
Abstract
Background
Research on the utilization of robotic surgical approaches in the management of inflammatory bowel disease (IBD) is limited. The aims of this study were to identify temporal trends in robotic utilization and compare the safety of a robotic to laparoscopic operative approach in patients with IBD.
Methods
Patients who underwent minimally invasive surgery (MIS) for IBD were identified using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database (2013–2021). Temporal trends of robotic utilization were assessed from 2013 to 2021. Primary (30-day overall and serious morbidity) and secondary (unplanned conversion to open) outcomes were assessed between 2019 and 2021, when robotic utilization was highest. Multivariable logistic regression was performed.
Results
The use of a robotic approach for colectomies and proctectomies increased significantly between 2013 and 2021 (p < 0.001), regardless of disease type. A total of 6016 patients underwent MIS for IBD between 2019 and 2021. 2234 (37%) patients had surgery for UC [robotic 430 (19.3%), lap 1804 (80%)] and 3782 (63%) had surgery for CD [robotic 500 (13.2%), lap 3282 (86.8%)]. For patients with UC, there was no difference in rates of overall morbidity (22.6% vs. 20.7%, p = 0.39), serious morbidity (11.4% vs. 12.3%, p = 0.60) or conversion to open (1.5% vs. 2.1%, p = 0.38) between the laparoscopic and robotic approaches, respectively. There was no difference in overall morbidity between the two groups in patients with CD (lap 14.0% vs robotic 16.4%, p = 0.15), however the robotic group exhibited higher rates of serious morbidity (7.3% vs. 11.2%, p < 0.01), shorter LOS (3 vs. 4 days, p < 0.001) and lower rates of conversion to an open procedure (3.8% vs. 1.6%, p = 0.02). Adjusted analysis showed similar results.
Conclusion
The use of the robotic platform in the surgical management of IBD is increasing and is not associated with an increase in 30-day overall morbidity compared to a laparoscopic approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Crohn’s disease (CD) and ulcerative colitis (UC) are chronic conditions characterized by inflammation of the gastrointestinal tract. The global incidence of these diseases, collectively known as inflammatory bowel disease (IBD), has risen dramatically over the last few decades [1, 2]. In the U.S. alone approximately 1.8 to 3.1 million adults are now affected by IBD [3, 4]. Despite a recent stagnation in the increase of incidence rates, the prevalence among older adults in the US continues to increase [3]. In parallel to these changes there has also been an evolution in the treatment paradigm for these conditions. While IBD was historically managed with surgery, the cornerstone of treatment is now medical therapy. New targeted therapeutic strategies, biologic agents, and increased knowledge of clinically relevant targets have improved both the management and outcomes of IBD patients [5]. Despite this, patients with UC and CD may still develop medically refractory or fulminant disease requiring surgical management.
Surgical management of IBD patients is challenging. Due to the chronic nature of the disease, patients are often malnourished, on immunosuppressive therapy at the time of surgery, and have a history of prior abdominal surgeries. There are no current IBD specific credentialing programs for surgeons, but several groups have proposed this type of training, with a focus on minimally invasive surgery (MIS) [6,7,8]. The use of the robotic platform has extended to almost all surgical fields and to increasingly complex patient populations and operations. Potential benefits in the IBD population include the ability to perform a total intracorporeal ileocolic anastomosis, increased exposure during difficult pelvic dissections, and decreased rates of conversion to open in colectomies [6, 9]. However, the increased costs that come from longer average operative times and the robotic console and instruments are a concern.
Prior studies that have focused on the utilization of the robotic platform in IBD patients were limited to single institutional series with small sample sizes [10,11,12,13]. Although these studies have shown that a robotic approach is feasible and safe in select IBD patients, granular data on national utilization of the platform and specific postoperative complications, including rates of conversion to open, anastomotic leak, ileus, and length of stay (LOS) are limited. Therefore, the aims of this study were to utilize a large national database to investigate temporal trends in the utilization of the robotic platform in IBD patients and compare postoperative outcomes between patients who underwent laparoscopic surgery and those who underwent robotic surgery.
Materials and methods
Data source
This was a retrospective analysis using the 2013–2021 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database and its procedure targeted colectomy and proctectomy files. ACS-NSQIP is a nationally validated, risk-adjusted, outcomes-based database that collects more than 150 perioperative variables on patients undergoing surgery from over 700 participating member hospitals of varying sizes and academic affiliations [14, 15]. Certified surgical clinical reviewers prospectively collect data with the purpose of evaluating and improving surgical quality of care. This study was reviewed and approved by the Institutional Review Board of the Johns Hopkins University School of Medicine.
Study population
Patients ≥ 18 years of age diagnosed with IBD (UC or CD) who underwent MIS management were included in this study. IBD diagnoses in patients were identified in NSQIP when IBD related International Classification of Diseases, 9th and 10th revisions (ICD-9/10) codes were listed as both the indication for surgery and the postoperative diagnosis (Supplemental Table 1). Common procedures performed for IBD in the proctectomy and colectomy targeted files were identified using Current Procedural Terminology (CPT) codes (Supplemental Table 2). Patients were excluded if they met any of the following criteria: (a) underwent emergency surgery, (b) CPT codes that included open surgery, rectal prolapse, congenital megacolon or obstruction, (c) American Society of Anesthesiologists (ASA) classification V or missing classification, or (d) non-laparoscopic or non-robotic case (Fig. 1).

Flowchart for selection of patient cohort. NSQIP National surgical quality improvement project, ICD International classification of disease, IBD inflammatory bowel disease, MIS minimally invasive surgery, ASA American Society of Anesthesiologists, CPT current procedural terminology, lap laparoscopic
Baseline characteristics of patients
Demographic characteristics included age, sex (male, female), and race (White, Black, other/unknown). Baseline clinical characteristics included operative stress score [3 (moderate stress) or 4 (high stress)], ASA classification (I–II, III–IV), obesity (defined as BMI ≥ 30), smoking status, history of diabetes, congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), hypertension (HTN), dyspnea, bleeding disorder, and preoperative chronic steroid/immunosuppressive use. Per NSQIP, preoperative chronic steroid/immunosuppressive therapy use is defined as a patient who has “required the regular administration of oral or parenteral corticosteroid medications or immunosuppressant medications, for a chronic medical condition, within the 30 days prior to the principal operative procedure. A one-time pulse limited short course, or a taper of less than 10 days duration would not qualify. Long-interval injections of long-acting agents (e.g., monthly) that are part of an ongoing regimen would qualify” [14, 15]. Operative stress scores were recently developed, and expanded, to quantify physiological stress of surgical procedures on a scale of 1–5 [16, 17]. A score of 1 corresponds to very low stress, 2 low stress, 3 moderate stress, 4 high stress, and 5 very high stress. Operative stress scores were assigned, when possible, based on previously published studies [16, 17]. Since this study only included patients who underwent robotic or laparoscopic surgery and robotic specific CPT codes do not exist, open CPT codes were assigned an adjusted operative stress score based laparoscopic equivalent cases. For example, a CPT code of 44143 corresponds to a “colectomy partial, end colostomy and closure of distal segment” and has an assigned operative stress score of 4. However, the laparoscopic equivalent (CPT 44206) has an operative stress score of 3 (Supplemental Table 2). Operative approach (robotic or laparoscopic) was categorized based on an intention-to-treat approach.
Temporal operative trends
Temporal trends in the utilization of the robotic platform in the surgical management of IBD were investigated by diagnosis (UC or CD) as well as primary procedure type (colectomy or proctectomy). NSQIP Procedure Targeted Colectomy Files were available starting in 2012, however a robotic approach was not reported until 2013, therefore trends in the rates of robotic colectomies were assessed from 2013 to 2021. The NSQIP Procedure Targeted Proctectomy Files were available starting in 2016 and therefore trends in the rates of robotic proctectomies were assessed from 2016 to 2021.
Outcomes
Primary outcomes were assessed from 2019 to 2021 when utilization of the robotic platform was higher to avoid bias from an initial robotic learning curve. The primary outcomes were 30-day postoperative overall and serious morbidity. Overall morbidity was defined as the occurrence of one or more of the following adverse events within 30 days postoperatively: wound infection, pneumonia, urinary tract infection (UTI), venous thromboembolism (VTE), cardiac complication, shock/sepsis, unplanned intubation, bleeding requiring transfusion, renal complication, on ventilator > 48 h, organ/space surgical site infection (SSI), and anastomotic leak. Serious morbidity was defined by the presence of Clavien–Dindo class III–IV complication (cardiac or renal complications, shock/sepsis, unplanned intubation, on ventilator > 48 h, organ/space SSI, or re-operation) [18]. Secondary outcomes included unplanned conversion to open, 30-day postoperative ileus, readmission, reoperation, mortality, operative time, and LOS.
Statistical analysis
Changes in utilization over time were assessed using the Cochran–Armitage test for trend. Baseline characteristics and postoperative outcomes were compared between the laparoscopic and robotic surgery groups for UC and CD patients separately. A Pearson’s Chi-squared test or Fisher’s exact test (when appropriate) was used for categorical variables, and Wilcoxon rank-sum (Mann–Whitney) test or quantile regression (when appropriate) was used for continuous variables. Multivariable logistic regression analysis was used to identify factors associated with 30-day postoperative overall morbidity, serious morbidity, and unplanned conversion to open procedure while adjusting for clinically relevant covariates listed in Table 1. Hosmer–Lemeshow goodness-of-fit test was used to evaluate the models. Statistical significance was indicated by p < 0.05. All statistical analyses were performed using Stata, version 17.0 (StataCorp, College Station, Texas, USA).
Results
Study population
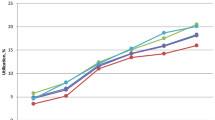
A total of 14,636 patients were identified who underwent MIS for IBD between the years of 2013–2021, with 5572 (38.1%) undergoing surgery for UC and 9064 (61.9%) for CD. An increasing proportion of proctectomies were performed robotically in both patients with UC (17.7% in 2016 to 41.0% in 2021) and CD (14.3% to 35.8%) (p < 0.001) (Fig. 2). The proportion of robotic colectomies also increased in both UC (1.7% in 2013 to 12.4% 2021) and CD patients (2.4% to 12.2%) (p < 0.001) (Fig. 3).

Trends over time of minimally invasive proctectomies for ulcerative colitis and Crohn’s disease. IBD inflammatory bowel disease, UC ulcerative colitis, CD Crohn’s disease

Trends over time of minimally invasive colectomies for ulcerative colitis and Crohn’s disease. IBD inflammatory bowel disease, UC ulcerative colitis, CD Crohn’s disease
Between the years of 2019–2021, 6016 patients had MIS for IBD. Of these patients, 3782 (62.9%) underwent surgery for CD with 3282 (86.8%) undergoing a laparoscopic procedure and 500 (13.2%) a robotic procedure. 2234 (37.1%) patients underwent surgery for UC, with 1804 (81.0%) undergoing a laparoscopic procedure and 430 (19.2%) a robotic procedure (Fig. 1). Among patients who underwent surgery for UC there was no difference in age, race, ASA classification, or preoperative comorbidities such as smoking history, diabetes, CHF, COPD, HTN, dyspnea, or presence of a bleeding disorder between the robotic and laparoscopic groups. Patients who underwent robotic surgery for UC were more frequently male (60.7% robotic vs 54.3% laparoscopic, p = 0.017), had a higher operative stress score (score 4: 67.0% vs 23.6%, p < 0.001), and less frequently used immunosuppressants preoperatively (37.4% vs 62.8%, p < 0.001) (Table 1). Among patients who underwent surgery for CD there was no difference in age, sex, ASA classification, preoperative steroid/immunosuppressant use, or preoperative comorbidities except bleeding disorder (0.2% robotic vs. 1.4% lap, p = 0.024) between the MIS approaches. Patients who had a robotic surgery tended to have a lower operative stress score (score 3: 87.4% vs. 97.1%, p < 0.001) (Table 1).
Most common procedures
The most common laparoscopic procedure performed in patients with UC was a total abdominal colectomy (TAC) without proctectomy (1103, 61.1%), followed by proctectomy with IPAA (ileal pouch-anal anastomosis) (170, 9.4%), and TAC with proctectomy (163, 9.0%). For robotic procedures a proctectomy with IPAA (117, 27.2%) was the most common, followed by TAC with proctectomy and ileal reservoir creation (102, 23.7%), and TAC without proctectomy (69, 16.1%).
The most common laparoscopic procedure performed in patients with CD was a partial colectomy with removal of terminal ileum and ileocolostomy (2241, 68.3%), followed by a partial surgical colectomy with anastomosis (351, 10.7%), and a TAC without proctectomy with ileostomy/ileoproctostomy (243, 7.4%). For robotic procedures, a partial colectomy with removal of terminal ileum and ileocolostomy (272, 54.4%) was the most common, followed by a partial surgical colectomy with anastomosis (70, 14.0%) and a proctectomy combined abdominoperineal with colostomy (55, 11.0%).
Unadjusted outcomes for UC patients
On unadjusted analysis, there was no difference in 30-day overall and serious morbidity, or an unplanned conversion to open procedure between UC patients who underwent a laparoscopic surgery and those who underwent a robotic surgery (overall morbidity: 22.6% vs. 20.7%, p = 0.390; serious morbidity: 11.4% vs. 12.3%, p = 0.598; conversion: 1.5% vs. 2.1%, p = 0.377; respectively) (Table 2). Differences in specific 30-day perioperative outcomes, however, were observed. Laparoscopic patients had higher VTE rates (3.8% vs. 1.9%, p = 0.045) and higher rates of bleeding requiring transfusion (8.7% vs. 4.7%, p = 0.005). There were no significant differences in rates of anastomotic leak (1.8% vs. 3.3%, p = 0.414) or organ/space SSI (6.5% vs. 8.4%, p = 0.178) (Table 2).
In terms of intraoperative outcomes, patients who underwent robotic surgery had longer operative times than patients who underwent laparoscopic surgery (median operative time 297 vs. 210 min, p < 0.001). Readmission rates were higher in the robotic group (19.8% vs. 14.1%, p = 0.003). The top three reasons for readmission were the same in both groups. These included ileus/small bowel obstruction (lap 27.3% vs. robotic 27.1%), followed by infection (lap 27.3% vs. robotic 21.2%), and failure to thrive/dehydration (lap 9.1% vs. robotic 16.5%). There was a higher proportion of patients in the laparoscopic group who were admitted for pain compared to the robotic group (8.7% vs. 4.7%). Expanded details on reasons for readmission can be found in Supplemental Table 3. There was also no difference in rates of reoperation, mortality, or LOS between the two operative approaches (Table 2).
Unadjusted outcomes for CD patients
On unadjusted analysis, there was no difference in 30-day overall morbidity between CD patients who underwent laparoscopic surgery and CD patients who underwent robotic surgery (overall morbidity: 14.0% vs. 16.4%, p = 0.151) (Table 3). The robotic group had a higher rate of serious morbidity (11.2% vs. 7.3%, p = 0.002) and a lower rate of an unplanned conversion to open procedure (3.7% vs 1.6%, p = 0.017). Differences in specific 30-day perioperative outcomes were observed. Robotic patients had higher organ/space SSI rates (8.0% vs. 4.4%, p < 0.001), higher rates of UTI (1.8% vs. 0.73%, p = 0.033), and higher rates of shock/sepsis (4.2% vs. 2.4%, p = 0.017). There were no significant differences in rates of anastomotic leak (2.4% vs. 2.2%, p = 0.850).
In terms of intraoperative outcomes, patients who underwent robotic surgery had longer operative times than patients who underwent laparoscopic surgery (median operative time 228 vs. 152 min, p < 0.001). Patients who underwent robotic surgery also had a significantly shorter LOS than the laparoscopic group [median 3 vs. 4 days, p < 0.001]. There was no difference in rates of 30-day readmission, reoperation, or mortality between the groups.
Adjusted analysis for UC patients
On multivariable logistic regression analysis, no differences in the odds of 30-day overall morbidity (OR 0.93, 95% CI 0.67–1.30, p = 0.680), serious morbidity (OR 1.28, 95% CI 0.85–1.91, p = 0.231), or conversion to open (OR 0.83, 95% CI 0.29–2.41, p = 0.731) were observed between the UC laparoscopic and robotic groups (Table 4).
Factors associated with increased odds of overall morbidity included ASA class III/IV (OR 1.50, 95% CI 1.18–1.92, p = 0.001) and steroid/immunosuppressive therapy use (OR 1.48, 95% CI 1.13–1.94, p = 0.004) (Supplemental Table 4). Factors associated with increased odds of serious morbidity included Black race (OR 2.76, 95% CI 1.57–4.84, p < 0.001), ASA class III/IV (OR 1.40, 95% CI 1.03–1.92, p = 0.033), and steroid/immunosuppressive therapy use (OR 1.53, 95% CI 1.07–2.17, p = 0.018) (Supplemental Table 4). Factors associated with increased conversion to open included BMI ≥ 30 (OR 2.41, 95% CI 11.04–5.58, p = 0.040) (Supplemental Table 4).
Adjusted analysis for CD patients
On multivariable logistic regression analysis, no difference in the odds of 30-day overall morbidity (OR 1.31, 95% CI 0.98–1.78, p = 0.072) was observed between the CD laparoscopic and robotic group (Table 4). However, patients who underwent robotic resections had higher odds of serious morbidity (OR 1.51, 95% CI 1.04–2.18, p = 0.029) and lower odds of conversion to open procedure (OR 0.39, 95% CI 0.17–0.90, p = 0.027) than the laparoscopic group (Table 4).
Factors associated with increased odds of overall morbidity include Other/Unknown race (OR 1.35, 95% CI 1.01–1.79, p = 0.042), ASA class III/IV (OR 1.38, 95% CI 1.11–1.72, p = 0.004), smoking history (OR 1.33, 95% CI 1.02–1.74, 0.034), history of HTN (OR 1.70, 95% CI 1.25–2.31, p = 0.001), and history of bleeding disorder (OR 3.84, 95% CI 1.87–7.90, p < 0.001) (Supplemental Table 5). Factors associated with increased odds of serious morbidity included ASA class III/IV (OR 1.77, 95% CI 1.33–2.36, p < 0.001) and smoking history (OR 1.51, 95% CI 1.08–2.10, p = 0.016). Factors associated with decreased odds of serious morbidity included age < 35 (OR 0.64, 95% CI 0.42–0.96, p = 0.033) (Supplemental Table 5). Other factors associated with increased conversion to open included age > 65 (OR 2.36, 95% CI 1.17–4.75, p = 0.016) and Black race (OR 2.00, 95% CI 1.07–3.72, p = 0.028) (Supplemental Table 5).
Discussion
Advances in medical therapy have led to significant improvements in the overall outcomes and quality of life for patients with IBD. Innovations over the last decade in surgical techniques, particularly the development and use of the robotic platform, have led to increased research on the potential risks and benefits of this approach over more conventional laparoscopic techniques. To our knowledge, this is the first study to investigate national trends in robotic utilization in IBD patients and the largest report on postoperative outcomes in these patients. Our findings highlight the following: (1) the use of the robotic platform in patients with IBD has increased dramatically over the last decade, (2) for patients with UC, the robotic approach is safe and feasible for a variety of procedures, (3) for patients with CD, the utilization of the robot is associated with comparable rates of overall morbidity yet higher rates of serious morbidity, shorter LOS and lower rates of unplanned conversion to open when compared to the laparoscopic approach, and (4) ongoing discussions are needed to accurately identify patients who may benefit from a robotic surgery approach.
Prior studies have shown that the proportion of laparoscopic resections in IBD has increased over time but national trends in robotic utilization have not been previously reported [19]. From 2013 to 2021 the rates of robotic colectomies and proctectomies for both CD and UC increased significantly. Reasons for this may be related to the increased availability of robotic consoles and/or a greater number of surgeons who feel comfortable or prefer to utilize this approach in their practice. Other contributing factors may be a shorter learning curve compared to laparoscopic surgery, particularly in complex diseases such as IBD, and the advantage of improved pelvic exposure in difficult cases [6]. These potential benefits must be weighed with the increased cost of robotic surgery. Although our study found that CD patients who underwent robotic surgery had a shorter LOS, the robotic platform is associated with a higher overall cost of surgery and increased utilization of operative time and thus personnel. Some reports have estimated the cost of robotic surgery is nearly 1.3–2.5 times higher than that of laparoscopic surgery [20, 21]. However, as newer platforms become available, and costs continue to decrease the authors believe utilization with continue to expand and there will continue to be improvement in outcomes.
As minimally invasive surgery, and more specifically robotic surgery, has become more widespread so has research comparing different operative approaches in colorectal procedures. Prior research focused on comparing outcomes between robotic, laparoscopic, and open approaches has been limited by the number of patients with IBD included in the analyses [12]. More focused comparisons between a robotic and laparoscopic approach in IBD are limited to institutional studies, two of which found no difference in outcomes between robotic and laparoscopic proctectomies [10, 11]. A systematic review and meta-analysis reported on five studies which compared robotic versus laparoscopic ileal pouch anal anastomosis (IPAA) and showed that in a pooled analysis there was a non-statistically significant trend toward less complications in robotic procedures [22]. Our study greatly expands the number of robotic surgery cases performed for IBD reported in the literature, and although we found no significant difference between the groups in UC patients, differences in CD patients were evident.
The surgical management of patients with CD is difficult. Numerous studies and editorials have drawn attention to specific challenges in the care of these patients and the need for highly specialized surgeons [6, 8, 23]. Intraoperative factors including friability of tissues and re-operative fields make the surgery complex, and knowledge of technical maneuvers specific to this disease are crucial to provide optimal care. Our study highlights a few potential benefits of a robotic approach, namely a decreased overall LOS and rates of unplanned conversion to open. The decreased rate of conversion is particularly important as many patients with CD are likely to require multiple surgical procedures throughout their lifetime. Conversely, we found that the robotic group had a higher rate of serious morbidity related to increased rates of postoperative organ/space SSI and shock/sepsis. Specifically, this increase appears to be driven by outcomes of patients who underwent robotic proctectomies in the year 2021. Serious morbidity rates increased from 12.1% in 2019 and 17.1% in 2020 to 37.5% in 2021. A similar trend was found among patients who underwent a laparoscopic proctectomy for CD with increases from 11.5% in serious morbidity in 2019 to 20.9% in 2021. Possible reasons for the increase in serious morbidity among robotic compared to the laparoscopic proctectomies could be the lack of haptic feedback in robotic surgery and inability to identify tissues that might be weakened by infection, inflammation, or abscess formation. Reasons for the drastic increase in serious morbidity for both groups in the year 2021 could be related to the COVID-19 pandemic. Patients during this period may have had their surgeries delayed as elective surgeries were canceled at many institutions during this time. It is important to note that despite the increase in serious morbidity among patients with CD who underwent a robotic resection this did not lead to an increased rate of readmission or reoperation. This can be an area of future study as more years of NSQIP data become available.
This present study is not without limitations. ACS-NSQIP is a national, standardized, multi-institutional database that focuses on measuring surgical quality of care but does not include hospital-specific variables. Thus, the authors cannot comment on which centers are performing MIS for patients with IBD and more specifically which centers are utilizing the robot. The dataset does not collect granular data beyond 30 days and as a result, the impact of morbidity and other complications on overall disease course is limited. Additionally, there is no ability to investigate if patients had multiple surgeries throughout the study cohort. The authors chose to analyze postoperative outcomes in patients from 2019 to 2021 when robotic utilization was highest, however the impact of the COVID-19 pandemic on these results is unknown. Finally, we analyzed the robotic and laparoscopic patients using an “intention-to-treat” approach for a more conservative analysis.
Limited research exists surrounding the risk and benefits of the robotic platform in complex patient populations. This study is the first to show an increase in the national utilization of the robot in the surgical management of IBD and presents the largest report on postoperative outcomes in patients undergoing robotic surgery for IBD. We found that in general patients can undergo robotic surgery with acceptable rates of morbidity compared to the laparoscopic approach. Further research to confirm the suggested benefits of the robotic approach in CD on rates of conversion to open and overall LOS is needed. Results from this study can ultimately be used to more accurately counsel patients who are undergoing MIS for IBD on expected outcomes. This can allow for a more precise, thorough, and patient centered discussion surrounding postoperative expectations. Lastly, the study adds to the growing body of literature reporting on the safety of a robotic approach in this unique patient population.
References
Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, Panaccione R, Ghosh S, Wu JCY, Chan FKL, Sung JJY, Kaplan GG (2017) Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet Lond Engl 390:2769–2778
Windsor JW, Kaplan GG (2019) Evolving epidemiology of IBD. Curr Gastroenterol Rep 21:40
Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB (2016) Prevalence of inflammatory bowel disease among adults aged ≥18 years—United States, 2015. MMWR Morb Mortal Wkly Rep 65:1166–1169
GBD 2017 Inflammatory Bowel Disease Collaborators (2020) The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 5:17–30
Turner D, Ricciuto A, Lewis A, D’Amico F, Dhaliwal J, Griffiths AM, Bettenworth D, Sandborn WJ, Sands BE, Reinisch W, Schölmerich J, Bemelman W, Danese S, Mary JY, Rubin D, Colombel J-F, Peyrin-Biroulet L, Dotan I, Abreu MT, Dignass A, International Organization for the Study of IBD (2021) STRIDE-II: an update on the selecting therapeutic targets in inflammatory bowel disease (STRIDE) initiative of the international organization for the study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology 160:1570–1583
Kotze PG, Holubar SD, Lipman JM, Spinelli A (2021) Training for minimally invasive surgery for IBD: a current need. Clin Colon Rectal Surg 34:172–180
Crippa J, Carvello M, Kotze PG, Spinelli A (2021) Robotic surgery in inflammatory bowel disease. Curr Drug Targets 22:112–116
Hansraj N, Kavic SM (2015) Surgery for Crohn’s disease: an emerging surgical specialty. Inflamm Bowel Dis 21:E28-29
Abd El Aziz MA, Grass F, Behm KT, D’Angelo A-L, Mathis KL, Dozois EJ, Larson DW (2022) Trends and consequences of surgical conversion in the United States. Surg Endosc 36:82–90
Miller AT, Berian JR, Rubin M, Hurst RD, Fichera A, Umanskiy K (2012) Robotic-assisted proctectomy for inflammatory bowel disease: a case-matched comparison of laparoscopic and robotic technique. J Gastrointest Surg 16:587–594
Rencuzogullari A, Gorgun E, Costedio M, Aytac E, Kessler H, Abbas MA, Remzi FH (2016) Case-matched comparison of robotic versus laparoscopic proctectomy for inflammatory bowel disease. Surg Laparosc Endosc Percutan Tech 26:e37-40
Huerta S, Meier J, Emuakhagbon V-S, Favela J, Argo M, Polanco PM, Augustine MM, Pham T (2021) A comparative analysis of outcomes of open, laparoscopic, and robotic elective (procto-) colectomies for benign and malignant disease. J Robot Surg 15:53–62
Flynn J, Larach JT, Kong JCH, Waters PS, Warrier SK, Heriot A (2021) The learning curve in robotic colorectal surgery compared with laparoscopic colorectal surgery: a systematic review. Colorectal Dis Off J Assoc Coloproctol G B Irel 23:2806–2820
American College of Surgeons (ACS) (n.d.) ACS NSQIP participant use data file. https://www.facs.org/quality-programs/data-and-registries/acs-nsqip/participant-use-data-file/. Accessed 13 Jan 2023
American College of Surgeons (ACS) (n.d.) About ACS NSQIP. https://www.facs.org/quality-programs/data-and-registries/acs-nsqip/about-acs-nsqip/. Accessed 13 Jan 2023
Shinall MC, Arya S, Youk A, Varley P, Shah R, Massarweh NN, Shireman PK, Johanning JM, Brown AJ, Christie NA, Crist L, Curtin CM, Drolet BC, Dhupar R, Griffin J, Ibinson JW, Johnson JT, Kinney S, LaGrange C, Langerman A, Loyd GE, Mady LJ, Mott MP, Patri M, Siebler JC, Stimson CJ, Thorell WE, Vincent SA, Hall DE (2020) Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg 155:e194620
Yan Q, Kim J, Hall DE, Shinall MC Jr, Reitz KM, Stitzenberg KB, Kao LS, George EL, Youk A, Wang CP, Silverstein JC, Bernstam EV, Shireman PK (2023) Association of frailty and the expanded operative stress score with preoperative acute serious conditions, complications, and mortality in males compared to females: a retrospective observational study. Ann Surg 277(2):e294–e304
Dindo D, Demartines N, Clavien P-A (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Gaglani T, Davis CH, Bailey HR, Cusick MV (2019) Trends and outcomes for minimally invasive surgery for inflammatory bowel disease. J Surg Res 235:303–307
Ramji KM, Cleghorn MC, Josse JM, MacNeill A, O’Brien C, Urbach D, Quereshy FA (2016) Comparison of clinical and economic outcomes between robotic, laparoscopic, and open rectal cancer surgery: early experience at a tertiary care center. Surg Endosc 30:1337–1343
Baek S-J, Kim S-H, Cho J-S, Shin J-W, Kim J (2012) Robotic versus conventional laparoscopic surgery for rectal cancer: a cost analysis from a single institute in Korea. World J Surg 36:2722–2729
Flynn J, Larach JT, Kong JCH, Warrier SK, Heriot A (2021) Robotic versus laparoscopic ileal pouch-anal anastomosis (IPAA): a systematic review and meta-analysis. Int J Colorectal Dis 36:1345–1356
Shrestha B (2016) Minimally invasive surgery for inflammatory bowel disease: current perspectives. World J Gastrointest Pharmacol Ther 7:214–216
Acknowledgements
The authors would like to acknowledge the role of the Johns Hopkins Surgery Center for Outcomes (JSCOR) for supporting this study.
Funding
Shannon N. Radomski received financial support from National Cancer Institute (NCI) Grant 5T32CA126607-12. Mr. Edwin Lewis provided generous support of Dr. Efron’s Department of Surgery Research Fund. The Nicholl Family Foundation provided generous support of the Johns Hopkins Division of Colorectal Surgery Research Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Vincent J. Obias formerly served as a consultant for Intuitive Surgical, Inc. Shannon N Radomski, Miloslawa Stem, Michael Consul, Jay Rammohan Maturi, Haniee Chung, Susan Gearhart and Ada Graham have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Radomski, S.N., Stem, M., Consul, M. et al. National trends and feasibility of a robotic surgical approach in the management of patients with inflammatory bowel disease. Surg Endosc 37, 7849–7858 (2023). https://doi.org/10.1007/s00464-023-10333-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10333-1