
Abstract
Background
Laparoscopy has enjoyed improvements over the last three decades primarily in achieving high definition, but the 70° field of view (FOV) remains unchanged. Complications related to events that take place out of the FOV continue to be reported. Additional problems leading to poor visualization are fogging and smoke accumulation. A novel laparoscopic system (SurroundScope, 270Surgical) was developed and dramatically expands the FOV from the 70° to 270° by adding side cameras at the distal tip of the laparoscope, while LED illumination eliminates fogging and improves smoke effects. This study describes the initial clinical experience with SurroundScope and its potential advantages over traditional laparoscopy.
Methods
SurroundScope was studied at Bnai Zion Medical Center in Israel and the Minnesota Institute for Minimally Invasive Surgery in America. 27 laparoscopic surgeries were performed, and at the end of each procedure, evaluations were completed by all surgeons and camera holders.
Results
All 27 cases were completed successfully without adverse events. No injuries occurred as a result of surgical tool manipulation outside of the central frame while 133 potentially adverse events were identified on side frames. There was no fogging across the 27 cases. The impact of smoke was negligible in all cases, as laparoscope removal or venting was never necessary. Surgeon respondents indicated that tools could be followed from the port to the site of surgery without camera manipulation. Most surgeons strongly agreed that the potential to identify bleeding was improved. Camera holders strongly agreed that the ergonomics were improved and that they moved the camera less than with a standard laparoscope.
Conclusions
Initial results demonstrate numerous advantages for SurroundScope as compared to traditional laparoscopy. The important benefits of expanded FOV, complete lack of fogging, and negligible smoke may improve patient safety, reduce adverse events and the duration of surgery. Further investigation to quantify these benefits is recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Laparoscopic surgery is the preferred approach for most abdominal procedures. Benefits of laparoscopic surgery include smaller incisions, less blood loss, less pain, quicker return to activity and work, reduced adhesion formation, reduced wound infections and improved cosmetic results [1, 2]. Many laparoscopic procedures can be performed in the outpatient setting, reducing hospital utilization and length of stay.
However, one of the primary limitations of laparoscopy has been visibility, due to a narrow field of view (FOV) and compromised image quality due to fogging, smoke formation, and smudging from contact with patient tissue [3]. Also, due to the narrow angle of the laparoscope, the surgeons often settle for a suboptimal camera view. Instruments are often outside of the field of view which can lead to iatrogenic injury.
Poor visibility results in poor depth perception and longer operation times, which may compromise patient outcomes. Poor visibility increases the risk of a missed iatrogenic injury which often requires reoperation [4,5,6]. To improve the performance of laparoscopy, surgeons must be properly trained and provided with appropriate tools to succeed.
Previously, a retrospective study designed to characterize intraoperative technical error-event patterns in successful laparoscopic procedures was conducted. By reviewing procedural video clips, it was reported that out of 54 procedures, there were 66 adverse events in 38 of them, while 75% were not noticed by the team. The underlying cause of these unnoticed events and the ‘near misses’ (i.e., situations and minor events that had the potential to result in an injury or adverse outcome but failed to do so due to chance or through appropriate countermeasures) may be an intraoperative technical error or off-screen injury or potential injury [7].
A recent laboratory study demonstrated that surgeons may benefit from multi-perspective visualization during laparoscopy, and that qualitative feedback indicates strong preference for the multi-perspective visual setup, especially the added aerial view [8]. Prior to this study, the benefits of a wide field of view during surgery was unrecognized.
Materials and methods
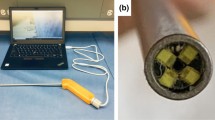
This purpose of the study was to review the utility of a new laparoscopic surgical system, SurroundScope. The video assembly unit of this system, which provides the expanded FOV and improved image characteristics, is located at the endoscope’s distal tip. The distal tip is equipped with a central color image sensor that covers an angle of 95°–115°. The distal tip also has side sensors that can extend the FOV at the press of a button to up to 270°. The system is also designed to eliminate lens fogging and to improve visualization through smoke. The purpose of this development is to provide a much wider field of view during laparoscopy, which allows surgeons to operate more efficiently without need for a higher level of skill or training than that currently required to perform laparoscopic surgery.
This open label study was prospectively conducted between December 2018 and February 2020 at the Bnai Zion Medical Center (BZ) in Haifa, Israel and the Minnesota Institute for Minimally Invasive Surgery (MIMIS) in Crosby, MN, USA. The study protocol was approved by Western Institutional Review Board for the trial performed at MIMIS and the BZ Ethical Committee and Israeli Ministry of Health (IMOH). The study was performed in accordance with the protocol, and all participants provided written informed consent prior to participation.
Adults scheduled for general laparoscopic surgery with the participating surgeons during the separate trial periods at each site were asked to participate in this study. 37 laparoscopic procedures were performed, 27 procedures at BZ Medical Center and 10 at MIMIS. Procedures were performed using the standard operative technique preferred by each participating surgeon, but with the SurroundScope for visualization instead of a traditional laparoscope.
The image produced on the 270 System screen is a combination of three pictures, and includes a central frame similar to the view obtained with a standard laparoscope. The frame provides a wider than usual FOV (95° angle vs 70° with standard laparoscopy). The additional two side frames provide the complete 270° FOV (Fig. 1).

Events classification examples (top images, only the central screen is on; bottom images, all screens are on). A Surgical work. B Non-standard angle of view. C Continuing manipulation from central to side screen. D Manipulation of tissue on side screen. E and F Avoiding potential injury
All procedures were recorded for later analysis. During each case, events occurring on the side frames were documented. Events were defined as significant activities or occurrences observed on the side frames without moving the camera. The captured events were classified into groups, aiming to generate an event log of activities that usually are missed while working with the standard narrow field of view.
A survey including sets of questions regarding the functionality of SurroundScope was presented to participating surgeons and camera holders after each case. Surgeon and camera holder satisfaction with SurroundScope compared to standard laparoscopy was evaluated using 1 to 5 Likert scale. Claims were statistically compared to good agreement threshold using the one-sample Wilcoxon test. Differences between type and complexity of procedures were compared using the Mann Whitney test. P values < 0.05 were considered statistically significant. Statistical analyses were carried out using SPSS 25.0.
Results
The 270System was successfully used in 37 general laparoscopic procedures without any adverse events related to the system. The operations covered the broad spectrum of general surgery as demonstrated in Table 1.
Users
A total of 22 assessments were obtained from the MIMIS surgeons. 27 assessments were obtained from the BZ surgeons and an additional 27 assessments from the BZ camera holders.
Surgeons and their experience are detailed in Table 2. The surgeons at MIMIS were slightly more experienced compared to BZ (median 19 years at MIMIS vs 14 years at BZ).
Side frame events log
More than 258 events were captured on the side frames while operating with the SurroundScope. Events were captured to create an "Events Log" and were classified as follows: surgical work; non-standard angle of view work or observation; continuing surgical manipulation from the central to the side frame; gripping of tissues at the side frames; and avoiding potential injury. Examples for the different events type can be seen in Fig. 1. At least six potential complications were avoided by the ability to continuously view the tools, ports and surgical work. They included identification of bleeding on the side frames, premature removal of a trocar, the ability to visualize safe insertion of laparoscopic instruments, and manipulation of sharp instruments and needles without causing iatrogenic injury. Several examples of the benefits of the SurroundScope are highlighted in Video 1.
Ability to follow tools and ports safety
Thirty-seven surgeons’ assessments on the percentage of time tools could be followed and ports could be visualized were obtained at BZ and MIMIS (Table 3, Fig. 2). 100% reported that tools were visualized most of the time (71–100%). 75.7% reported that ports were visualized most of the time (71–100%). At BZ, 96.3% of assessments reported that ports can be visualized most of the time. 100% of the MIMIS surgeons reported that tools and ports could be continuously followed more/much more than standard (Table 4).

Percent of time tools and ports visualized. Light green 71–100%, medium green 31–70%, dark green 0–30%
Surgeon’s assessments
Twenty-two surgeons’ general assessments of the SurroundScope were obtained at MIMIS. Each participating surgeon completed an assessment for each procedure. Additional participating surgeons often served as camera holder, and also completed an assessment at the completion of the procedure. This resulted in two or three assessments per procedure. A score of 1 through 5 was selected for each question (1 = Strongly disagree; 2 = Disagree; 3 = Neither agree nor disagree; 4 = Agree; 5 = Strongly agree).
Results of the MIMIS surgeon’s assessments are seen in Fig. 3. At MIMIS, the average score ranged from 4.0 to 4.9. All claims, except of improvement of hand eye coordination, demonstrate significantly more than “good agreement” (score 4, p < 0.04). There were no significant differences between complex and intermediate procedures (p > 0.494).

Surgeon’s assessments (MIMIS)
Figure 4 shows results of 27 assessments completed by surgeons at BZ. The average agreement ranged from 3.7 to 4.9. Several claims demonstrate significantly more than “good agreement” (score > 4) p < 0.04. There was high satisfaction with no significant difference between complex and intermediate procedures.
An additional 27 assessments were obtained from the BZ Camera holders (Fig. 5). The average agreement ranged from 4.0 to 5.0, demonstrating good agreement with all claims. There was total agreement with the ergonomics of the system’s handle.

Surgeon’s assessments (BZ)

Camera holder assessments (BZ)
Presence of fog and smoke
During all 37 procedures at both sites, the SurroundScope was never withdrawn due to fogging. Additionally, 27 surgeons’ assessments on visual impairment due to smoke were obtained in BZ. As demonstrated in Table 5, although smoke was present during the procedures, it did not interfere with the procedure.
Discussion
This study demonstrates the superior performance of SurroundScope during laparoscopic procedures. SurroundScope provides a much wider field of view compared to standard commercial laparoscopic cameras. This study included a wide variety of laparoscopic procedures to test the performance of SurroundScope. Operations were performed by surgeons having a wide range of experience, skills and surgical methods. Additionally, the procedures included in this study varied in complexity, which was defined following each case by the operating surgeon.
Each operation was considered a technical success. No adverse events occurred during the trial, supporting the safety of SurroundScope during laparoscopy.
Analysis of the events captured on the side frames as well as the assessments completed by the surgeons and the camera holders suggested improved safety during surgery due to the increased field of view. This view includes ports, instruments and the surgical field, which allows more instruments to work in parallel in different areas of the surgical field. No injuries occurred as a result of surgical tool manipulation outside of the standard operative frame, while plenty of potentially adverse events that were identified on the side frames could be either observed or even manipulated to avoid injury. Additionally, surgeon respondents indicated that the tools could be followed from the port to the site of surgery 71–100% of the time without camera manipulation, as a result of port visibility on the side frames. This benefit could improve safety and enhance workflow. The potential to identify bleeding and the overall perception of safety was improved using the 270 System.
The awareness of the surgical field provided by the SurroundScope improved intra-operative planning and execution of the surgical procedure. The ability to simultaneously map the entire surgical field, can optimize placement of trocars. Operations covering a wide field including a total abdominal colectomy, diagnostic laparoscopy, and Roux-en-Y gastric bypass were performed with the SurroundScope and highlighted the benefit of the wide field of view.
SurroundScope uses LED for illumination thus preventing fog to accumulate on the lens and eliminating the need for disruptive removals of the laparoscope for cleaning. The improved visibility through smoke was designed using the combination of the image processing and illumination.
Loss of visual acuity during laparoscopic procedures is a source of frustration with potential costs to patient safety and increased operative time. This is compounded given that tactile feedback is limited and subsequent visual prompts are paramount to safety [9]. Few approaches to manage fogging have been reported and most techniques are cumbersome, requiring additional extraction and re-insertion of laparoscopic equipment [3, 10]. Despite many efforts to reduce lens fogging, including uses of warm saline, anti-fog solutions, chlorhexidine, betadine, self-heating scopes, and rubbing the lens on serosal surfaces, there has yet to be an adequate method to prevent fogging and pauses due to impaired visualization [2]. The results from the current study indicate the SurroundScope can eliminate lens fogging. There was no incidence of fogging across all cases in the trial. The impact of smoke was negligible in all cases, as the number of incidents requiring scope removal or venting was zero and the smoke events were defined as either imperceptible or perceptible but not interfering. Assessments completed by camera holders participating in the study indicate that the perceived amount of camera manipulation is much less than compared to traditional laparoscopy. Surgeons felt that either due to the camera structure or the minimal camera manipulation, the scope was kept relatively clean during the procedures. Also, if a single lens is ‘smudged,’ camera holders were able to safely improvise and use the additional cameras to complete a critical task.
Assessments completed by surgeons and camera holders revealed the improved ergonomics of SurroundScope. The system does not include a light cable or sterile sleeve, and its overall weight is decreased. Minimal camera manipulation resulted in improved communication between surgeons and camera holders. Surgeons confirmed that the work with the 270 System becomes intuitive with minimal clinical training.
In summary, just as side mirrors on motor vehicles are essential for safety, so is the importance of side views during surgery. The side frames enable tracking of laparoscopic instruments as they safely approach the target, and prevent injuries to organs normally outside the FOV. In addition, removal of instruments and resected specimens occurs easily without moving the camera. Expanding the FOV to allow peripheral vision simulates the human eye and naturally adds the overall perception of safety and operative control. While focusing on the details of the procedure being conducted on the central frame, by only glancing slightly toward either side of the frame, one can visualize the entire cavity and avoid injuries.
The concept of providing a wide-angle 270° view of the abdomen, with minimal camera movement, was highly valued among the surgeons and camera holders in this study. Initial results demonstrate numerous advantages for SurroundScope as compared to traditional laparoscopy. The potential important benefits of an expanded FOV, the lack of fogging, and negligible smoke include improvements in safety and surgical techniques, duration of surgery, and a reduction in adverse events. In addition, the reduction in laparoscopic camera movement may lead to the elimination of camera holder personnel in favor of a mechanical camera holder.
Surgeries involving four and sometimes even six hands working in parallel, exhibited new possibilities only made possible by expanding the entire surgical field. This is enabled due to the wide view and stable image that is provided by the extended FOV. New possibilities may include more efficient surgical work of laparoscopic procedures or laparoscopic performance of surgeries that are currently performed in the open method.
This study represents the first clinical trial reporting the benefits of a laparoscopic camera system that dramatically expands the field of view. While additional research is necessary to explore the potential benefits of multi-perspective visualization in surgical cases, the SurroundScope system was found to not only improve multi-perspective visualization, but also eliminate the problem of fogging and improve visualization through smoke accumulation. Further investigation to measure outcomes is now needed as this novel development in laparoscopic surgery has the potential to improve patient safety and expand the reaches of minimally invasive surgery.
References
Abbitt D, Khalloug BB, Redan J (2017) Quantifying intraoperative laparoscopic visual field opacity. JSLS. https://doi.org/10.4292/JSLS.2017.00004
Song T, Lee DH (2019) A randomized Comparison of laparoscopic lens defogging using anti-fog solution, waRm saline, and chlorhexidine solution (CLEAR). Surg Endosc. https://doi.org/10.1007/s00464-019-06852-5
Lawrentschuk N, Fleshner NE, Bolton DM (2010) Laparoscopic lens fogging: a review of etiology and methods to maintain a clear visual field. J Endourol. https://doi.org/10.1089/end.2009.0594
Roviaro GC, Varoli F, Saguatti L, Vergani C, Maciocco M, Scarduelli A (2002) Major vascular injuries in laparoscopic surgery. Surg Endosc. https://doi.org/10.1007/s00464-001-8238-z
Way LW, Stewart L, Gantert W, Liu K, Lee CM, Whang K, Hunter JG (2003) Causes and prevention of laparoscopic bile duct injuries: analysis of 252 cases from a human factors and cognitive psychology perspective. Ann Surg. https://doi.org/10.1097/01.SLA.0000060680.92690.E9
Michaelson MD, Cotter SE, Gargollo PC, Zietman AL, Dahl DM, Smith MR (2008) Management of complications of prostate cancer treatment. CA Cancer J Clin. https://doi.org/10.3322/CA.2008.0002
Bonrath EM, Gordon LE, Grantcharov TP (2015) Characterizing ‘near miss’ events in complex laparoscopic surgery through video analysis. BMJ Qual Saf. https://doi.org/10.1136/bmjqs-2014-003816
Sanford Z, Turner R, George I, Addo A, Mentis H, Zahiri R, Weltz AS, Park A (2017) A novel use of multi-perspective two-dimensional versus single perspective two-dimensional view in laparoscopy. In: SAGES annual meeting poster presentation abstract ID: 95181
Manning TG, Papa N, Perera M, McGrath S, Christidis D, Khan M, O’Beirne R, Campbell N, Bolton D, Lawrentschuk N (2017) Laparoscopic lens fogging: solving a common surgical problem in standard and robotic laparoscopes via a scientific model. Surg Endosc. https://doi.org/10.1007/s00464-017-5772-x
Manning TG, Perera M, Christidis D, Kinnear N, McGrath S, O’Beirne R, Zotov P, Bolton D, Lawrentschuk N (2017) Visual occlusion during minimally invasive surgery: a contemporary review of methods to reduce laparoscopic and robotic lens fogging and other sources of optical loss. J Endourol. https://doi.org/10.1089/end.2016.0839
Funding
This research was funded by the 270Surgical Ltd. company.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
I Matter reports an equity interest in and serves on the advisory board of 270Surgical. Dr. Severson reports personal fees from Johnson & Johnson, personal fees from DyaMx, Inc, and serves on the advisory board of Microline Surgical. Dr. McCollister reports personal fees from Johnson & Johnson and DyaMx, Inc. Drs. Sroka, Laniado, Thompson, and Loveitt have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 89986 KB)
Rights and permissions
About this article

Cite this article
Thompson, K.J., Sroka, G., Loveitt, A.P. et al. The introduction of wide-angle 270° laparoscopy through a novel laparoscopic camera system. Surg Endosc 36, 2151–2158 (2022). https://doi.org/10.1007/s00464-021-08451-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08451-9