
Abstract
Background
The American health care system faces deficits in quality and quantity of surgeons. SAGES is a major stakeholder in surgical fellowship training and is responsible for defining the curriculum for the Advanced GI/MIS fellowship. SAGES leadership is actively adapting this curriculum.
Methods
The process of reform began in 2014 through a series of iterative meetings and discussions. A working group within the Resident and Fellow Training Committee reviewed case log data from 2012 to 2015. These data were used to propose new criteria designed to provide adequate exposure to core content. The working group also proposed using video assessment of an MIS case to provide objective assessment of competency.
Results
Case log data were available for 326 fellows with a total of 85,154 cases logged (median 227 per fellow). The working group proposed new criteria starting with minimum case volumes for five defined categories including foregut (20), bariatrics (25), inguinal hernia (10), ventral hernia (10), and solid organ/colon/thoracic (10). Fellows are expected to perform an additional 75 complex MIS cases of any category for a total of 150 required cases overall. The proposal also included a minimum volume of flexible endoscopy (50) and submission of an MIS foregut case for video assessment. The new criteria more clearly defined which surgeon roles count for major credit within individual categories. Fourteen fellowships volunteered to pilot these new criteria for the 2017–2018 academic year.
Conclusions
The new SAGES Advanced GI/MIS fellowship has been crafted to better define the core content that should be contained in these fellowships, while still allowing sufficient heterogeneity so that individual learners can tailor their training to specific areas of interest. The criteria also introduce innovative, evidence-based methods for assessing competency. Pending the results of the pilot program, SAGES will consider broad implementation of the new fellowship criteria.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Surgical training in the United States is considered among the best in the world; however, it faces deficits in both quality and quantity of surgeons needed to care for an aging population. From a quantity standpoint, the American Association of Medical Colleges (AAMC) projects a shortfall of approximately 20,000 to 30,000 surgeons by the year 2030 [1]. Perhaps more concerning is a perceived decrease in the quality of general surgery graduates. A survey of 91 surgical subspecialty fellowship program directors in 2013 reported the perception that 30% of recent general surgery graduates could not perform a laparoscopic cholecystectomy independently and 66% could not operate for 30 min independently during a major procedure [2]. The reasons for this observation are considered multi-factorial and include decreased work hours and increased technical skill required to master new surgical technology such as laparoscopy and robotics [3]. Trainees also face declining opportunities for operative autonomy related to sociopolitical mandates for quality, efficiency, and patient safety. All of these factors create challenges for general surgery programs to produce graduates who are prepared for independent practice [4,5,6]. In light of these issues, surgical education in the United States is in need of focused, thoughtful reform to meet the needs of the surgical trainee and the American public.
The governing bodies and major societies within surgical education have recognized these challenges to effective training, and have begun the process of reform. The Accreditation Council for Graduate Medical Education (ACGME) and Surgery Residency Review Committee (RRC) rolled out new case minimums for chief residents graduating in 2018. The new minimums place heavier emphasis on basic and complex laparoscopy, surgical critical care, breast surgery, endocrine surgery, and non-operative trauma. The minimums also require a wider breadth of abdominal and alimentary tract procedures [7].
The American Board of Surgery (ABS) has also recognized the importance of flexible endoscopy training for general surgery trainees and now requires graduates to complete a comprehensive curriculum in flexible endoscopy that includes measurement of performance beyond case numbers including passing the Fundamentals of Endoscopic Surgery (FES) exam [8]. In a statement on residency redesign released in April 2016, the ABS further identified the need to develop competency-based assessment tools rather than relying on case minimums alone as intraoperative training and individual trainee progress is variable. The Board went on to propose integrating Entrustable Professional Activities (EPAs) into surgical education to gauge progression though a curriculum and completion of core elements of training [9]. These new requirements seek to better prepare trainees for modern day surgical practice and to ensure that residents are able to independently and comprehensively manage the various disease entities encountered in general surgery practice. Although residency reform is clearly necessary, it is important to realize that modern surgical training does not end with residency as approximately 80% of general surgery graduates pursue additional training in the form of fellowships [10]. Thus, comprehensive surgical education reform must also include reform of fellowship training.
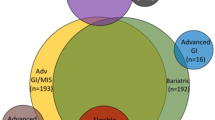
The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has a long history of leading in surgical education. The Minimally Invasive Surgery (MIS) Fellowship Council (MISFC) was created in 1997 to organize MIS fellowships, establish guidelines for training and begin to organize a match process for high-quality non-ACGME fellowships [11]. SAGES was an early stakeholder of the MISFC. With collaboration with additional gastrointestinal surgical societies, the MISFC ultimately evolved into the Fellowship Council (FC) with an even broader mission; the FC has grown substantially and now oversees 156 non-ACGME fellowship programs with 199 fellowship positions in Advanced Gastrointestinal (GI), flexible endoscopy, advanced GI/MIS, Bariatric, Hepatopancreatobiliary (HPB), colorectal, and thoracic surgery. The FC has organized a matching process for fellowship applicants, oversees accreditation of member programs, and maintains an electronic case log registry. Accreditation is determined based on site visits and a program’s adherence to core elements of fellowship education. Similar to the ABS efforts, the FC is creating EPAs as part of its Unified Standards Task Force for use within its various fellowship programs.
The specialty specific elements of fellowship education for FC fellowships are defined by the respective national societies associated with a given fellowship specialty focus. SAGES continues to be primarily responsible for defining the requirements for fellowships with Advanced GI/MIS and flexible endoscopy designations. The FC uses these requirements for the purpose of accrediting programs with these designations. For individual graduates, in 2014, SAGES began offering certificates to graduating fellows who fulfilled specified requirements for Advanced GI/MIS and/or flexible endoscopy fellowships. The number of FC approved Advanced GI/MIS and Flexible endoscopy fellowships has rapidly increased in the past 20 years and now includes 96 programs and 122 fellowship positions per year. In total, these fellowships represent 61% of FC fellowship programs, reinforcing SAGES role as a major stakeholder in fellowship training. The breakdown of FC fellowships is summarized in Table 1.
As required for a SAGES certificate, the current minimum case numbers for graduating Advanced GI/MIS fellows is 150 complex MIS cases (laparoscopic or robotic). Basic cases (diagnostic laparoscopy, cholecystectomy, and appendectomy), as defined by the ACGME resident case log system, are excluded as these are deemed more appropriate for resident-level learners. This framework has been in place for over a decade and allows for a large amount of heterogeneity in the experience of individual fellows. This heterogeneity enables trainees to tailor their fellow’s experience to their specific interests and is considered by many to be a strength of the FC accreditation process. Case logs of previous fellows in all FC programs are publically available on the FC website and are often used by applicants to base their rank order decisions as to their preferred fellowship program.
While tailoring the fellowship experience to a trainee’s anticipated needs post fellowship is desirable, it is also important that all graduating fellows receive appropriate exposure to core areas of advanced surgical training so they are well equipped to practice independently and meet the needs of the communities they will serve. To provide this base of core training while continuing to embrace the customizable experience of fellowships, curriculum reform is required.
Curriculum reform needs to focus not just on surgical technique, but on all aspects of surgical care using the most effective methods possible for expeditious and full patient recovery. While most SAGES fellowships provide training in the comprehensive care of upper GI disorders (including morbid obesity) and hernia management, to date, core training areas have not been well defined. This fact, coupled with national efforts to organize surgical training according to disease-based content areas, makes it apparent that better definitions of the core content of Advanced GI/MIS fellowships are needed. There is also a need to include objective measures of surgical competency, beyond case numbers, to ensure a trainee is ready for independent practice. With these principles in mind, SAGES is re-evaluating the curriculum recommendations for Advanced GI/MIS fellows to meet the challenges of the current educational and sociopolitical climate in surgical training.
Methods
Reform of the Advanced GI/MIS fellowship curricula was identified as a priority for SAGES at a presidential retreat in December 2014. During the same time, SAGES leaders were actively engaged in national discussions regarding competency-based surgical education, including the president and president-elect attending the Gastrointestinal Surgery Advisory Committee (GISAC) meeting at the ABS retreat in June 2015. Discussions about SAGES’s role in the evolving landscape of surgical education occurred at this meeting and continued to occur on a regular basis at the Executive Committee level. In January 2016, the SAGES leadership agreed to re-tool the former Resident Education Committee to become the Resident and Fellow Training (RAFT) Committee to emphasize this committee’s responsibility to provide oversight for SAGES fellowships. During the annual meeting in March 2016, the SAGES Board of Governors unanimously agreed to keep the Advanced GI/MIS name for SAGES surgical fellows and charged the RAFT Committee with developing a core curriculum for these fellowships that included updated case log requirements and objective evaluation criteria.
A working group from the RAFT Committee, consisting of leaders in surgical education, embarked on creating this new framework via iterative meetings and discussions. To inform the working group’s decision making, SAGES obtained de-identified case log data from the FC for cases performed by all Advanced/GI MIS fellows from 2012 to 2015. These cases were stratified into case types considered relevant to core content areas, and the working group used these data to help establish case log minimums for fellowship training. The working group also determined that new evaluation methods were needed to better ensure that graduating fellows were competent to perform core procedures. Accordingly, the group proposed inclusion of video assessment of an MIS foregut case as part of the new criteria as a measure of competency.
Results
FC case log data were available for 326 fellows with a total of 85,154 cases logged. Based on these data, the working group proposed minimum case volumes for five defined categories plus a minimum volume of flexible endoscopy. After discussions with the RAFT Committee, the working group further refined the requirements for these six criteria into a final proposal to present to SAGES leadership (Table 2). The criteria were designed to create a core experience that would be common to all Advanced GI/MIS fellowships while still allowing for and ensuring some degree of heterogeneity based on institutional specialties and the specific interests of individual fellows. An analysis of the 2012–2015 case log data showed that fellows would have met the proposed minimums for an individual category 60–86% of the time. Only 20% of fellows would have satisfied all six of the new criteria; however, 76% of fellows would have satisfied at least four of the six new criteria (Table 3). The working group determined that these new minimums represented balanced criteria that would be sufficient to provide adequate exposure to core content but not so onerous that fellows would struggle to consistently achieve them.
In addition to establishing the new minimum case volume criteria, the working group created a new set of expectations for fellows with respect to their role as surgeon. Whereas the previous criteria did not provide explicit requirements, the new criteria stipulate that the fellow must be the primary surgeon or teaching assistant (defined as leading a more junior trainee through a case) for all 75 defined category cases and at least 50 of the remaining 75 cases. A first assistant role is acceptable for credit on up to 25 non-defined category cases (Table 2).
Finally, the working group incorporated a video assessment requirement into the new criteria. Through discussions with the SAGES executive committee, the working group selected a laparoscopic fundoplication within the foregut core content area for video assessment. The criteria specify that the fellow should only submit a case performed as the primary surgeon. Faculty should supervise the case and may serve as a passive assistant, but if higher level faculty assistance or guidance is frequently required, the case would not be appropriate for submission. The entire unedited video, devoid of patient identifying information, will be provided to SAGES for review. Standardized, validated assessment methods for these videos are under development by a separate working group, as part of the SAGES Curriculum Task Force. The intention is that a performance threshold will be established and achievement of this level of performance will be required for satisfactory completion of the fellowship. Obviously, granting of a certificate of completion would include proof of successful completion of training at a FC accredited program and the approval signature of the Program Director.
These new criteria were approved by the RAFT Committee at the October 2016 SAGES Annual Meeting. The following month, the SAGES Board of Governors and the Executive Committee also voted to approve this new framework and endorsed the RAFT Committee’s plans to launch a pilot. SAGES informed the FC of these plans, and the FC Board and Executive Committee approved the pilot initiative. Advanced GI/MIS Fellowship Programs Directors who also have leadership roles in SAGES were invited to participate in the pilot. Fourteen programs (Table 4) volunteered to participate for the 2017–2018 academic year. The goals of the pilot are to determine the feasibility of meeting the new case log criteria and implementing the video assessment component. The RAFT Committee will closely monitor the outcomes of this pilot by evaluating the number of graduating fellows qualifying for a SAGES certificate, in order to determine if modifications are needed or if the new framework is suitable to submit to the FC for consideration as new criteria for program certification.
Discussion
Surgical education is undergoing considerable reform at multiple levels. While SAGES has had a tremendous impact on graduate medical education since its formation in 1981, the SAGES criteria for granting certificates to fellows are in need of modernization. Given other national efforts, including the creation of EPAs by both the ABS and the FC, it is apparent that SAGES fellowships needed to have their core content better defined. After much vetting and thoughtful consideration, the leadership of SAGES created the new criteria for Advanced GI/MIS Fellowships presented in this paper. These criteria were specifically designed to better define the core content that should be contained in all GI/MIS fellowship curricula, while continuing to allow sufficient heterogeneity such that individual trainees can tailor their training to specific areas of interest. Additionally, our goal was to introduce innovative methods for ensuring competency that go beyond didactic examinations and counting case numbers.
Critics of the new criteria may argue that the new case minimums are poorly constructed because only 20% of programs currently meet them. However, the intention of the new criteria is not to create a training requirement that all current programs can meet, but rather to thoughtfully create new criteria that will elevate the quality of fellowship education by carefully defining what SAGES considers core content in an Advanced GI/MIS Fellowship. Quality will be enhanced by defining a minimum core training experience because SAGES can build more robust curricula around these defined core content areas and also work toward verifying competency in these areas using more powerful assessment tools. The previous criteria of “150 complex MIS cases” could not adequately provide this structure. Reform by definition should represent a significant change to the status quo, and SAGES leadership feels that the new criteria will do this in a meaningful and valuable way such that graduating fellows will be better equipped to enter practice.
Additionally, the American Board of Medical Specialties (ABMS) recently announced the concept of Focused Practice Designations (FPDs) to “recognize areas of specific expertise of their diplomates and allow those physicians to concentrate their continuing certification efforts in the very area on which much of their professional practice is based.” The ABMS launched a pilot program for granting a FPD in Hospital Medicine. Pending the results of the pilot program, FPDs may be made available for other medical and surgical specialties [12]. With better defined core content areas, the new SAGES Advanced GI/MIS fellowship criteria may be helpful in providing a pathway for this type of recognition.
The working group identified areas common to Advanced GI/MIS fellowships according to three years of historical case log data. Foregut, bariatric, and inguinal and ventral hernias were deemed to be areas that were either well represented in current fellowships or thought to be sufficiently important to establish minimum case volumes. For example, during the three years of case logs available for review, 73–86% of current programs would have met the new criteria for foregut (20) and bariatric (25) cases, indicating that these would likely be obtainable requirements. Hernia operations had not been emphasized by the previous requirements; thus, lower requirements (10 inguinal and 10 ventral) were selected as reasonable targets, as 66–74% of programs would have met these new criteria. The rest of the core defined category cases (10) were allocated to a collection of other areas, including solid organ, hepatopancreatobiliary, colon, or thoracic, such that exposure to at least one or more of these other areas would be afforded.
For each of the 75 defined category cases, it was proposed that fellows should serve as primary surgeon or teaching assistant (TA). Other FC fellowship types had developed such criteria, but none had been previously proposed for Advanced GI/MIS fellowships [13]. The working group specifically thought that it was important to allow teaching cases to count toward these case volume requirements for several reasons. First, from the trainee’s perspective, fellows who have already developed significant expertise in a particular area may benefit from being allowed to serve as a teacher to a more junior trainee instead of simply performing an operation themselves. Second, since many fellowship programs are offered at institutions which also sponsor residency programs, allowing and even encouraging fellows to serve in a supervisory role mitigates competition for cases and optimizes educational benefit for both fellow and resident learners. For the 75 non-defined category cases, it was considered appropriate to require the fellow to serve as primary surgeon or TA in 50 of these cases and not simply as an assistant. Based on the data from 2012 to 2015, Advanced GI/MIS fellows graduated with a median of 227 cases; therefore, establishing these requirements for 125 cases should not be overly burdensome to fellows or fellowship programs.
SAGES also recognizes the increasing importance of flexible endoscopy in surgical training with many general surgeons performing large volumes of endoscopy in their daily practices [14, 15]. More importantly, within the realm of Advanced GI/MIS surgery, endoscopy is a common adjunct to foregut and bariatric operations in the preoperative, intraoperative, and postoperative settings [16, 17]. With this in mind, the working group felt that flexible endoscopy should be considered core content within the Advanced/GI MIS Fellowship, and they proposed a minimum volume of 50 diagnostic or therapeutic endoscopies be included in the new criteria. Although the previous criteria did not emphasize or even include minimum criteria for flexible endoscopy, the historical case log data revealed that 60% of fellows still logged more than 50 endoscopies. Based on these data, the working group felt it would be beneficial to add flexible endoscopy to the SAGES Advanced GI/MIS fellowship curriculum and that it should be feasible for programs to comply with this new requirement.
Although the new minimum case log and endoscopy requirements are designed to provide sufficient exposure to core content, they are not considered thresholds for achieving competency. The ABS has already recognized that simple case minimums may no longer be adequate to ensure readiness for independent practice, and a shift toward more sophisticated assessments of competency is the future of medical education in America and abroad [9, 18]. Video assessment of operative performance has been shown to correlate with patient outcomes, including complications and mortality [19]. However, national efforts to facilitate the use of this novel method of performance assessment are lacking. Recently, SAGES launched its Masters’ Program, which includes curricula designed to foster lifelong learning for surgeons in practice across seven core content areas [20]. Importantly, each pathway contains a video assessment of an anchoring procedure. Thus, SAGES is incorporating this innovative metric of competency into the new Advanced GI/MIS fellowship criteria by requiring video assessment of an MIS Foregut case. The video assessment is designed to provide a better metric of surgical competency than case numbers alone. Future evolution of the Advanced GI/MIS fellowship may involve expansion of video assessment to include all core content areas of the fellowship.
Although the video assessment component is innovative and important, it may pose some logistical challenges in the near future. An unedited video of a typical foregut procedure will be 1–4 h. Under the pilot program there will only be 14 videos to review, but when the new criteria are rolled out to all fellowships, this number will increase to at least 120 videos. Fortunately, methods are under development to use edited video, social media, and even crowd sourcing to generate meaningful assessments. Knowing that more and more trainees in medicine and surgery feel unprepared for practice upon graduation, SAGES feels that a real-world, competency-based assessment of technical skill is a necessary piece of comprehensive reform. Depending on the results of the pilot program, SAGES will implement appropriate measures to support the video review component of its curriculum.
Advanced GI/MIS fellowships must align with surgical education reform nationally. As MIS techniques become more advanced, the ability to achieve competency in all operations during five years of general surgery training will become nearly impossible. However, general surgery training will remain critical in producing graduates competent in the most common open, minimally invasive, and endoscopic gastrointestinal operations. These graduates should be prepared to enter practice and provide a breadth of surgical care to the vast majority of patients they encounter. Well-trained surgeons would also recognize complex care that is beyond the scope of their general surgery training and should appropriately refer to higher levels of care. It will largely fall to fellowships or mentorship in practice to provide disease-specific pathways for this complex surgical training. Advanced GI/MIS training will provide surgeons with an attractive skill set to care for a variety of common disease processes with complex operations that are in demand in a variety of practice settings.
SAGES also recognizes that these reforms represent a first step in what is likely to be an ongoing process. Surgical and educational techniques continue to evolve, and fellowship training will need to continue to grow and adapt. One topic that is not addressed in the new criteria is the need for the Advanced GI/MIS surgeon to also be competent in complex open techniques. Currently, any open procedure performed during the Advanced GI/MIS fellowship does not count for major credit. However, some cases are too complex to complete with MIS modalities and fellows may benefit from exposure to these cases to round out their training. This may be especially true for patients undergoing revisional procedures following multiple previous operations. Similarly, an open approach may be optimal for some inguinal and ventral hernias.
As the practice of surgery evolves, alternate training avenues may also prove necessary. SAGES is actively working with the Americas Hernia Society (AHS) to create criteria for a new FC Hernia Fellowship category. Some of these criteria may need to be adapted into the Advanced GI/MIS fellowships when they become available. Additionally, SAGES has been actively participating for several years in an effort initially led by the Society for Surgery of the Alimentary Tract (SSAT) to explore a new fellowship in Complex GI Surgery. The focus of that fellowship is the elective and emergent management of GI diseases across the entire GI tract. This work is now being conducted by an intersociety working group and an initial pilot is proposed by the SSAT. Pending the pilot results, further modifications to the Advanced GI/MIS fellowship criteria may be warranted.
Conclusions
The new criteria for the certifying Advanced GI/MIS Fellows has been thoughtfully crafted to modernize fellowships by defining core content areas and introducing novel methods for competency assessment. The redesign is being tested through a pilot program this year. Pending results of the pilot program, the new criteria may serve as a model for educational reform across other medical and surgical disciplines.
References
Dall T, Chakrabarti R, Iacobucci W, Hansari A, West T (2017) 2017 Update: the complexities of physician supply and demand: projections from 2015 to 2030. Association of American Medical Colleges, Washington
Mattar SG, Alseidi AA, Jones DB et al (2013) General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg 258(3):440–449
Park A, Witzke D, Donnelly M (2002) Ongoing deficits in resident training for minimally invasive surgery. J Gastrointest Surg 6(3):501–507 (discussion 507–509)
Lewis FR, Klingensmith ME (2012) Issues in general surgery residency training-2012. Ann Surg 256(4):553–559
Scally CP, Sandhu G, Magas C, Gauger PG, Minter RM (2015) Investigating the Impact of the 2011 ACGME Resident Duty Hour Regulations on Surgical Residency Programs: The Program Director Perspective. J Am Coll Surg 221(4):883–889e881
Bell RH Jr, Banker MB, Rhodes RS, Biester TW, Lewis FR (2007) Graduate medical education in surgery in the United States. Surg Clin North Am 87(4):811–823.
ACGME (2017) Defined category minimum numbers: general surgery effective for program graduates beginning academic year 2017–2018, Accreditation Council for Graduate Medical Education, Chicago
ABS Flexible endoscopy curriculum for general surgery residents (2014)
ABS Statement Regarding Residency Redesign (2016). https://www.absurgery.org/default.jsp?news_resredesign0416. Accessed 25 Apr 2016
Borman KR, Vick LR, Biester TW, Mitchell ME (2008) Changing demographics of residents choosing fellowships: longterm data from the American Board of Surgery. J Am Coll Surg 206(5):782–788 (discussion 788–789)
Swanstrom LL, Park A, Arregui M, Franklin M, Smith CD, Blaney C (2006) Bringing order to the chaos: developing a matching process for minimally invasive and gastrointestinal postgraduate fellowships. Ann Surg 243(4):431–435
American Board of Medical Specialties Announces New, Focused Practice Designation (2017). http://www.abms.org/media/136465/abms-announces-new-focused-practice-designation.pdf. Accessed 14 Mar 2017
Fellowship Council Accreditation Guidelines and Definitions (2016) https://fellowshipcouncil.org/wp-content/uploads/2012/02/FC-Accreditation-Guidelines-and-Definitions-4-2016-Web.pdf. Accessed 6 Sept 2017
Pearl J, Fellinger E, Dunkin B et al (2016) Guidelines for privileging and credentialing physicians in gastrointestinal endoscopy. Surg Endosc 30(8):3184–3190
Zuckerman R, Doty B, Bark K, Heneghan S (2007) Rural versus non-rural differences in surgeon performed endoscopy: results of a national survey. Am Surg 73(9):903–905
De Palma GD, Forestieri P (2014) Role of endoscopy in the bariatric surgery of patients. World J Gastroenterol 20(24):7777–7784
Wolter S, Dupree A, Miro J et al (2017) Upper gastrointestinal endoscopy prior to bariatric surgery-mandatory or expendable? An analysis of 801 cases. Obes Surg 27(8):1938–1943
Safavi A, Lai S, Butterworth S, Hameed M, Schiller D, Skarsgard E (2012) Does operative experience during residency correlate with reported competency of recent general surgery graduates? Can J Surg 55(4):S171–S177
Birkmeyer JD, Finks JF, O’Reilly A et al (2013) Surgical skill and complication rates after bariatric surgery. N Engl J Med 369(15):1434–1442
Jones DB, Stefanidis D, Korndorffer JR Jr et al (2017) SAGES university MASTERS program: a structured curriculum for deliberate, lifelong learning. Surg Endosc 31(8):3061–3071
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Joshua J. Weis, Matthew Goldblatt, Aurora Pryor, Brian J. Dunkin, L. Michael Brunt, Daniel B. Jones, and Daniel J. Scott have nothing to disclose.
Additional information
Submitted for presentation at the SAGES Annual Meeting, April 10–14, 2018, Seattle, WA.
Rights and permissions
About this article

Cite this article
Weis, J.J., Goldblatt, M., Pryor, A. et al. SAGES’s advanced GI/MIS fellowship curriculum pilot project. Surg Endosc 32, 2613–2619 (2018). https://doi.org/10.1007/s00464-018-6020-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6020-8