
Abstract
Background
Obesity has been considered a relative contraindication to peritoneal dialysis (PD). Surprisingly, PD catheter dysfunction rates and longevity have not been studied in the growing obese ESRD population. The aim of this study was to determine the effect of patient weight on PD catheter survival in the three insertion technique categories of advanced laparoscopy (AL), basic laparoscopy (BL), and open.
Methods
We examine retrospectively collected data on 231 consecutive PD catheter insertions at the NorthShore University HealthSystem between 2004 and 2014. Three cohorts were created based on the catheter insertion technique: open, BL using selective adhesiolysis, and AL using rectus sheath tunnel, selective omentopexy, and adhesiolysis. Primary outcomes included catheter dysfunction and catheter dysfunction-free survival for each cohort by BMI: normal weight (18.5–24.9), overweight (25–29.9), obese (≥30). Nominal variables were compared using Chi-square test, continuous variables using ANOVA or Kruskal–Wallis tests, and catheter survival was assessed using the Kaplan–Meier method with log-rank test. Statistical significance was established at 0.05.
Results
For the three BMI categories, there were no statistically significant differences in patient demographics. There were no statistically significant differences in catheter dysfunction or peri-operative complications by BMI category among all patients. This was also true in the AL cohort. Among all patients, similar 2-year dysfunction-free catheter survival was noted for normal weight, overweight, and obese patients (log-rank p = 0.79). This was also true across all insertion techniques: open (log-rank p = 0.87), BL (log-rank p = 0.41), AL (log-rank p = 0.43). In the obese cohort, the 2-year dysfunction-free catheter survival was 91.1% in AL, 83.5% in BL, and 65.7% in open (log-rank p = 0.58).
Conclusion
Obesity does not increase complications or shorten dysfunction-free PD catheter survival regardless of the operative technique used. Obesity should not be considered as a relative contraindication to PD catheter placement as it confers similar technique success to normal- and overweight individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Obesity in the adult United States population has grown to epidemic proportions, with a prevalence estimated by CDC to be 36.5% in 2011–2014 [1]. Patients with end-stage renal disease (ESRD) are equally affected by the obesity problem. Between 1995 and 2002, obesity increased by 33% in the incident ESRD patients initiating dialysis, with an increase in mean BMI from 25.7 to 27.4 during this time period [2]. This trend continues, with reported mean BMI of 28.9 in the incident ESRD patients in 2007–2009 [3]. While obesity is a well-known risk factor for end-stage renal disease (ESRD) [4], historically it has been considered as a relative contraindication to peritoneal dialysis (PD) [5]. Therefore, obese patients are less likely to be offered and to initiate peritoneal dialysis (PD) as a modality in the United States [6]. This has been mainly due to early data showing that obese individuals suffer inferior PD outcomes, including increased risk of mortality, inadequate solute clearance, higher risk of infectious complications, as well as early technique failure [5, 7,8,9]. Over the years, many of these notions have been challenged. We now know that obesity does not seem to confer an increased mortality risk in patients on PD, and in fact may provide a survival advantage for this patient population [10,11,12,13]. Furthermore, the findings of inadequate solute clearance in the obese were based mostly on mathematical models and current research shows that in fact it is possible to achieve adequate solute clearance in obese PD patients with higher dwell volumes [14, 15]. Data remain mixed in terms of infectious complications in the obese PD population [9, 16, 17]. However, research is lacking in the area of PD technique failure and PD longevity in the obese population. This is especially important with the recent introduction of advanced laparoscopic insertion techniques [18].
The durability of the PD catheter is the key factor in the long-term success of PD, and is contingent on the PD catheter insertion technique. Mechanical PD catheter complications are the main reasons for PD failure and subsequent transfer to hemodialysis accounting for 19.6% of failures [19, 20]. Advanced laparoscopic (AL) insertion technique, which utilizes rectus sheath tunnel, selective omentopexy, and selective adhesiolysis, has been shown to confer lower mechanical PD catheter dysfunction rates and improved dysfunction-free catheter survival in the general PD patient population when compared to open and basic laparoscopy (BL) [18, 21, 22].
Given the growing population of obese ESRD patients and the widely established benefits of PD over hemodialysis (HD), including preservation of residual renal function [23, 24], improved autonomy and quality of life [25, 26], a slight survival advantage within the first 2 years of dialysis initiation [27, 28], and lower dialysis costs [3, 29,30,31], research is urgently needed to define the effect of obesity on PD technique failure and PD longevity outcomes. Therefore, we sought to investigate the impact of patient weight on PD outcomes such as PD catheter dysfunction rates, dysfunction-free catheter survival, and peri-operative complications among patients whose PD catheters were inserted using open, basic laparoscopic, and advanced laparoscopic insertion techniques.
Patients and methods
Study design
The study was approved by the NorthShore University HealthSystem Institutional Review Board. Retrospective database of eligible patients undergoing open, basic laparoscopic, and advanced laparoscopic peritoneal dialysis catheter insertion was queried. All the operations were performed by five high volume minimally invasive surgeons and one vascular surgeon performing routine PD catheter insertions at the four hospitals comprising NorthShore University HealthSystem.
Patients
Our retrospective PD database includes 235 consecutive PD catheter insertions performed during a transition period from open to basic laparoscopic to advanced laparoscopic insertion procedures performed between February 2004 and November 2014. Inclusion criteria included evidence of post-insertion catheter use and adequate post-operative follow-up. Four (4) patients were excluded from the analysis as their BMI was <18.5. Variables gathered included patient demographics, pre-operative data such as comorbidities, reason of renal replacement therapy, prior renal replacement therapy, prior abdominal operations, intraoperative data such as details of operative technique, complications, additional operative interventions, and post-operative data such as post-operative complications, catheter dysfunction (inflow/outflow obstruction, migration, peri-catheter leak), need for any reason for catheter revision/removal, and length of follow-up.
Outcomes and definitions
Primary outcomes measured included mechanical PD catheter dysfunction rates and PD catheter dysfunction-free survival and overall PD catheter survival. Mechanical PD catheter dysfunction was defined as the need for revisionary surgery or catheter removal due to inflow/outflow obstruction to dialysate flow, catheter tip migration, or peri-catheter leak. Dysfunction-free catheter survival was defined as total length of time of primary catheter use from the time of insertion to either revision or removal due to mechanical catheter dysfunction only. Analysis was censored (see “Statistical analysis” for definition) on all other reasons for catheter removal, such as wound infection, peritonitis, patient preference for HD, clinical PD failure (inadequate dialysis), renal transplant, return of renal function, as well as loss to follow-up and death. Dysfunction-and-infection-free catheter survival was defined as total length of time of primary catheter use from the time of insertion to either revision due to mechanical dysfunction or removal due to mechanical catheter dysfunction or infectious complication. Analysis was censored on patient preference for HD, clinical PD failure, renal transplant, return of renal function, as well as loss to follow-up and death. Overall PD catheter survival was defined as total length of time of primary catheter use from the time of insertion to either revision or removal due to mechanical dysfunction, infectious complications, patient preference for HD and clinical PD failure, censored only on catheter removal due to renal transplant, return of renal function, loss of follow-up, and death. Secondary outcomes included peri-operative complications. Intraoperative complications included bleeding and bowel injury. Post-operative complications included (1) infectious complications: peritonitis (early peritonitis within 2 weeks of operation, late peritonitis 2 weeks or more following surgery), superficial wound infections, or peri-catheter abscess within 1 month of operation, (2) ileus (lack of return of bowel function within 3 days of operation), (4) urinary retention, (5) incisional hernia.
Study groups
Patient cohorts were defined based on BMI categories as per WHO classification of normal weight (18.5–24.9), overweight (25–29.9), and obese (≥30). Strict operative procedure definitions were utilized to further subdivide patients into operative cohorts of open, basic laparoscopy (BL), and advanced laparoscopy (AL). Procedures utilizing a minilaparotomy incision were categorized as open. BL was defined as the use of laparoscopy to visualize catheter placement in the pelvis, including adhesiolysis when performed. AL was defined as use of laparoscopy with performance of rectus sheath tunnel, selective omentopexy, and selective adhesiolysis. Please refer to our previous publication for detailed description of these surgical procedures [18].
Statistical analysis
Demographics, operative characteristics, operative technique, peri- and post-operative complications, and mechanical PD catheter dysfunction rates were compared by BMI category. Categorical variables were compared using Chi-square test. Continuous variables were compared using analysis of variance or Kruskal–Wallis test with post hoc comparisons made using Tukey’s test or Dunn test. Kaplan–Meier catheter dysfunction-free survival curves, dysfunction-and-infection-free survival curves, and overall catheter survival curves were constructed based on BMI and operative technique groups and compared using log-rank test with post hoc comparisons made using Tukey’s test. Survival time endpoint was reached either when the event of interest (or censoring event) occurred or when the follow-up time ended. All censored observations contributed to the total number at risk up to the time that they ceased to be followed. Statistical significance was established at p < 0.05. All statistical analyses were conducted using SAS version 9.3 (SAS Institute Inc, Cary, NC).
Results
Study design and patient characteristics
The study cohort comprised 235 consecutive PD catheter insertions from February 2004 to November 2014. Four patients were excluded from the analysis as their BMI was <18.5, with a total of 231 patients included in the analysis. We encountered no mortalities within 30 days of the operation. None of the laparoscopic procedures were converted to open. Patient demographics are presented in Table 1. Overall mean age of the entire cohort was 63.5 ± 16.7. For the three BMI categories of normal weight, overweight, and obese, the average age of the patients was 65.4 (±19.7), 64.5 (±15.0), and 60.4 (±15.0), respectively. Males comprised 60.6% of the entire cohort. The percent of male gender in each BMI cohort was 55.6, 65.2, and 60.0%, respectively. There was no statistical difference between the age, gender, post-operative follow-up, prior abdominal surgery, prior peritoneal dialysis or hemodialysis, insertion technique, or ASA class between groups.
Operative variables in the advanced laparoscopy cohort
In the advanced laparoscopy cohort, utilization of selective omentopexy was significantly higher in the obese population when compared to both normal weight and overweight individuals (76.7% vs 48.1% vs 38.2%, respectively, p = 0.01, Table 2). There were no statistically significant differences in the utilization of selective adhesiolysis or the operative time among the three BMI cohorts. Although all simultaneous umbilical hernia repairs occurred in the overweight (5) and obese (5) patients, this finding was not statistically significant (p = 0.09).
Peri-operative complications
In the analysis of the entire study cohort, we encountered low rates of intra- and post-operative complications (Table 3). Three (3) patients experienced intraoperative complications which included a bleed, enterotomy, and serosal tear. These intraoperative complications were controlled at the time and did not lead to long-term sequelae. None of these complications occurred in the obese cohort. Early infectious complications included exit site infections (occurring within 1 month of operation), diagnosed in 3 patients and early peritonitis (occurring within 2 weeks of the operation) diagnosed in 3 patients. There were no statistically significant differences in the above post-operative infectious complications between the three BMI cohorts (Table 3). Two (2) patients developed incisional hernias, both in the overweight cohort and both following open operations. There were no incisional hernias noted in the obese cohort. Post-operative complications did not statistically differ among the three BMI cohorts. Late peritonitis (more than 2 weeks following the operation) was diagnosed in 60 patients among the entire cohort (Table 3). There was no statistically significant difference in late peritonitis among the three BMI cohorts. When looking only at the advanced laparoscopy cohort, there were no statistically significant differences in intraoperative, post-operative, and late complications by BMI category (Table 4).
Catheter dysfunction rates
Catheter dysfunction, revision, and removal rates by BMI category are presented in Table 5. Among all patients, we found nine mechanical catheter dysfunctions in the normal weight cohort, 14 in the overweight cohort, and 12 in the obese cohort. There were no statistically significant differences in PD catheter dysfunction rates among the three BMI cohorts when all dysfunctions were considered together, or separated by type of mechanical catheter dysfunction (inflow obstruction, outflow obstruction, catheter migration, or peri-catheter leak). The rates of catheter revision due to mechanical dysfunction were also similar among the three BMI cohorts. PD catheter revisions due to mechanical dysfunctions occurred in 9 normal weight individuals, in 11 overweight individuals, and in 10 obese individuals. Time to revision did not differ among the BMI groups. There were no differences between the three BMI cohorts in PD catheter removal due to: (1) mechanical dysfunction only, (2) mechanical dysfunction and infectious complications, and (3) all causes (inclusive of patient preference, PD failure, renal transplant, etc).
Similarly, the rates of PD catheter dysfunction, revision, and removal were not statistically different between the three BMI cohorts among patients in the advanced laparoscopic insertion technique cohort (Table 6).
Long-term results and peritoneal dialysis longevity by BMI
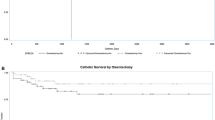
Among all patients in the study, the 2-year dysfunction-free catheter survival was similar between the normal weight, overweight, and obese individuals (84.1% vs 86.7% vs 80.3%, respectively, log-rank p = 0.79) (Table 7, Fig. 1). This was also true when 2-year dysfunction-free catheter survival was assessed by the same BMI stratification within each operative technique cohort: open (85.1% vs 79.7% vs 65.7%, log-rank p = 0.87), BL (58.6% vs 87.3% vs 83.5%, log-rank p = 0.41), AL (100% vs 92.0% vs 91.1%, log-rank p = 0.43) (Table 7, Supplemental Figure). In the obese cohort, all three insertion techniques resulted in similar 2-year dysfunction-free catheter survival (AL = 91.1% vs BL = 83.5% vs open = 65.7%, log-rank p = 0.58) (Table 7).

Kaplan–Meier dysfunction-free catheter survival curves for all patients by BMI category (log-rank p = 0.79)
Among all patients in the study, the 2-year dysfunction-and-infection-free catheter survival was similar between the normal weight, overweight, and obese individuals (67.1% vs 75.4% vs 59.3%, respectively, log-rank p = 0.34) (Table 8). This was also true when 2-year dysfunction-and-infection-free catheter survival was assessed within each operative technique cohort: open (73.8% vs 69.1% vs 54.9%, log-rank p = 0.79), BL (48.0% vs 76.5% vs 43.8%, log-rank p = 0.15), AL (71.9% vs 81.4% vs 82.6%, log-rank p = 0.72) (Table 8). In the obese cohort, all three insertion techniques resulted in similar 2-year dysfunction-and-infection-free catheter survival (AL = 82.6% vs BL = 43.8% vs open = 54.9%, log-rank p = 0.11) (Table 8).
Among all patients in the study, the 2-year overall catheter survival was similar between the normal weight, overweight, and obese individuals (34.7% vs 49.7% vs 37.8%; log-rank p = 0.09) (Table 9). In obese patients, overall survival was different between operative techniques (log-rank p = 0.02). We found significantly improved overall PD catheter survival in the obese patients following AL insertion as compared to BL insertion (62.0% vs 16.3%; log-rank p = 0.02), but not when compared to open insertion (62.0% vs 43.7%; log-rank p = 0.24).
Discussion
We found that outcomes following peritoneal dialysis catheter insertion are not adversely affected by obesity in our entire study population, regardless of the operative technique. Obese subjects were as likely to benefit from long-term PD catheter function as their normal weight and overweight counterparts. This was true when considering mechanical PD catheter dysfunction alone, as well as infectious complications such as early exit site infection and early and late peritonitis. Addition of patient preference and clinical PD failure to the analysis did not change the above conclusions. This finding held true not only in our full study cohort, but also in each of the three common operative insertion technique cohorts.
Existing research on the topic of obesity and PD technique survival is scant and most published studies focus on patient survival as their primary outcome, with less emphasis on technique survival. A multicenter prospective study published in 2002 studied patient survival and PD technique survival in 208 patients divided into two BMI categories, greater than 27 and between 20 and 27. The authors showed that PD technique survival, defined as switch to hemodialysis, was similar among the two groups at 2-year follow-up. Although the study results are compelling, the arbitrary BMI cutoff limits our ability to make broader conclusions. Prasad et al. showed in their retrospective cohort of 328 patients that death-censored PD technique survival was similar among obese, overweight, and normal weight patients in India [32]. Conversely, Snyder et al. reported that overweight and obese patients in a retrospective cohort experienced higher rates of switch to HD as compared to normal weight individuals [6]. Similarly, a retrospective study published by Unal et al. showed that BMI was significantly associated with PD technique failure in 392 PD patients being treated with PD between 1995 and 2013 [33]. The definition of technique failure used in the above studies is very broad. Furthermore, the authors do not specify the surgical technique used for catheter placement.
The only available study assessing BMI effect on PD catheter dysfunction rates (among other patient-specific variables) is a study by Singh et al. [34]. The authors looked at outcomes specifically related to PD catheter failure, defined as catheter removal due to catheter-related problems. The authors determined that BMI did not affect PD catheter survival. In our study, we go a step further, looking at PD catheter-related outcomes of mechanical PD catheter dysfunction, infectious complications, and patient-related factors as reasons for technique failure. We also further subdivide patients into cohorts based on the PD catheter insertion method, which we believe is important given the lack of standardized surgical insertion technique and our recently published findings showing superiority of advanced laparoscopic PD catheter insertion on PD catheter longevity [18].
Additionally, obesity is believed to be a risk factor for infectious complications in patients on PD, but the literature on this topic is similarly conflicting. Prasad et al. showed that obese individuals had a 3.4-fold greater risk of peritonitis when compared with normal weight individuals after 22 month follow-up [32]. This study did not use WHO BMI category definitions, and reported obesity as BMI > 25, which makes it difficult to draw broader conclusions. Additionally, despite the differences in peritonitis rates by BMI, this study showed no difference in technique failure (defined as switch to HD) by BMI. The ANZDATA registry study by McDonald et al. also showed increased risk of peritonitis in the obese PD patients, with increasing BMI associated with earlier and more frequent peritonitis episodes [9]. However, more recent studies show no increased infectious complications in obese patients. Hsieh et al. reported no significant correlation between BMI and peritonitis in 391 PD patients [35]. Nessim et al. also found no association between exit site infections or peritonitis and BMI in 938 patients, with the exception of coagulase-negative Staphylococcus peritonitis which appeared more common in the obese [17]. In our study we show no differences in infectious complications, including exit site infections, early and late peritonitis. We purposefully chose the 2-week mark to separate peritonitis into early and late, as the former is likely related to the peri-operative technique, while the latter is likely related to patient characteristics. We also show that PD catheter survival is similar among BMI categories when accounting for catheter removals due to infectious complications.
There are no studies to date that specifically analyze the longevity of PD catheter function in obese patients following the relatively recently introduced insertion techniques utilizing advanced laparoscopy with the use of rectus sheath tunnel and selective omentopexy (performed only when the omentum was large and extended into the pelvis). We show that in the advanced laparoscopic insertion cohort, the use of omentopexy is significantly higher in the obese, which is not surprising since this group of patients has increased intra-abdominal adiposity. In addition, the AL cohort had significantly improved overall PD catheter survival in the obese patients compared to BL (no omentopexy). We observed a trend toward higher 2-year dysfunction-free and dysfunction-and-infection-free catheter survival percentage in the obese cohort using AL compared to open. However, this did not achieve statistical significance. Subsequent studies validating our findings on advanced laparoscopic insertion technique and related rates of mechanical and infectious complications, as well as PD catheter survival in the obese population is warranted.
The limitations of this study are inherent to its retrospective nature. The PD catheter insertion techniques were utilized in sequence as our practice evolved over time, with open procedures utilized early (2004–2008), followed by basic laparoscopy (2005–2012), and then advanced laparoscopy (2008–present). The evolving surgeon experience has the potential for introduction of bias, which would be difficult to control short of a randomized controlled trial. Related to this is the differential length of follow-up, which has the potential of increasing the chance of identifying catheter dysfunction and late peritonitis in the open group. However, we have accounted for this differential follow-up in our statistical methodology limiting outcomes to 2-year catheter survival.
Given that obesity has been long considered a relative contraindication to PD, our findings are important, providing evidence that PD in obese patients is safe and durable. Snyder et al. retrospectively reviewed a cohort of 418,021 Medicare patients initiating dialysis between 1995 and 2000, and showed that obese patients were 13% less likely to initiate peritoneal dialysis when compared to patients with normal BMI, despite having improved survival [6]. The authors speculated that these results could potentially be due to narrower treatment options offered to this patient population.
With the heightened risk of ESRD in the obese and the increasing prevalence of obesity in the ESRD patient population, many patients could potentially not be offered this important mode of renal replacement therapy. However, our findings suggest that obesity should not be a deterrent to the initiation of PD.
References
Adult Obesity Facts | Overweight & Obesity | CDC. https://www.cdc.gov/obesity/data/adult.html. Accessed 21 Mar 2017
Kramer HJ, Saranathan A, Luke A, Durazo-Arvizu RA, Guichan C, Hou S, Cooper R (2006) Increasing body mass index and obesity in the incident ESRD population. J Am Soc Nephrol JASN 17:1453–1459. doi:10.1681/ASN.2005111241
United States Renal Data System (2015) USRDS annual data report: epidemiology of kidney disease in the United States
Hsu C, McCulloch CE, Iribarren C, Darbinian J, Go AS (2006) Body mass index and risk for end-stage renal disease. Ann Intern Med 144:21–28
(1997) NKF-DOQI clinical practice guidelines for peritoneal dialysis adequacy. National Kidney Foundation. Am J Kidney Dis 30:S67–136
Snyder JJ, Foley RN, Gilbertson DT, Vonesh EF, Collins AJ (2003) Body size and outcomes on peritoneal dialysis in the United States. Kidney Int 64:1838–1844. doi:10.1046/j.1523-1755.2003.00287.x
Nolph KD, Jensen RA, Khanna R, Twardowski ZJ (1994) Weight limitations for weekly urea clearances using various exchange volumes in continuous ambulatory peritoneal dialysis. Perit Dial Int J Int Soc Perit Dial 14:261–264
McDonald SP, Collins JF, Johnson DW (2003) Obesity is associated with worse peritoneal dialysis outcomes in the Australia and New Zealand patient populations. J Am Soc Nephrol JASN 14:2894–2901
McDonald SP, Collins JF, Rumpsfeld M, Johnson DW (2004) Obesity is a risk factor for peritonitis in the Australian and New Zealand peritoneal dialysis patient populations. Perit Dial Int J Int Soc Perit Dial 24:340–346
Aslam N, Bernardini J, Fried L, Piraino B (2002) Large body mass index does not predict short-term survival in peritoneal dialysis patients. Perit Dial Int J Int Soc Perit Dial 22:191–196
Johnson DW, Herzig KA, Purdie DM, Chang W, Brown AM, Rigby RJ, Campbell SB, Nicol DL, Hawley CM (2000) Is obesity a favorable prognostic factor in peritoneal dialysis patients? Perit Dial Int J Int Soc Perit Dial 20:715–721
Badve SV, Paul SK, Klein K, Clayton PA, Hawley CM, Brown FG, Boudville N, Polkinghorne KR, McDonald SP, Johnson DW (2014) The association between body mass index and mortality in incident dialysis patients. PLoS ONE 9:e114897. doi:10.1371/journal.pone.0114897
Ladhani M, Craig JC, Irving M, Clayton PA, Wong G (2016) Obesity and the risk of cardiovascular and all-cause mortality in chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant. doi:10.1093/ndt/gfw075
Shibagaki Y, Faber MD, Divine G, Shetty A (2002) Feasibility of adequate solute clearance in obese patients on peritoneal dialysis: a cross-sectional study. Am J Kidney Dis 40:1295–1300. doi:10.1053/ajkd.2002.36904
Boyle SM, Li Y, Wilson FP, Glickman JD, Feldman HI (2017) Association of alternative approaches to normalizing peritoneal dialysis clearance with mortality and technique failure: a retrospective analysis using the United States renal data system-dialysis morbidity and mortality study, wave 2. Perit Dial Int J Int Soc Perit Dial 37:85–93. doi:10.3747/pdi.2015.00227
Piraino B, Bernardini J, Centa PK, Johnston JR, Sorkin MI (1991) The effect of body weight on CAPD related infections and catheter loss. Perit Dial Int J Int Soc Perit Dial 11:64–68
Nessim SJ, Komenda P, Rigatto C, Verrelli M, Sood MM (2013) Frequency and microbiology of peritonitis and exit-site infection among obese peritoneal dialysis patients. Perit Dial Int J Int Soc Perit Dial 33:167–174. doi:10.3747/pdi.2011.00244
Krezalek MA, Bonamici N, Lapin B, Carbray J, Velasco J, Denham W, Linn J, Ujiki M, Haggerty SP (2016) Laparoscopic peritoneal dialysis catheter insertion using rectus sheath tunnel and selective omentopexy significantly reduces catheter dysfunction and increases peritoneal dialysis longevity. Surgery 160:924–935. doi:10.1016/j.surg.2016.06.005
Shahbazi N, McCormick BB (2011) Peritoneal dialysis catheter insertion strategies and maintenance of catheter function. Semin Nephrol 31:138–151. doi:10.1016/j.semnephrol.2011.01.003
Mujais S, Story K (2006) Peritoneal dialysis in the US: evaluation of outcomes in contemporary cohorts. Kidney Int. doi:10.1038/sj.ki.5001912
Attaluri V, Lebeis C, Brethauer S, Rosenblatt S (2010) Advanced laparoscopic techniques significantly improve function of peritoneal dialysis catheters. J Am Coll Surg 211:699–704. doi:10.1016/j.jamcollsurg.2010.08.010
Crabtree JH, Burchette RJ (2009) Effective use of laparoscopy for long-term peritoneal dialysis access. Am J Surg 198:135–141. doi:10.1016/j.amjsurg.2008.10.019
Moist LM, Port FK, Orzol SM, Young EW, Ostbye T, Wolfe RA, Hulbert-Shearon T, Jones CA, Bloembergen WE (2000) Predictors of loss of residual renal function among new dialysis patients. J Am Soc Nephrol JASN 11:556–564
Tam P (2009) Peritoneal dialysis and preservation of residual renal function. Perit Dial Int J Int Soc Perit Dial 29(Suppl 2):S108–S110
Rubin HR, Fink NE, Plantinga LC, Sadler JH, Kliger AS, Powe NR (2004) Patient ratings of dialysis care with peritoneal dialysis vs hemodialysis. JAMA 291:697–703. doi:10.1001/jama.291.6.697
Juergensen E, Wuerth D, Finkelstein SH, Juergensen PH, Bekui A, Finkelstein FO (2006) Hemodialysis and peritoneal dialysis: patients’ assessment of their satisfaction with therapy and the impact of the therapy on their lives. Clin J Am Soc Nephrol CJASN 1:1191–1196. doi:10.2215/CJN.01220406
Fenton SS, Schaubel DE, Desmeules M, Morrison HI, Mao Y, Copleston P, Jeffery JR, Kjellstrand CM (1997) Hemodialysis versus peritoneal dialysis: a comparison of adjusted mortality rates. Am J Kidney Dis 30:334–342
Heaf JG, Løkkegaard H, Madsen M (2002) Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant 17:112–117
Davis WT, Dageforde LA, Moore DE (2014) Laparoscopic versus open peritoneal dialysis catheter insertion cost analysis. J Surg Res 187:182–188. doi:10.1016/j.jss.2013.09.041
Klarenbach SW, Tonelli M, Chui B, Manns BJ (2014) Economic evaluation of dialysis therapies. Nat Rev Nephrol 10:644–652. doi:10.1038/nrneph.2014.145
Shih Y-CT, Guo A, Just PM, Mujais S (2005) Impact of initial dialysis modality and modality switches on Medicare expenditures of end-stage renal disease patients. Kidney Int 68:319–329. doi:10.1111/j.1523-1755.2005.00413.x
Prasad N, Sinha A, Gupta A, Sharma RK, Bhadauria D, Chandra A, Prasad KN, Kaul A (2014) Effect of body mass index on outcomes of peritoneal dialysis patients in India. Perit Dial Int J Int Soc Perit Dial 34:399–408. doi:10.3747/pdi.2013.00056
Unal A, Hayri Sipahioglu M, Kocyigit I, Elmali F, Tokgoz B, Oymak O (2014) Does body mass index affect survival and technique failure in patients undergoing peritoneal dialysis? Pak J Med Sci 30:41–44. doi:10.12669/pjms.301.3807
Singh N, Davidson I, Minhajuddin A, Gieser S, Nurenberg M, Saxena R (2010) Risk factors associated with peritoneal dialysis catheter survival: a 9-year single-center study in 315 patients. J Vasc Access 11:316–322
Hsieh Y-P, Chang C-C, Wen Y-K, Chiu P-F, Yang Y (2014) Predictors of peritonitis and the impact of peritonitis on clinical outcomes of continuous ambulatory peritoneal dialysis patients in Taiwan–10 years’ experience in a single center. Perit Dial Int J Int Soc Perit Dial 34:85–94. doi:10.3747/pdi.2012.00075
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Stephen P. Haggerty has following disclosures: consultant and speaker for Covidien and Medtronic Since 2013, Honorarium from Bard 2013. Monika Krezalek, Nicolas Bonamici, Brittany Lapin, JoAnn Carbray, Jose Velasco, Woody Denham, John Linn, and Michael Ujiki have no conflict of interest or financial ties to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Krezalek, M.A., Bonamici, N., Kuchta, K. et al. Peritoneal dialysis catheter function and survival are not adversely affected by obesity regardless of the operative technique used. Surg Endosc 32, 1714–1723 (2018). https://doi.org/10.1007/s00464-017-5852-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5852-y