynamic isotopic study of the kidneys with an associated indirect cystoscintigraphy was performed, while a second CUS was scheduled only for patients with PUV and high-grade VUR after their surgical correction.
Results
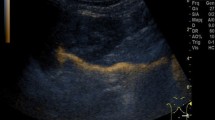
In the group of the 22 patients with 45 kidney-ureter units (KUUs) in whom the comparative study with VCUG was performed, 38 episodes of VUR were detected with one or both examinations (Table 1). VUR was detected in 36 KUUs with CS/CUS and in 29 with VCUG. CS/CUS detected 4 episodes of IV–V grade VUR (2 in 2 duplex kidneys) (Fig. 1) and 5 episodes of II–III grade VUR missed by VCUG. Conversely, 2 cases of grade I–II VUR missed by CS/CUS were detected by VCUG. Apart from the clinically insignificant low-grade VUR, more VUR of severe grade was detected with CS/CUS than with VCUG. Moreover, in the same group of patients, CUS demonstrated 2 cases of PUV and CS indicated 2 further cases, which were confirmed by endoscopy. VCUG diagnosed only 3 cases, because the urethra was not visualized during the voiding phase in an infant incorrectly positioned on the radiological table. The comparitive study demonstrated a concordance in the diagnosis of reflux in 30 of 45 (66.6%) KUUs.

a Renal ultrasonography: duplex kidney with mild pelvic dilatation. b Voiding cystourethrosonography (CUS): contrast medium clearly visible in both refluxing units (UP upper pelvis, LP lower pelvis)
Four patients of this group underwent surgery: in 2 cases PUV were endoscopically resected and 2 cases of severe reflux underwent ureteral reimplantation with remodeling.
Considering all the 34 patients (64% of which were males), CS and CUS diagnosed 55 cases of VUR (grades II–V) in 71 KUUs and 11 urinary tract malformations, comprising 4 PUV, 4 complete renal duplications, 1 paraureteric Hutch diverticulum, 1 solitary and refluxing kidney (Fig. 2), and 1 ureterocele with non-refluxing megaureter. Overall, 42 cases of VUR were of high grade (III–V) (Table 2). Seven patients had renal insufficiency detected for the first time on their admission to the hospital.

High-grade reflux in solitary kidney: a pre-contrast ultrasonography shows a small, dysplastic kidney; b reflux of the contrast medium in the dilated ureter and pelvis during CUS (P pelvis, Ur ureter)
Twelve patients with high-grade VUR, 7 of whom had associated urinary tract malformations, underwent surgical intervention (5 ureteral reimplantations, 1 with ureterocele excision, 1 upper and 2 lower hemi-nephrectomies). Of the patients, 94% completed a semi-annual clinical and US follow-up. Considering the social, economical, and local difficulties of this country, this result was extremely favorable.
Six patients with high-grade VUR and/or PUV had a repeat CUS 12–24 months after the surgical treatment, and 8 patients underwent renal dynamic isotopic studies associated with indirect cystoscintigraphy. Only a case of grade II VUR was detected with CUS in these patients.
In the group of male patients (64% of all patients) the bladder was carefully studied both under basal conditions and during voiding. CS correctly identified PUV in 2 cases, which was confirmed by VCUG and finally resected by endoscopy. In the second group of patients, the transperineal US approach of CUS clearly demonstrated the normal and the obstructive pattern of the male urethra (Fig. 3). Two patients with PUV underwent endoscopy and the US diagnosis was confirmed.

Transperineal approach during the voiding phase of CUS. a Normal male urethra; b posterior urethral valve clearly demonstrated as confirmed by fluoroscopic VCUG (c) (U urethra, B bladder, BN bladder neck, PUV posterior urethral valve)
CS and CUS were well accepted by the parents, and caused little discomfort in the older and more co-operative children. No adverse events related to the intravesical administration of contrast medium were detected during and after these procedures. The mean time for the complete examinations was 30±10 min, during which the echo enhancement with Levovist was always visible, whereas the imaging window of Echovist was very short. The dynamic visualization of the refluxing ureters and pelvicalyceal systems was quite easily performed, while the thermic paper registrations of the images were not always satisfactory due to the poor quality of the apparatus used. Notwithstanding these technical difficulties, a documentation of the presence or absence of VUR was performed in every patient, both in severe and in low-grade VUR.
We calculated that the average cost of each examination, including contrast medium and single-use materials, was 35 Euros, excluding the time (1 h) of the doctor and nurse performing the procedure. This time included obtaining the informed consent, the preparation of the patient, the US evaluation (complete basal and dynamic), and reporting the diagnosis to the parents.
Discussion
Reflux nephropathy and obstructive uropathies are well-known causes of chronic renal insufficiency and terminal renal failure in western countries [10], while in Albania they are the primary causes of renal insufficiency in childhood [7]. With the advent of antenatal and postnatal US diagnosis of congenital urinary tract abnormalities and the prompt identification of infant pyelonephritis, early detection of primary and secondary VUR has been made possible, and patients protected against the potential risk of renal damage progression. In Albania the antenatal US diagnosis of uropathies is currently still exceptional, while pyelonephritic episodes are often recognized late and frequently patients first evaluated in the hospitals have already suffered renal damage or even renal insufficiency.
To exclude urinary malformations in febrile children, fluoroscopic VCUG and sometimes intravenous pyelography are performed. However, the old conventional radiological apparatuses and contrast media, as well as insufficiently developed technical skills for the pediatric age group, expose these unfortunate patients to a significant radiation dose.
The diagnostic accuracy of VUR is also limited, with potentially harmful clinical implications. Surgical treatment is the only therapeutic choice for high-grade VUR in this country, due to the high cost of antibiotics and to the difficulty of performing adequate follow-up of patients under medical prophylaxis. New horizons may be opened by the potential benefits of the endoscopic treatment of VUR, although costs may still represent a limiting factor [11].
In this pilot study, the first to our knowledge performed in a developing country, we assessed the validity of a US-based imaging modality, contrast-enhanced CUS, to detect VUR, comparing its results with the detection and grading of VUR with conventional VCUG. All the investigations were performed under the supervision of a pediatric nephrologist experienced in US (M.B.) in two different periods, using the available obsolete US machines with transducers not always ideal for pediatric use. During the second period, contrast medium US transperineal dynamic urethral imaging was introduced and performed according to the previously described experience [5, 6]. The transperineal US approach enabled us to continue the dynamic visualization of the male urethra during spontaneous micturition, also without contrast medium. In the 2 years after the conclusion of the study, 10 more cases of PUV were diagnosed, and this initial experience has been partially reported elsewhere [12].
The study was performed using two qualitatively different contrast media, i.e., Echovist and Levovist, because in 1995 only the first was available. Although the echo-enhancing characteristics of Levovist were superior to those obtained using Echovist, the diagnostic results of CS with Echovist were considered satisfactory in this study.
Comparison of the results obtained with CS/CUS and those with VCUG in 45 renal units showed a superior sensitivity of CS/CUS in detecting and grading both primary and secondary VUR. Moreover, during US examination the kidney shape, dimension, and morphological ultrasonographic structure were visualized, as well as the associated urinary tract malformations. In the same patients, a functional study of the urinary tract was tentatively performed, observing the urinary peristalsis and the bladder filling and emptying. Surgical correction of VUR and PUV relied more on CS/CUS imaging than on VCUG, since VCUG did not identify 1 case of PUV and few cases of high-grade VUR due to technical reasons, such as the missed registration of the voiding phase of the examination. The low quality of VCUG examinations in some patients made it impossible to consider this fluoroscopic examination as the gold standard in the study of VUR. In our patients, a few cases of grade I–II VUR were detected only with VCUG or with CUS. This is not surprising, since the demonstration of low-grade reflux in the same patient with cyclic voiding cystourethrography [13], cyclic radionuclide cystography [14], and cyclic cystosonography [15] has been variable. The diagnostic efficacy of CUS was validated by the results of the surgical interventions, and by the results of the follow-up completed by almost all the patients, which did not show the presence of complications due to missed diagnosis. The results of this comparative study, and the recent availability of a better radiological apparatus, are improving the diagnostic quality of VCUG.
Echo-enhanced CS/CUS was without any adverse side-effects, was well accepted by all patients and parents, and was performed without costly apparatus, although high-performance US machines would improve the diagnostic ability of this technique [1]. The well-known limiting factor for the routine use of CS/CUS, represented by the costs of the contrast medium, was reduced in our study by using the same vial of Levovist for examining 2 patients in sequence. In the youngest patients, 2–3 ml of Levovist proved to be sufficient to clearly visualize the microbubbles inside the refluxing urinary tract. In patients with a larger bladder capacity, a US contrast medium concentration of about 3% of the bladder content achieved diagnostic results, although the optimal echo-enhancing effect is obtained by 7%–10% contrast medium concentration, according to the literature [1]. Perhaps a cheaper means for echo-enhancement of the US signal in the urinary tract, such as more stable second-generation contrast media [16], will contribute to a further reduction in the costs of CUS. After the preliminary examination, according to the presumed diagnosis, the patients either underwent immediate surgical treatment, performed by an Italian-Albanian team (8 cases), or discharged for a delayed scheduled intervention (4 cases) or for medical follow-up. This clinical approach was considered by us and by the parents, often living away from the referral center, as very efficient and efficacious, and has convinced us to consider CUS as the possible first diagnostic examination for detecting VUR in the Albanian patients.
In conclusion, CUS has good reproducibility, but the quality of the examination depends on the operator’s experience. With rigorous training and strong motivation of dedicated professionals, dynamic urethrosonography without contrast medium and echo-enhanced CUS could be of great benefit for the identification in children with potentially dangerous pathologies (such as severe reflux and/or urethral obstruction), particularly in developing countries. The identification in infancy and in childhood of nephrouropathies that are common causes of hypertension and of end-stage renal diseases, using a relatively inexpensive diagnostic technique, could significantly influence their progression. This is particularly important in countries, such as Albania, where renal replacement therapy is highly expensive and where only a minority of the patients affected can hope to take advantage of it.
References
Darge K (2002) Diagnosis of vesicoureteral reflux with ultrasonography. Pediatr Nephrol 17:52–60
Bosio M (1998) Cystosonography with echocontrast: a new imaging modality to detect vesicoureteric reflux in children. Pediatr Radiol 28:250–255
Bosio M (2000) Visualizzazione dell’uretra posteriore nel maschio durante la fase minzionale della cistosonografia con ecocontrasto. Proceedings SINP Congress, Milan, pp 6–7
Bosio M, Manzoni GA (2001) Voiding cystourethrosonography: a new imaging modality in the study of the lower urinary tract in children. Proceedings of the American Academy of Pediatrics, Section of Urology, San Francisco, California, pp 231–232
Bosio M, Manzoni GA (2002) Detection of posterior urethral valves with voiding cystourethrosonography with echo contrast. J Urol 168:1711–1715
Bosio M (2002) Role of ultrasound in the imaging of posterior urethral valves. Rays 27:135–139
Xhepa R, Cullufi P, Hoxha O, Bushati A, Shehu B (2000) Epidemiologia dell’insufficienza renale cronica nei bambini albanesi: esperienza biennale del centro di riferimento. Proceedings of the SINP Congress, Milan, p 91
Bosio M, Xhepa R (1996) La cistosonografia con ecocontrasto: una promettente tecnica diagnostica per i paesi in via di sviluppo: l’esperienza albanese. Proceedings of the SINP Congress, Cosenza, p 39
Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Moebius TE (1985) International system of radiographic grading of vesicoureteric reflux. Pediatr Radiol 15:105–109
Ardissino G, Daccò V, Testa S, Bonaudo R, Claris-Appiani A, Taioli E, Marra G, Edefonti A, Sereni F (2003) Epidemiology of chronic renal failure in children: data from the Italkid project. Pediatrics 111:e382–e387
Kobelt G, Canning DA, Hensle TW, Lackgren G (2003) The cost-effectiveness of endoscopic injection of dextranomer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol 169:1480–1485
Xhepa R, Hoxha O, Cullufi P, Alushani D, Shehu B, Bosio M (2002) Echographic diagnosis of the male urethral obstruction in children: Albanian experience. Acta Pediatr Esp 60:39
Paltiel HJ, Rupich RC, Kiruluta HG (1992) Enhanced detection of vesico-ureteral reflux in infants and children with use of cyclic voiding cystourethrography. Radiology 184:753–755
Fettich JJ, Kenda RB (1992) Cyclic direct radionuclide voiding cystography: increasing reliability in detecting vesico-ureteral reflux in children. Pediatr Radiol 22:337–338
Novljan G, Kenig A, Rus R, Kenda RB (2003) Cyclic voiding urosonography in detecting vesicoureteral reflux in children. Pediatr Nephrol 18:992–995
Bosio M (2003) Developments in the ultrasound imaging of vesico-ureteral reflux in children. Proceedings of the 8th World Congress of Nephrology, Berlin. p 269
Acknowledgements
This study was presented (in part) at the Congress of the Italian Society of Pediatric Nephrology, Cosenza, 1996, and at the Congress of the Italian Society of Pediatric Urology, Bergamo, 1998.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xhepa, R., Bosio, M. & Manzoni, G. Voiding cystourethrosonography for the diagnosis of vesicoureteral reflux in a developing country. Pediatr Nephrol 19, 638–643 (2004). https://doi.org/10.1007/s00467-004-1439-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-004-1439-7