
Abstract
Introduction
Five billion people worldwide do not have timely access to surgical care. Cinterandes is one of the only mobile surgical units in low- and middle-income countries. This paper examines the methodology that Cinterandes uses to deliver mobile surgery.
Methods
Founding and core staff were interviewed, four missions were participated in, and internal documents and records were analysed between 1 May and 1 July 2014.
Results
Cinterandes performed 7641 operations over the last 20 years (60% gastrointestinal/laparoscopic), travelling 300,000 km to remote areas of Ecuador. The mobile surgery programme was initiated by a local Ecuadorian surgeon in 1980. Funding was acquired from businesses, private hospitals, and individuals, to fund a low-cost surgical truck, simple equipment, and running costs. The mobile surgical unit is a 24-foot modified Isuzu truck containing a preparation room with general equipment storage and running water, together with an operating room including the operating table, anaesthetic and surgical equipment. Mission structure includes: patient identification by a network of local medical personnel in remote regions; pre-operative assessment at 1 week by core team via teleconsultations; four-day surgical missions; post-operative recovery in tents or a local clinic; post-operative follow-up care by local personnel and remote teleconsultations. The permanent core team includes seven members; lead surgeon, lead anaesthetist, operating-room technician, medical coordinator, driver, general coordinator, and receptionist. Additional support members include seven regular surgeons, residents, medical students, and volunteers.
Conclusion
Surgery is a very effective way to gain the trust of the community, due to immediate results. Trust opens doors to other programmes (e.g. family medicine). Surgery can be incorporated with all other aspects of health care, which can in turn be incorporated with all other aspects of human development, education, food production and nutrition, housing, work and productivity, communication, and recreation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Five billion people worldwide do not have timely access to safe, affordable surgical care [1]. In the poorest third of the world, only 3.5% of the world’s surgery is delivered [2]. High-quality gastrointestinal and endoscopic care is rarely received by those in remote areas and the poor, particularly as a consequence of difficulties accessing surgical services due to distance, poor-quality road networks, and a lack of suitable transport [3, 4]. One solution brings surgical care to the patient through mobile surgery (MS).
Cinterandes, an Ecuadorian humanitarian mobile surgical programme, uses a truck equipped as an operating theatre to deliver surgery to the rural and remote patients in Ecuador. It is one of the only mobile surgical units in low- and middle-income countries (LMICs). The aim of this paper is to formally examine the methodology of the mobile surgical programme of Cinterandes.
Methods
Data were collected during 6-weeks field research working closely with Cinterandes (1 May to 1 July 2014). Numerous interviews were conducted with Cinterandes founding members ER (president/lead surgeon), ALV, EBR, together with core Cinterandes doctors and staff [5]. Four missions were joined with ER to Palmar and El Valle Cuenca, conducting 37 operations over 1200 km. Cinterandes records on mission protocols since inception in 1980 were analysed, together with notes on planning strategies and implementation [6]. The following discussions are based on the data, documents, and discussions as described above.
This paper examines how mobile surgery is delivered in Ecuador, focusing on three key domains:
-
1.
Initiation of the mobile surgery programme in Ecuador.
-
2.
Structure of Cinterandes mobile surgery programmes.
-
3.
Ideology and strategy of mobile surgery from Cinterandes.
The goal of this paper is to provide guidance for new mobile surgery programmes in other settings, through learning from the experiences of Cinterandes.
Results
Cinterandes has performed 7641 operations between 1994 and 2015, 60% of which were gastrointestinal and laparoscopic. It has travelled more than 300,000 km to provide free or affordable surgery in many remote and rural areas in Ecuador.
Initiation of the mobile surgery programme in Ecuador
Worldwide, surgery has on occasions been systematically delivered in a mobile unit through a variety of modalities, including by truck and ship [7,8,9]. Mobile surgery is a way of delivering surgical care to the patient’s own habitat; instead of bringing the patient to the operating room, the operating room is taken to the patient.
Ecuador is an example of an LMIC in which access to surgery is a substantial challenge for those living in rural and remote areas. Some of the main barriers include: geographical limitations imposed by the Amazonian and Andes mountains; difficulties in leaving their homes, crops and animals unattended; unfamiliarity, costs, and lodging associated with urban city-based hospitals; inconvenience encountered at hospitals and associated complexities and frustrations in receiving surgical care [10].
Local Ecuadorian surgeon ER recognised these barriers in 1980 and envisioned the MS concept as a way to defeat this by taking surgery to the rural and remote patients. However, there were many challenges in applying this concept in an LMIC such as Ecuador, including road infrastructures, perceived high cost, and limited governmental and financial support. Guidelines and examples to follow were rare, as there were minimal records or descriptions of truck-based MS performed prior to Cinterandes. It was not until 1994 that the mobile operating truck was designed, created, and imported to Ecuador, as well as funding for the programme acquired. In this time, several governmental and non-governmental organizations refused to support or finance the programme, until General Motors instructed its subsidiaries in Ecuador to do so. Aymesa, Maresa, B.B. Botar, and Fundación Grupo Aymesa financed the mobile unit; Ecuadoreans in the US San Francisco Bay Area and Ecuadorean ladies in US Washington D.C. provided the equipment. The local University of Cuenca and the University of Azuay gave full academic and material support to the programme. This helped in developing a low-cost purpose-built operating truck, obtaining simple equipment, and basic funding for running costs.
Between 1991 and 1994, prior to purchasing the mobile surgery truck, the core surgical team travelled to small rural hospitals, mostly in the Amazon Jungle, where the team developed unique skills in working together with limited resources. This also enabled them to identify the needs and requirements for their future truck. Ten pilot missions were conducted in total, nine of which were in the Amazon Jungle.
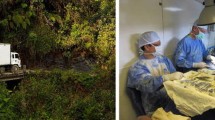
Since 1994, Cinterandes has performed on average 1–2 missions every month, travelling to the remotest parts of Ecuador (Fig. 1). The central office is located in Cuenca, where the planning and organisation of missions takes place. Cinterandes is a non-governmental, not-for-profit charitable organisation, providing surgical operations free of charge. It has gained national and international support and has also played a key role in the initiation, development, and implementation of mobile surgery in Honduras.

Cinterandes mobile surgical truck travelling through the heart of the Amazon Rainforest. Many patients here would never have had their surgery otherwise
Structure of Cinterandes mobile surgery programmes
-
1.
Structuring of mobile surgery programme and missions
Cinterandes has developed a well-defined programme to structure each individual mission into the following five stages:
-
(a)
Patient identification for mobile surgery
Destinations are planned several months in advance. Contact is made with known local medical personnel in the rural and remote region, to identify local needs and circumstances. The local medical personnel spread the word about the upcoming mission between local social circles, sometimes facilitated with leaflets. If any of the population think or have been told that they require a surgical operation, they are advised that they can visit the local medical personnel for an initial examination. A brief examination is conducted locally, and the patient is shortlisted for surgery if appropriate.
Selection of patients is vital in the context of MS. As a general principle, patients are selected who do not have pertinent co-morbidities or when difficult surgical procedures are anticipated from the technical perspective. Cinterandes considers the following factors as exclusion criteria for mobile operations:
-
Patients less than 1 year or more than 80 years of age.
-
Patients with an ASA class of 3 or above.
-
Patients with BMI over 30 are excluded from undergoing major operations.
-
Patients with large incisional hernias are usually excluded, as post-operative respiratory complications are frequent, and thus are high risk in requiring temporary respiratory support.
-
Patients who are generally anticipated to have severe technical and complicated problems during surgery.
Patients who fulfil any of these exclusion criteria are referred to hospital-based care. The proposed shortlist of potential surgical candidates is communicated with Cinterandes’ core team at the central office, and a draft itinerary for the mission is established. Official approval of the mission by local and national authorities is obtained in advance.
-
(b)
Pre-operative assessments of patients
Once the local medical contact has identified patients, a Cinterandes surgeon and anaesthetist visit the area to conduct pre-operative consultations, typically 1 week prior to the MS mission. Depending on location and the skill level of the local medical personal, this stage may also be facilitated, or occasionally replaced, with real-time video consultations. A careful history and physical examination is carried out. The accuracy of the diagnosis is confirmed, and laboratory tests and imaging are requested when indicated.
The pre-operative consultation enables an effective organisation of the operating schedule, patient evaluation and selection, and foreseeing medical supplies. It also saves valuable time during the remote visits, which in turn translates into more operating time.
-
(c)
Surgical missions
Missions are typically four days in duration. The truck travels one day prior, with the driver and the general assistant, to allow for setting up. It is typically stationed next to a health centre, school or community house where a preparation room and a recovery room are arranged. Depending on local facilities, three tents can also be set up for post-operative care. Rarely, in more urbanised areas, the truck is parked adjacent to the local hospital, as there are several small hospitals in Ecuador that despite having an operating room do not have the adequate personnel and functioning equipment. Being adjacent to a hospital enables the use of, besides the mobile surgical unit, the hospital operating room and the beds for hospitalisation of patients who need it.
At the start of each operating day, patients are once again interviewed and examined to ensure that pre-operative instructions were complied to, and that no additional pathology had developed such as respiratory or intestinal infections.
Missions usually consist of three days of continuous and intense surgery. There are at least 2–3 operating surgeons present on the mission, allowing for continuous operating based with rotating surgeons. At the start of each day, the mobile surgical unit is thoroughly cleaned and sterilized. Operations are carried out with great care, in accordance with pre-established protocols (Figs. 2, 3). Various modalities of anaesthesia are used, depending on the surgical procedure and circumstances, including local, regional, spinal, and general.

Inside perspective of the operating room

After the operation, the patient is transferred to a portable bed and descended by the hydraulic ramp
-
(d)
Post-operative recovery
Immediate post-operative care takes place either in tent facilities or in a local clinic (Fig. 4). Patients are carefully monitored by Cinterandes staff until they recover and are sent or taken home when they fulfil discharge criteria, and when there is no immediate risk of surgical or anaesthetic complications. From this moment, they are left under the care of the local medical personnel. A Cinterandes surgeon and anaesthetist are continuously available for consultation by phone and a home visit if necessary.

Post-operative care is provided in tent facilities or clinic settings. Waking up with family present, close to home, can have a significant positive impact on patient satisfaction
One of the benefits of operating on patients in their own environment and surroundings is in this post-operative stage, where patients, families, and relatives are often brought closer by sharing the burden of the surgical experience through immediate post-operative care. The first thing that children see when they wake up in the post-operative tent is the face of their mother or father.
-
(e)
Post-operative follow-up care
Patients are seen by local medical personnel, together with real-time audio or visual communication with the core Cinterandes team at the central office, post-operatively at 1 week, 1 month, 6 months, and 1 year. Telemedicine plays a critical role in the secondary post-operative care [11], where Cinterandes surgeons are able to speak to patients and assess surgical wounds remotely (Fig. 5).

Secondary post-operative care by Cinterandes surgeons taking place remotely from the central office in Cuenca, using telemedicine
Technology and communication in Ecuador, as in other LMICs, are limited. However, particularly over the last decade, mobile communication has become abundant in virtually all parts of Ecuador; currently, there are 16.5 million active cellular phones for a population of 15.6 million people [12]. In rural and remote areas, it is also typical that there is internet connection in at least the near vicinity. In such instances, the value of basic technology in low-resource settings is evident.
-
2.
Team structure to operate the mobile surgical programme
Cinterandes consists of seven permanent full-time members (Fig. 6) based at the central office:

Structure of the team for the central office and the mobile surgical unit team for missions. Core team members are marked using asterisk
-
President, lead surgeon: responsible for developing and implementing strategic plans of the Foundation, spear-heading the mobile surgery programmes, and foundation international representation and advocacy.
-
Executive director, lead anaesthetist: responsible for managing the staff, fundraising, building teams and coalitions, and implementing programme strategies.
-
Surgical coordinator: responsible for liaising with the network of known local medical contacts in remote regions. They are the first point of contact for any clinical queries.
-
Operating-room nurse, technician, and general assistant: responsible for stocks and equipment.
-
Driver/general assistant: responsible for the maintenance of the truck, planning of routes and supplies.
-
General coordinator: acts as the communicating point between Cinterandes and the various other entities.
-
Receptionist: provides secretarial, clerical, and administrative support.
During surgical missions in the truck, alongside the core team members listed above, there are further team members involved:
-
Seven regular surgeons, of whom one to two participate on each mission. These surgeons work voluntarily and rotate between themselves to provide service.
-
Resident surgeons from local hospitals.
-
Medical students, usually on elective experiences, to gain experiences in humanitarian and outreach strategies.
-
Local medical personnel in the rural and remote areas, who act as the bridge between local people and the surgical team.
-
Local district contacts and leaders, who aid in arranging for lodging, food, supplies, and security.
The team structure and members of Cinterandes have remained almost identical over the last 20 years, and this is one of the key reasons to the Foundation’s success. Each member has developed a certain level of expertise and experience in their role and maintains a level of loyalty and honesty to the Foundation.
-
3.
Mobile surgical unit truck specifications
The current mobile surgical unit is a 24-foot modified Isuzu truck. It is a tailor-made, purpose-built truck designed in Ecuador and assembled in USA by General Motors. The truck dimensions were specifically tailored, as although a larger and wider vehicle would have provided more operating space, the nature of the winding and narrow roads in rural Ecuador would not facilitate this.
There are two main rooms (Fig. 7):

Cinterandes mobile surgical truck design and layout
-
The operating room: This room contains a central operating table, stretcher for patient transfer, laparoscopic tower, electrosurgical generator, portable anaesthesia machine, mini-shelf with anaesthetic drugs, oxygen tanks, endosurgery generator, defibrillator, and a fire extinguisher. There are two storage cupboards in the corners of this room which stock multiple sets of sterile equipment. At the rear of this room, there is a wide door opening to a secure hydraulic powered ramp at the rear of the truck, allowing for the safe transport of the patient from the operating table to the ground.
-
The preparation room: This room includes a running-water tap and basin for surgical scrubbing, a wide table, multiple cabinets and cupboards for the storage of equipment, an autoclave, and a small bathroom.
Additional to the truck, a main office has been essential in providing the main strategic base for the planning of programmes, logistical and travel arrangements, and storage of equipment. The 110-m2 office is based in the city of Cuenca, where most of the team members reside.
-
4.
Types of surgical operations performed as mobile surgery
Gastrointestinal operations are among one of the most appropriate types of procedures for mobile surgical unit circumstances. This is mainly due to appropriate post-operative care in simple community-based settings, suitability of the required surgical equipment, and recovery times. The types and frequencies of the various surgical operations performed by Cinterandes since inception in 1994 are demonstrated in Tables 1 and 2. Complication rates have been far below 1%, similar to tertiary hospitals in developed countries. There have been no patient mortalities. Typical patient demographics are demonstrated in Table 3 over a 12-month period.
-
5.
Cost-effectiveness of mobile surgery
Mobile surgery is highly cost-effective. During 2014 [13], Cinterandes performed 202 surgical procedures on local patients in 10 different regions of Ecuador. The cost incurred by Cinterandes (DI) was $121,356. The total real market cost (TR) which disregards donated and discounted items and time was $212,135. Total DALYs averted was 1258. The cost-effectiveness ratio was $96/DALY (DI) or $169/DALY (TR), respectively. This is highly comparable to hospital-based surgery in LMICs which typically costs $50–$400/DALY [14]. It also compares favourably with other traditional public health interventions in LMICs; BCG vaccine for tuberculosis at $50-$250/DALY, antiretroviral therapy for HIV at $500/DALY, and oral rehydration therapy at $1000/DALY.
Ideology and strategy of mobile surgery from Cinterandes
Surgery is a very effective way to gain the trust of the community, as it produces immediate and quantifiable results. From Cinterandes’ experience, this trust can open doors to other programs such as family medicine which are often more challenging to embrace as many of their benefits may be invisible or slow. An example includes the reduction in malnutrition rates following surgical missions to the small village of Santa Ana high in the Andes Mountains. Basic nutritional concepts had been previously introduced in this region, with little acceptance. However, after seeing the results of patients operated on in the mobile surgical unit, together with structured education and encouragement from the surgical team towards basic nutritional concepts, the malnutrition rate in children aged 1 year old dropped from 28.4 to 5.6%, and for children aged 1–4 years old dropped from 32.3 to 7.1%, between 2002 and 2005 [15]. In a survey of 101 Cinterandes patients in 2014 [5, 10], 47% of patients cited ‘trust’ as the reason why they chose mobile surgery by Cinterandes.
In our current era, the financial burden of seeking surgery is substantial. It is estimated worldwide, one quarter of people who undertake a surgical procedure experience ‘catastrophic expenditure’ as a result of seeking care (direct out-of-pocket payments >40% of household income net of subsistence needs) [16, 17]. In the light of this, the fee strategy of the mobile surgical unit is essential in determining accessibility for poor patients. Cinterandes has always functioned under the philosophy that surgery for these rural and remote poor patients should be free of charge, unless the patient feels they are able and in the position to pay, in which case they decide their own fee appropriate for them (for which a guidance is available). Cinterandes functions as a humanitarian, rather than a business for-profit approach. It can be argued that as mobile surgery is indeed cost-effective, it could be run as a profit-generating business. However, the philosophies of Cinterandes maintain that in such instances, the primary priority of providing accessible surgery for rural and remote poor patients may be compromised.
Sincerity and compassion from patients in rural communities should not be underestimated. Communities care when their local people receive good treatment and reciprocate this through taking care of the team out of genuine compassion and love. This in turn supports and facilitates the missions. For the vast majority of Cinterandes’ missions, the lodging, food, and security were taken care of by the local community.
Surgery can be incorporated with all other aspects of health care. Health care should in turn be incorporated with all other aspects of human development; education, food production and nutrition, housing, work and productivity, communication, and recreation (Fig. 8). One of Cinterandes’ essential principles is in promoting human development. This human development acts as the liberation of human potential, leading to mankind’s progress, well-being and improvement of quality of life of the individual and the community, with liberty and in harmony with the environment.

Model demonstrating how mobile surgery and health care should be integrated with all other aspects of human development to enhance human potential and quality of life. Note health is central not only because of its importance to assure quality of life, but because the team who began the programme are physicians, and health care is the centre of their activities
In the experience of Cinterandes, it is essential to recognise that mobile surgery is not simply transporting a hospital to the patient. There are many limitations that must be recognised, including lack of post-operative intensive-care facilities, reduced access to care post-operatively after the core team leave, fewer resources, and more limited space. Patient selection and patient care are adapted to ensure quality and safe surgery. More complex surgeries and patients with significant co-morbidities are referred to established hospitals. Good patient outcomes along with appropriate referral builds patient and community trust, which enables a broader impact for a variety of health care and public health interventions
With this, the concept of ‘mobility’ is changing the health delivery system. If surgery, with all of its complexity, can be performed successfully in a mobile way, most other fields of health care can also be performed in this way.
Conclusion
Cinterandes has demonstrated that in Ecuador, mobile surgery has enabled patients in rural and remote areas to undertake operations that many would not have otherwise had; in this case 7641 patients over 20 years. This has not been without challenges, including local and government support, financing, local infrastructure, development of a programme, and successful team. The mobile surgery programme is structured to address all areas of the patient’s perioperative care, to ensure a safe and high-quality surgical experience for the patient. Technology has played an essential role in enabling communication between patients in remote areas and the surgical team. The Cinterandes programme structure may provide guidance for other countries to adopt and adapt, tailoring to local needs, requirements, and limitations.
References
Meara JG, Leather AJ, Hagander L et al (2015) Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 386(9993):569–624
Weiser TG, Regenbogen SE, Thompson KD et al (2008) An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372(9633):139–144
Grimes CE, Bowman KG, Dodgion CM et al (2011) Systematic review of barriers to surgical care in low-income and middle-income countries. World J Surg 35:941–950
Grimes CE, Law RSL, Borgstein ES et al (2012) Systematic review of met and unmet need of surgical disease in rural sub-Saharan Africa. World J Surg 36:8–23
Rodas E, Vicuña AL, Rodas EB (2014) President, Founder, and Lead Surgeon. Cinterandes Foundation. 25 interviews with the author between 01/05/2014 and 01/07/2014. Personal communication
Cinterandes Foundation (1980–2014). Internal documents, reports, and databases. Cinterandes Central Office, Cuenca, Ecuador. Unpublished
Fontana M, Lucha P, Snyder M et al (1999) Surgery aboard ship: is it safe? Mil Med 164(9):613–615
Cheng LHH, McColl L, Parker G (2012) Thyroid surgery in the UK and on board the Mercy Ships. Br J Oral Maxillofac Surg 50(7):592–596
Sechriest VF, Lhowe DW (2008) Orthopaedic care aboard the USNS Mercy during operation unified assistance after the 2004 Asian Tsunami. J Bone Joint Surg Am 90(4):849–861
Price MD, Shalabi HT, Shalabi ST et al (2015) Is mobile surgery successful in overcoming patient barriers to surgery? Poster session presented at: Extreme Affordability Global Health Conference 2015, Centre for Global Surgery, University of Utah. 3rd Annual Conference. 10–11 April 2015; Salt Lake City, Utah, USA
Mora F, Cone S, Rodas E et al (2006) Telemedicine and electronic health information for clinical continuity in a mobile surgery program. World J Surg 30:1128–1134
Central Intelligence Agency (2015) Ecuador. In The World Factbook. www.cia.gov/library/publications/the-world-factbook/geos/ec.html. Last Accessed 17/04/2015
Shalabi HT, Price MD, Shalabi ST et al (2015) Cost-effectiveness of mobile surgery in low- and middle-income countries: an Ecuadorian case study. Oral presentation at: 46th World Congress of Surgery. International Society of Surgery. 23–27 August 2015; Bangkok, Thailand
Chao TE, Sharma K, Mandigo M et al (2014) Cost-effectiveness of surgery and its policy implications for global health: a systematic review and analysis. Lancet Glob Health 2:e334–e345
De Vries C, Price R (2010) Global surgery and public health: a new paradigm. Jones and Bartlett, Sudbury
Doorslaer V, O’Donnell O, Rannan-Eliya RP et al (2006) Effect of payments for health care on poverty estimates in 11 countries in Asia: an analysis of household survey data. Lancet 368(9544):1357–1364
Bickler SW, Weiser TG, Kassenbaum N et al (2014) Chapter 2: Global burden of surgical conditions. In: Disease control priorities, 3rd edn: Economic Evaluation for Health. World Bank, Washington
Acknowledgments
Dr. Edgar Rodas, founder and leader of Cinterandes since inception in 1980, sadly passed away on 2 March 2015. It is because of his visions and fortitude that Cinterandes has remained one of the most successful mobile surgical units in the developing world, dedicated to treating the poor and remote population. The methodology, concepts, and principles of Cinterandes examined in this paper were his visions and ideologies. This paper is dedicated in his memory. Further acknowledgements and thanks are made to Freddy Peralta (operating-room technician), Gonzalo Matute (driver and assistant), Carolina Donoso (general coordinator), Janeth Matute Mendoza (administration manager), and Dolores Rodas (visionary) for their substantial aid and initiatives in acquiring archived and current data and documents.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
HT Shalabi, MD Price, ST Shalabi, EB Rodas, AL Vicuña, B Guzhñay, RR Price, and E Rodas have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Shalabi, H.T., Price, M.D., Shalabi, S.T. et al. Mobile gastrointestinal and endoscopic surgery in rural Ecuador: 20 years’ experience of Cinterandes. Surg Endosc 31, 4964–4972 (2017). https://doi.org/10.1007/s00464-016-4992-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-4992-9