
Abstract
Background
Due to improvements in endoscopic as well as robotic technology, and a request for better cosmetic results, there was a significant increase in thyroid surgery using these methods during the past decade.
Methods
The aim of our study is to evaluate the perioperative short- and long-term outcome as well as the learning curve of EndoCATS and the Quality of Life (QoL).
Results
A total of 150 patients with 152 hemithyroidectomies who underwent endoscopic thyroid surgery by EndoCATS between 2010 and 2016 were enrolled in this study. The mean specimen volume was 15.04 g ± 7.89 g. The mean operation time was 132.79 ± 50.52 min. There is a significant reduction of the operation time after the 53th case. (p < 0.05) There was no acute rebleeding or permanent hypoparathyroidism. Permanent RLN palsy occurred in 3 nerves at risk (NAR) 1.97%. There were no cases of pneumothorax, postoperative infections or skin flap ischemia. 94.11% of the patients describe their state of general health as good as or better than before the surgery.
Conclusions
EndoCATS is a safe and effective, but a demanding single port access procedure; therefore, extensive training is required. An advantage is the near ideal visualization of the RLN and the parathyroid glands as well as the ability to recover even large specimens without difficulties.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In 2008, Schardey et al. first described the videoendoscopic thyroidectomy by the dorsal retroauricular approach (RA) (EndoCATS) feasible not only in human cadavers, but also in patients [1]. The first patient was operated on in November 2006. The procedure leaves no visible scars in the neck, as the incision is in the hairline at the edge of the scalp. Nodal points are helpful for executing this new operation in the beginning. The surgical quality score presented in the first report is a complex and objective measure of ability of leaners to deal with the procedure. The initial report was succeeded by a prospective clinical feasibility study on 30 patients [2]. After this feasibility trial the procedure was reevaluated experimentally focusing on solving the problems of access related nerve lesions, mostly of the accessory nerve crossing the sternocleidomastoid muscle [3]. The procedure was then modified into its final form being carried out about 20 times per year at our high-volume of thyroid surgical center. The main difference was that the initial approach to the thyroid was medial to the sternocleidomastoid muscle (SCM), which caused problems with the accessory nerve in 5%. This problem could be eliminated by approaching the thyroid from above, meaning lateral or superficial to the SCM. Distal to the omohyoid muscle the thyroid was then approached by passing between the sternal and clavicular heads of the SCM entering De Quervains space.
In 2010 Walvekar presented an experimental study on human cadavers using a modification of the retroauricular approach (RA) by extending the incision from the scalp to behind the ear lobe and actually lifting a skin flap [4]. The first clinical use of this approach was reported by Terris in 2011 [5]. Over the last decade unilateral RA thyroid surgery mostly using a laparoscope and later a robot has spread worldwide [1, 2, 4,5,6,7,8,9,10]. RA thyroid surgery has many names. Surgeons using the Walvekar technique lifting a skin flap mostly called it face-lift thyroid surgery while we called our technique Endoscopic Cephalic Access Thyroid Surgery (EndoCATS).
Due to improvements in endoscopic and robotic technology as well as an increase in surgical experience with these techniques there was a significant increase in endoscopic thyroid surgery in the past decade. The different RA approaches have even been used in complex interventions e.g. for inflammatory thyroid disease and neck dissection in differentiated thyroid malignancies [11]. Despite these advances some factors should be considered in a careful patient selection: underlaying thyroid pathology, size of thyroid gland, extra-thyroidal invasion and suspicious lymphadenopathy [12].
Concerning the RA thyroidectomy, published data could show that it is not only technically feasible, but safe and with highly satisfactory cosmetic results [9, 13]. The RA when using a robot even seems to be beneficial for reducing operation time and hospital stay [9].
The American Thyroid Association (ATA) Statement on Remote-Access Thyroid Surgery acknowledged several barriers to implementation of minimally invasive thyroid surgery, including a limited published experience for the several remote access techniques, many of which utilize a robotic platform [12]. With more and more published data, not only for RA but for all available endoscopic and robotic approaches in thyroid surgery, a more comprehensive understanding of the potential and limitations of these procedures is now available [8, 10]. However long-term results are still rare.
The aim of our study is an evaluation of the short- and long-term perioperative outcome, the learning curve of EndoCATS, as well as the quality of life (QoL) after surgery.
Materials and methods
This is a single center retrospective data analysis. All procedures were performed at the Department of General, Visceral, Vascular and Endocrine Surgery, Agatharied Academic Teaching Hospital, Ludwig-Maximilians-University Munich, a high volume center for thyroid surgery with more than ten years of clinical experience in endoscopic thyroid procedures using the EndoCATS, Axillo-Bilateral-Breast-Approach (ABBA), and Transoral Endoscopic Thyroidectomy (Vestibular Approach, TOETVA) and our latest modification of the transoral technique Transoral Thyroid Surgery Vestibular and Retro auricular Approach: (TOVARA) [14]. Until now, more than 500 endoscopic thyroidectomy procedures have been carried out at our institution. All EndoCATS procedures performed at our institution between 2010 and 2016 were included in analysis; the initial 30 cases performed between 2006 and 2008 have already been reported in the feasibility study [2].
Patients
The EndoCATS procedure is used for unilateral thyroidectomy in patients with a one sided pathology of the thyroid gland with an estimated volume of less than 45 ml. Only patients asking for the endoscopic procedure were assessed and operated with EndoCATS. Patients with unilateral pathology and a lobal volume of more than 45 ml as well as those requiring bilateral thyroidectomy were operated with the ABBA technique and at the end of 2016 with TOETVA. Patients asking for invisible scar thyroidectomy procedure find EndoCATS most appealing since they never ask for ABBA or TOETVA. Patients with previous irradiation or surgery of the neck, extrathyroidal disease and planned neck dissection we excluded from this procedure. All patients, who underwent endoscopic thyroid surgery by the EndoCATS approach between 2010 and 2016 were enrolled in this study. A total of 150 patients could be included. Bilateral EndoCATS procedures were carried out only twice in two young female patients with Graves disease, so 152 surgical procedures were performed with 152 nerves at risk (NAR). Written informed consent was obtained from all patients. This study was approved by the local review board (reference number 17–054).
Patient demographics (age, gender, ASA score), perioperative data (operative time, diagnosis, specimen size, complications, length of hospital stay) and pathological characteristics were retrospectively documented. Operative time was defined as the time from initial skin incision to final skin closure.
The primary endpoint of this study was the rate of postoperative complications: recurrent laryngeal nerve (RLN) injury for NAR, hypocalcemia, hypoparathyroidism and bleeding complications. Permanent RLN palsy was defined as persistent vocal cord dysfunction for six months or longer from the time of surgery. Temporary hypocalcemia was defined by symptomatic hypocalcemia requiring calcitriol and calcium supplements in the immediate postoperative period. Permanent hypoparathyroidism was defined by low or undetectable parathyroid hormone level requiring calcium and Vitamin D supplementation for six months or longer from time of surgery. Furthermore, a learning curve based on the duration of surgery was calculated.
In addition, a prospectively questionnaire based follow up was carried out about complications specific for the RA remote access (pain in the cervical spine, swelling of the neck, changes of sensation at the scar and in the surgical field). The intake of iodine or thyroid hormone substitution and postoperative satisfaction with cosmetic result and SF – 12 quality of life score was used [15, 16]. The SF-12 score assesses twelve items concerning physical functioning, role limitations, physical pain, health perception, energy level, social functioning, and psychological well-being, resulting in physical and mental health composite scores.
Surgical procedure (Fig. 1)

A Positioning of the patient; B skin incision, and dissection area; C Flap elevation; D 1. position of the spatula; E spatula is fully inserted; F division of the SCM; G Ligation of superior thyroid vessels; H endoscopic assistance to preserve parathyroid gland
All procedures were performed by a team of two surgeons. Under general anesthesia, the patient is placed in the supine position with the head rotated (30°) to the contralateral side of the dissection. Intermittened laryngeal nerve monitoring is used during the procedures. The patient is intubated with a laryngeal EMG tube (Dr. Langer Medical GmbH, GERMANY). Approximately 1 cm of hair was shaved along the retro-auricular occipital hairline.
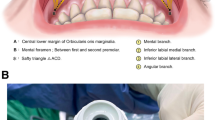
A 4 cm skin incision in the scalp dorsal to the mastoid bone is carried out. The ventral fascial sheath of the SCM is opened and the virtual space between the ventral fascial sheath and the ventral surface of the SCM becomes accessible. Sharp dissection with scissors is carried out until blunt dissection with the retractor spatula (Storz Endoscopes, Tuttlingen, Germany) becomes possible and the endoscope is inserted. This retractor spatula contains a channel for an endoscope (Fig. 2). We use the IMAGE1 S™ video and endoscopes with diameter of 4 mm. (Storz Endoscopes, Tuttlingen, Germany) Ventral traction must be used carefully since it can cause damage of the greater auricular nerve. After the identification of the omohyoid muscle the spatula is passed medially and below this structure and after that more caudally between the sternal and clavicular head of the SCM. The carotid sheath with the jugular vein, Carotid artery and vagal nerve are then identified and opened. Blunt dissection is then carried out with the probe from the nerve monitor and following its identification -, the vagal nerve signal is documented by nerve monitoring (AVALANCHE®, Dr. Langer Medical GmbH, GERMANY). The next step consists of entering the surgical space of De Quervain with the retractor spatula by blunt dissection. After fully exposing the surface of the thyroid gland and establishing an adequate working space, the Spatula is fixed to a self-retaining readjust able retractor (Storz Endoscopes, Tuttlingen, Germany).

A reusable spatula developed for the procedure with an integrated 5 mm channel for laparoscope
The superior pole is mobilized away from the inferior constrictor muscle, after the external branch of the superior laryngeal nerve (SLN) is identified with the help of the nerve monitoring (AVALANCHE®, Dr. Langer Medical GmbH, GERMANY)., and the vascular pedicle is sealed and divided with the Harmonic scalpel (HS) HARMONIC ACE®, Ethicon Inc., USA). The superior pole is then reflected ventrally and inferiorly and the superior parathyroid gland identified and dissected postero-laterally away from the thyroid gland. The recurrent laryngeal nerve (RLN) is identified just proximal to its entrance beneath the inferior constrictor muscle and its function documented by nerve monitoring. The ligament of Berry is divided having the nerve under direct vision and then the isthmus can be transected. The middle thyroid vein is divided using the HS, and the inferior pole is then fully mobilized using blunt dissection. The inferior parathyroid gland is identified and dissected laterally away from the thyroid gland. The inferior thyroid artery and vein, the remaining attachments of the gland are divided and the thyroid lobe is retrieved through the retroauricular incision. Finally, the integrity of RLN, SLN and vagal nerve are documented by nerve monitoring. The skin is closed using a running self-absorbable suture. Figure 3 shows the scar 7 days, 14 days and 1 year after surgery (Fig. 3). For pain control we use a standardized medication like in our conventional open surgical cases [17]. All patients receive an injection of local anesthetic around the incision after skin closure followed by an oral analgesic regimen started before surgery consisting of etoricoxib 120 mg once daily and metamizole 500 mg four times per day [17].

Scar 7 days, 14 days and 1 year after surgery
Due to the neuromonitoring a lesion to the RLN can be directly proven intra operatively. To differentiate between temporary or permanent RLN all patients were examined for hoarseness postoperatively. All patients with abnormal findings during neuromonitoring or voice changes were re-examined with laryngoscopy after at least 6 months post surgery.
Statistics
A χ2-test was used to examine associations between categorical variables, and an unpaired two-tailed student’s t-test for continuous variables. Mean, standard deviation (SD) and range (min–max) are calculated. Analyses were performed with SPSS 22 (IBM, Armonk, NY, USA). The cumulative sum control chart (CUSUM) was used to determine changes in operation time and calculation of a learning curve. p-values α < 0.05 were considered statistically significant.
Results
Demographic and clinical features (Table 1)
The mean age of the n = 150 patients was 47.08 years (SD ± 11.97; range 21 to 80 years). There were 139 female and 11 male patients. Bilateral procedures were carried out only twice. So there were 152 NAR. ASA score, mean duration of hospital stay and duration of surgery are shown in Table 1.
Perioperative outcome (Table 2)
There were 139 (91.45%) benign lesions and 13 (8.55%) cases of differentiated thyroid cancer. The mean specimen volume was 15.04 g (SD ± 7.89 g; 2 g to 50.7 g). The mean operation time was 132.79 ± 50.52 min. Operative times decreased significantly along with surgeons’ experience. The CUSUM curve showed a decrease from the 53th case on; there is a significant reduction of the operation time compared the cases before and after the 53rd case (p < 0.05), whereas the specimen size stayed constant over time. (Fig. 4).

Learning curve
Surgical complications using the EndoCATS approach included temporary dysphonia in 20 (17.24%) patients and 18 (11.84%) cases of transient hypocalcemia without cases of permanent hypocalcemia or hypoparathyroidism. There were no cases of pneumothorax, postoperative infections or skin flap ischemia. There were no cases of seroma, but four cases of local, access-related hematomas. These bruises occurred just below the ear; one underwent endoscopic revision but was found to be only a minor (2 ml). There were no cases of postoperative rebleeding requiring emergency redo surgery. Permanent RLN palsy occurred in 3 NAR (1.97%).
Long term outcome (Table 3)
The mean follow up period was 37.38 months (median 53.2; SD, ± 146). After thyroid surgery 73.77% of the patients were taking iodine or thyroid hormone substitution. 34.65% reported a temporary swelling in the neck, with a median duration of 14 days after surgery. Postoperative pain in the cervical spine was reported by 17.65% of patients and 60.61% reported of a transient numbness in the area of the retroauricular scar with a median duration of 32.5 days; in 11.11% of these cases, the numbness persisted. Most of the patients (93.86%) were satisfied with the surgical result and would undergo endoscopic thyroid surgery again. Only 3.51% and 2.63% were slightly or not satisfied. As can be expected, patients without complications are significantly more satisfied than patients with complications (p < 0.05).
One week postoperatively, 90.99% patients had only little or no pain and 68.75% of patients had no or hardly any pain immediately after surgery.
SF 12 QoL
The response rate for participation in the follow-up questionnaire was 76.00% (114/150). The mean follow up is two years. 94.11% (107 patients) of responding patients describe their state of general health as good or at least better than before thyroid surgery. 10.89% reported emotional problems with their work or other regular daily activities. 84.16% of patients seldom or never have problems with social functioning. 79.41% of patients do not experience any problems when doing hard physical work. 88.12% of patients are rare or never discouraged or sad.
Discussion
A total of 150 patients underwent endoscopic thyroid surgery by EndoCATS from 2010 until 2016 and were included in the retrospective analysis of this single center experience. All procedures were performed by a team of two surgeons. Bilateral procedures were carried out only twice. In two young female patients with graves disease this was carried out for bilateral thyroidectomy. All in all, 152 hemi-thyroidectomies have been performed with 152 nerves at risk (NAR). We registered 3 cases of permanent RLN palsy (1.97%), no cases of acute rebleeding requiring emergency surgery, 11.84% of transient hypocalcemia and no cases of permanent hypoparathyroidism.
Although the overall sum of complications seems rather good we see of the rate of RLN palsy fall back behind the RLN paly rate of less than 1% which we can achieve in open thyroidectomy. So there is room for improvement. However when looking at the literature the complication rate of conventional thyroid surgery for RLN palsy lies between 0.3 and 6% [18, 19]. In a recent study from 2020 on 11,370 patients, who underwent either lobectomy or total thyroidectomy were reported using the American College of Surgeons National Surgical Quality Improvement Program thyroidectomy-specific database (2016–2017) [19]. LN injury occurred in 6.0% (n = 677) of the 11,370 patients included in the study. The RLN injury rate varied significantly based on the primary indication for surgery, from 4.3% in patients undergoing surgery for a single nodule to 9.0% in patients undergoing surgery for differentiated cancer (P < 0.01). RLN injury occurred more often in thyroidectomies than lobectomies (6.9% versus 4.3%, P < 0.01) and more often in operations without intraoperative nerve monitoring (6.5% versus 5.6%) [19]. A Review of 66,902 thyroid gland operations in 2017 in Germany reports an overall frequency of permanent vocal cord palsy of 1.5%.[20], Rebleeding (0–6.5%), infections (1–3%), temporary hypocalcaemia 6,5–23.6% and permanent hypoparathyroidism of 2% [18, 20,21,22,23,24]. inglooking at center experienceoidectomy. So there is less than on % out. minor (2 ml)ma be only ve monitoring (s diseaseCATS most appealing since they never ask for ABBA or TOETVA. thyroidectomy were.
Complication rate for RA are not conclusive, because only very small case numbers have so far been reported. The numbers vary from 4–54 cases [2, 5, 24,25,26,27,28,29]. The rate for RLN palsy varies between 0 and 5.5%, for hematoma 0–5.6%, transient hypocalcemia 25% and for infections 0% [2, 5, 12, 24,25,26,27,28,29].
Compared to the recently published data, our series seems to have an acceptable complication rate for a newly developed endoscopic technique [19].
There is no obvious difference in complication rates (rebleeding, infections and permanent hypoparathyroidism) between EndoCATS other RA procedures and conventional thyroid surgery. [18, 20,21,22,23, 30]. However, the degree of evidence is low as there are no results from prospective randomized trials.
In addition to the good cosmetic results and high patient satisfaction EndoCATS has several advantages. In our opinion the visualization of the RLN and the parathyroid glands is excellent when using the EndoCATS technique in comparison to other remote approaches we regularly use. We cannot prove this by our data, but up to now, we have experience with more than 500 endoscopic thyroid surgeries using different remote approaches as described above. A good view on the critical structures is confirmed by other authors using RA [11]. This is in particular true for those using a robotic technique, which can provide a three-dimensional 10–12-fold magnified view [31].
EndoCATS requires a great deal of experience in endoscopic thyroid surgery. The main challenge and difficulty of EndoCATS is the single port approach with the restricted movement in a limited space. Triangulation of instruments is limited. Another factor is that the midline is not opened as in ABBA, transoral or conventional open techniques, limiting the surgical space. In that respect we do agree with Sung et al. [32] and a contralateral lobectomy requires a contralateral incision. Other authors considered the unusual perspective to be a reason for RLN injury [31].
Access-specific complications such as numbness around the skin incision was mostly a temporary phenomenon. Wound infections or skin flap ischemia as described in up to 2.3% of cases by other groups did not occur in our surgical procedures [33]. Many working groups use the approach described by Terris et al. a very long retroauricular incision extending to the hairline lifting a skin flap [5, 27]. We only use a 4 cm skin incision in the scalp dorsal to the mastoid bone[1,2,3], which does not result in skin flap ischemia.
The approach related dissection is much less than required for ABBA. Singer et al. [34] estimated a reduction of 38%. Retroauricular surgery is also considered to be a rather familiar surgically approach, which is widely used in parotidectomy and submandibular gland incision [35,36,37]. There is no risk of brachial plexus injury and no concern of paraesthesia of the anterior chest like in ABBA [38, 39]. Other disadvantages are inherent to the approach like transient hypoaesthesia in the distribution of the greater auricular nerve, which is not uncommon. [40] In comparison to TOETVA, which only allows the removal of very small specimen EndoCATS has practically no limitations concerning this aspect. A clear disadvantage lies in the fact that we are dealing with a unilateral procedure [2]. Nonetheless female patients with a small potentially cancerous lesion are less reluctant to have it removed when a technique using an invisible scar is available. Here the EndoCATS technique has a definite advantage with the scar hidden within the scalp. This is one of the reasons why 93.86% of the patients were satisfied with the surgical result and would undergo endoscopic thyroid surgery again.
Low-volume surgeons with less than 25 interventions per year and are more likely to experience complications (odds ratio 1.51, P = 0.002) and cause longer hospital stays (+ 12%, P = 0.006) [41]. Endoscopic thyroidectomies do require a great deal of experience in video-endoscopic surgery in order to be able to develop the skills required for the proper performance and management of the endoscopic procedure. In addition, a careful and precise selection of patients is important especially the first cases. Experience in conventional open thyroidectomy can be helpful [42]. In our data we found a significant reduction of the operation time after four years and 53 cases (p < 0.05). Lee et al. describe a decrease of operation time and of the complication rate after 50 cases for RA [43]. This is confirmed by other studies reporting endoscopic thyroidectomy procedures (25–60 cases) [31, 42, 44, 45]. Compared to conventional open thyroid surgery, the learning curve is almost twice as high.
Quality-of-life outcomes after surgical procedures always need to be seen in the relation to postoperative adverse events [46]. Promberger et al. showed, that even transient complications that had resolved within 6 months after the operation, including transient recurrent laryngeal nerve palsy, hypocalcemia, or wound infections had a significantly negative influences on postoperative quality of life [43] and satisfaction. This was also seen in our study since patients without complications were significantly more satisfied than patients with complications. (p < 0.05) Complications in thyroid surgery are reported to cause high levels of distress with a long-lasting impact on ‘‘social functioning,’’ ‘‘emotional condition,’’ and ‘‘mental health’’ [46]. We however only found ‘‘social functioning” to be impaired in patients with complications.
Only 76.00% of patients took part in the survey concerning the patient related outcome measures quality of life, cosmetic result and patient satisfaction, therefore some selection bias cannot be excluded in our study. The value of a 93.81% with high rate of satisfaction might be enthusiastic. However, the perioperative in-hospital outcome regarding complications is known for all patients as it is documented in patients’ files. Concerning the patient reported outcome measures, these can be stated as “subjective problems” and it must be taken into account, that only a certain type of patient does ask for such an “invisible scar “ endoscopic thyroid surgery procedure; these patients also have a very high level of expectancy, which might again influence the patient reported outcome in the case complications do occur.
Although our data represent one of the largest series of RA reported with low complication rates, the evidence for retroauricular remote access procedures is low, as most data are generated from retrospective surgical series. More data from randomized multicenter trials would be necessary to finally evaluate these surgical techniques in comparison to other remote access and conventional open procedures, not only in benign but even malignant thyroid disease. One solution to help with the evaluation of results from small series published until now could be the analysis of prospective registry data.
Conclusion
EndoCATS thyroidectomy is a safe and effective procedure with a learning curve comparable to other endoscopic thyroidectomy procedures. The remote endoscopic approach specific complications were moderate, whereas patients’ satisfaction with the cosmetic result was very high. Due to the unconventional view during dissection and the restriction of space due to the single port approach, we recommend extensive training.
References
Schardey HM, Schopf S, Kammal M, Barone M, Rudert W, Herandez-Richter PS (2008) Invisible scar endoscopic thyroidectomy by the dorsal approach: experimental development of a new technique with human cadavers and preliminary clinical results. Surg Endosc 22:813–820
Schardey HM, Barone M, Pörtl S, von Ahnen M, von Ahnen T, Schopf S (2010) Invisible scar endoscopic dorsal approach thyroidectomy: a clinical feasibility study. World J Surg 34:2997–3006
Wirth U, Kammal M, Doberauer J, Graw M, Schardey HM, Schopf S (2011) Invisible scar endoscopic thyroid surgery by the dorsal approach: importance of the spinal accessory nerve. Surg Radiol Anat 33(8):703–711
Walvekar RR, Wallace E, Bergeron B, Whitworth R, Beahm DD, Nuss DW (2010) Retro-auricular video-assisted “gasless” thyroidectomy: feasibility study in human cadavers. Surg Endosc 24(11):2895–2899
Terris DJ, Singer MC, Seybt MW (2011) Robotic facelift thyroidectomy. II Clinical feasibility and safety Laryngoscope 121(8):1636–1641
Dimitrios L (2011) Minimally invasive thyroidectomy: A comprehensive appraisal of existing techniques. Surgery 150:17–24
Schardey HM, Schopf S (2011) Invisible-scar endoscopic thyroidectomy by the dorsal approach. Surg Endosc 25:3472–3473
Bomeli SR, Duke WS, Terris DJ (2015) Robotic facelift thyroid surgery Gland Surg 4(5):403–409
Alabbas H, Bu Ali D, Kandil E (2016) Robotic retroauricular thyroid surgery Gland Surg 5(6):603–606
Lira RB, Chulam TC, Kowalski LP (2017) Safe implementation of retroauricular robotic and endoscopic neck surgery in South America. Gland Surg 6(3):258–266
Tae K, Ji YB, Song CM, Ryu J (2019) Robotic and Endoscopic Thyroid Surgery: Evolution and Advances. Clin Exp Otorhinolaryngol 12(1):1–11
Berber E, Bernet V, Fahey TJ 3rd, Kebebew E, Shaha A, Stack BC Jr, Stang M, Steward DL, Terris DJ, Commitee ATASA (2016) American Thyroid Association statement on remote-access thyroid surgery. Thyroid 26(3):331–337
Byeon HK, Holsinger FC, Tufano RP, Park JH, Sim NS, Kim WS, Choi EC, Koh YW (2016) Endoscopic retroauricular thyroidectomy: preliminary results. Surg Endosc 30(1):355–365
Karakas E, Klein G, Schopf S (2020) Transoral Thyroid Surgery Vestibular Approach: Does Size Matter Anymore? J Endocrinol Invest 43(5):615–622
Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, Bulinger M, Kaasa S, Leplege A, Prieto L, Sulllivan M (1998) Cross-Validation of Item Selection and Scoring for the SF-12 Health Survey in Nine Countries: Results from the IQOLA Project. International Quality of Life Assessment J Clin Epidemiol 5(11):1171–1178
Goldfarb M, Casillas J (2016) Thyroid Cancer-Specific Quality of Life and Health-Related Quality of Life in Young Adult Thyroid Cancer Survivors. Thyroid 26:923–932
Schopf S, von Ahnen M, von Ahnen T, Neugebauer EAM, Schardey HM (2012) Effect of Local Anesthesia and Cox-2 Inhibitors After Thyroid Resection on Postoperative Pain Results of Two Consecutive Randomized Controlled Monocenter Studies. Journal of pain management 5(3):279–287
Hayward NJ, Grodski S, Yeung M, Johnson WR, Serpell J (2013) Recurrent laryngeal nerve injury in thyroid surgery: a review. ANZ J Surg 83:15–21
Gunn A, Oyekunle T, Stang M, Kazaure H, Scheri R (2020) Recurrent Laryngeal Nerve Injury After Thyroid Surgery: An Analysis of 11,370 Patients. J Surg Res 12(255):42–49
Maneck M, Dotzenrath C, Dralle H, Fahlenbrach C, Paschke R, Steinmüller T, Tusch E, Jeschke E, Günster C (2017) Complications after thyroid gland operations in Germany A routine data analysis of 66,902 AOK patients. Chirurg 88:50–57
Dralle H (2015) Surgical assessment of complications after thyroid gland operations. Chirurg 86:70–77
Bergenfelz A, Jansson S, Kristoffersson A, Mårtensson H, Reihnér E, Wallin G, Lausen I (2008) Complications to thyroid surgery: results as reported in a database from a multicenter audit comprising 3,660 patients. Langenbecks Arch Surg 393:667–673
Promberger R, Ott J, Kober F, Koppitsch C, Seemann R, Freissmuth M, Hermann M (2012) Risk factors for postoperative bleeding after thyroid surgery. Br J Surg 99:373–379
Edafe O, Balasubramanian SP (2017) Incidence, prevalence and risk factors for post-surgical hypocalcaemia and hypoparathyroidism. Gland Surg 6(Suppl 1):59-S68
Lee DY, Baek SK, Jung KY (2016) Endoscopic thyroidectomy: retroauricular approach. Gland Surg 5(3):327–335
Kandil E, Saeed A, Mohamed SE, Alsaleh N, Aslam R, Moulthrop T (2015) Modified robotic-assisted thyroidectomy: an initial experience with the retro auricular approach. Laryngoscope 125:767–771
Russell JO, Razavi CR, Al Khadem MG, Lopez M, Saraf S, Prescott JD, Starmer HM, Richmon JD, Tufano RP (2018) Anterior cervical incision-sparing thyroidectomy: Comparing retroauricular and transoral approaches. Laryngoscope Investig Otolaryngol 3(5):409–414
Russell JO, Razavi CR, Garstka ME, Chen LW, Vasiliou E, Kang SW, Tufano RP, Kandil E (2019) Remote-access thyroidectomy: a multi-institutional north american experience with transaxillary, robotic facelift, and transoral endoscopic vestibular approaches. J Am Coll Surg 228(4):516–522
Byeon HK, Holsinger FC, Tufano RP, Chung HJ, Kim WS, Koh YW, Choi EC (2014) Robotic total thyroidectomy with modified radical neck dissection via unilateral retroauricular approach. Ann Surg Oncol 21(12):3872–3875
Byeon HK, da Kim H, Chang JW, Ban MJ, Park JH, Kim WS, Choi EC, Koh YW (2016) Comprehensive application of robotic retroauricular thyroidectomy: The evolution of robotic thyroidectomy. Laryngoscope 126(8):1952–1957
Liu S, Qiu M, Jiang DZ, Zheng XM, Zhang W, Shen HL, Shan CX (2009) The learning curve for endoscopic thyroidectomy: a single surgeon’s experience. Surg Endosc 23(8):1802–1806
Sung ES, Ji YB, Song CM, Yun BR, Chung WS, Tae K (2016) Robotic thyroidectomy: comparison of a postauricular facelift approach with a gasless unilateral axillary approach. Otolaryngol Head Neck Surg 154(6):997–1004
Byeon HK, Holsinger FC, Duvvuri U, Kim DH, Park JH, Chang E, Kim SH, Koh YW (2018) Recent Progress of Retroauricular Robotic Thyroidectomy With the New Surgical Robotic System. Laryngoscope 128:1730–1737
Singer MC, Seybt MW, Terris DJ (2011) Robotic facelif thyroidectomy: I. Preclinical simulation and morphometric assessment. Te Laryngoscope 121(8):1631–1635
Song CM, Jung YH, Sung M, Kim KH (2010) Endoscopic resection of the submandibular gland via a hairline incision: A new surgical approach. Te Laryngoscope 120(5):970–974
Grover N, D’Souza A (2013) Facelif approach for parotidectomy: an evolving aesthetic technique. Otolaryngology-Head and Neck Surgery 148(4):548–556
Song CM, Ji YB, Kim KR, Tae K (2015) Robot-assisted excision of branchial clef cysts using a postauricular facelif approach. Auris Nasus Larynx 42(5):424–427
Terris DJ, Singer MC (2012) Qualitative and quantitative differences between 2 robotic thyroidectomy techniques. Otolaryngology-Head and Neck Surgery 147(1):20–25
Kuppersmith RB, Holsinger FC (2011) Robotic thyroid surgery: An initial experience with North American patients. Te Laryngoscope 121(3):521–526
Sephton BM (2019) Extracervical Approaches to Thyroid Surgery Evolution and Review. Minim Invasive Surg. https://doi.org/10.1155/2019/5961690
Adam MA, Thomas S, Youngwirth L, Hyslop T, Reed SD, Scheri RP, Roman SA, Sosa JA (2017) Is There a Minimum Number of Thyroidectomies a Surgeon Should Perform to Optimize Patient Outcomes? Ann Surg 265(2):402–407
Cao F, Jin K, Cui B, Xie B (2013) Learning curve for endoscopic thyroidectomy: a single teaching hospital study. Onco Targets Ther 6:47–52
Lee DY, Oh DJ, Kang KR, Kim MS, Oh KH, Baek SK, Kwon SY, Woo JS, Jung KY (2016) Comparison of Learning Curves for Retroauricular and Transaxillary Endoscopic Hemithyroidectomy. Ann Surg Oncol 23(12):4023–4028
Liu SY, Kim JS (2017) Bilateral axillo-breast approach robotic thyroidectomy: review of evidences. Gland Surg 6(3):250–257
Kwak HY, Kim SH, Chae BJ, Song BJ, Jung SS, Bae JS (2014) Learning curve for gasless endoscopic thyroidectomy using the trans-axillary approach: CUSUM analysis of a single surgeon’s experience. Int J Surg 12(12):1273–1277
Promberger R, Hermann M, Pallikunnel SJ, Seemann R, Meusel M, Ott J (2014) Quality of life after thyroid surgery in women with benign euthyroid goiter: influencing factors including Hashimoto’s thyroiditis. Am J Surg 207:974–979
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Thomas von Ahnen, Ulrich Wirth, Martin von Ahnen, Julia Kroenke, Peter Busch, Hans‑Martin Schardey and Stefan Schopf have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
von Ahnen, T., Wirth, U., von Ahnen, M. et al. Endoscopic cephalic access thyroid surgery (EndoCATS) using the retroauricular approach – a single centre retrospective data analysis. Surg Endosc 36, 117–125 (2022). https://doi.org/10.1007/s00464-020-08244-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08244-6