
Abstract
Background
Laparoendoscopic single-site (LESS) surgery has been established for various procedures. Shortcomings of LESS surgery include loss of triangulation, instrument collisions, and poor ergonomics, making advanced laparoscopic tasks especially challenging. We compared a LESS system with a robotic single-site surgery platform in performance of a suturing and knot-tying task under clinically simulated conditions.
Methods
Each of five volunteer minimally invasive surgeons was tasked with suturing a 5 cm longitudinal enterotomy in porcine small intestine with square knots at either end, using a laparoendoscopic or da Vinci robotic single-site surgery platform, within a 20 min time limit. A saline leak test was then performed. Each surgeon performed the task twice using each system. The time to completion of the task and presence of a leak were noted. Fisher’s exact test was used to compare the overall completion rate within the defined time limit, and a Wilcoxon rank test was used to compare the specific times to complete the task. A p value of <0.05 was considered significant.
Results
All surgeons were able to complete the task on the first try within 20 min using the robot system; 60 % of surgeons were able to complete it after two attempts using the LESS surgery system. Time to completion using the robot system was significantly shorter than the time using the standard LESS system (p < 0.0001). There were no leaks after closure with the robot system; the leak rate following the standard LESS system was 90 %.
Conclusions
Surgeons demonstrated significantly better suturing and knot-tying capabilities using the robot single-site system compared to a standard LESS system. The robotic system has the potential to expand single-site surgery to more complex tasks.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Standard multiport laparoscopic surgery is commonly performed in general surgery. The number of laparoscopic operations has increased over the past few decades and is considered the standard of care for certain procedures [1]. The hallmark of laparoscopic surgical procedures is the concept of triangulation, which requires multiple instruments to approach the center of the surgical field from several points separated by space. This allows for a better spatial understanding of a 3D field viewed on a 2D monitor, effective tissue retraction and countertraction, and an improved ergonomic working environment. Fundamental to performance of surgical procedures is suturing and knot tying, which requires specific skill to be performed laparoscopically. Laparoscopic multisite suturing and knot tying are considered to be advanced skills that have widened the use of minimally invasive surgery [2]. Thus, complex surgical operations can be routinely performed using laparoscopic techniques. However, attaining proficiency in these skills often requires a structured teaching curriculum and multiple repetitions [3].
Laparoendoscopic single-site (LESS) surgery, was introduced in the 1990s but gained momentum as an advanced surgical technique and laparoscopic surgical approach only a decade later [4]. Since then, LESS surgery has been established for cholecystectomy, appendectomy, and nephrectomy, among other procedures. The proposed benefits of LESS surgery include decreased postoperative pain, faster recovery time, fewer wound complications, and improved cosmesis [4]. However, the standard multiport laparoscopy and LESS surgery have not been compared in a large trial. Meanwhile, single-site surgery is associated with several technical problems that are inherent to the technique itself. Loss of triangulation, collisions of the instruments, collisions of the instruments with the laparoscope and camera head, lack of maneuverability, and lack of proper exposure are all considered shortcomings of LESS surgery, making advanced laparoscopic tasks cumbersome [5].
As already noted, laparoscopic suturing and knot tying are considered advanced skills with a steep learning curve. Although the multisite approach to laparoscopic surgery is the gold standard, increasingly complex operations are attempted with a minimal port approach. Suturing and intracorporeal knot tying with single port systems poses significant difficulty, often requiring conversion to traditional multiport laparoscopy or even open surgery. In fact, while suturing with extracorporeal knot tying is described, few reports describe the learning curve of intracorporeal knot tying using LESS surgical techniques [6, 7].
A specialized robotic platform for single-site surgery was developed in an attempt to overcome the technical difficulties inherent to LESS surgery and to improve operator ergonomics [8, 9]. It has therefore been suggested that the robotic single-site platform would make more complex laparoscopic tasks easier than using more conventional single-incision laparoscopic surgical techniques. In this study, we used a surgical task using suturing and knot tying to compare the laparoendoscopic to the robotic single-site platforms.
Materials and methods
This study employed five minimally invasive surgeons from three separate institutions. Each had previous training in LESS and varying experience with performing single-site surgery in their practice. Similarly, each of the surgeons received the minimal formal training for use of the da Vinci (Intuitive Surgical, Inc., Sunnyvale, CA) robot multiport system (which also includes a box-trainer skills lab). Most had performed at least one robotic multiport operation; none had performed a purely single-site robotic operation in their practice.
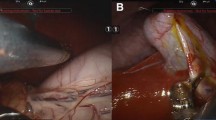
Each surgeon was required to perform a predetermined suturing task using a common LESS surgery platform, and compared to the same task performed using the robotic single-site platform. The task was performed in a standard box trainer on explanted porcine small intestine containing a longitudinal 5 cm incision.
Each of the five participants was allowed a maximum of 20 min to complete a running suture closure of the longitudinal enterotomy, with intracorporeal knot tying at each end of the running suture. A saline leak test was then performed to check the integrity of the closure and the successful completion of the task. This was done with injection of 60 ml of saline under constant pressure with a standard syringe.
Each participant was required to complete the suturing task twice using a standard LESS surgical platform, and twice using the robotic single-site platform. They were randomly assigned to which task they attempted first to minimize the transfer of learning from one task to the other. In addition, a specified amount of elapsed rest time was required between tasks. Successful completion of the task within the allotted time, as signified by the results of the saline leak test, was recorded as the primary outcome.
The LESS platform comprised a SILS port (Covidien, Norwalk, CT), 5 mm cannulae, and an Olympus EndoEye 5 mm articulating laparoscope (Olympus America, Center Valley, PA). Participants were allowed to choose any combination of common commercially available manual rigid or articulating needle drivers or graspers.
The robotic platform included the curved cannulae, an 8.5 mm camera cannula, and 8.5 mm 30° scope. Each participant was allowed to choose any combination of robotic single-site platform needle driver or Maryland dissector to complete the task. A study observer and a study supervisor oversaw the administration of each test session, and each participant was blinded to the performance of the other four participants.
Fisher’s exact test was used to compare overall completion rate of the suturing task within the defined time limit between the two single-site surgical methods. Leak rates were similarly compared. A Wilcoxon rank test was used to compare the times to complete the suturing tasks. A p value of <0.05 was considered significant.
Results
Of the five minimally invasive surgeons who participated in the study, four were men and one was a woman, with ages ranging from 38 to 56 years, and having 4 to 18 years of posttraining minimally invasive surgical experience (Table 1). On average, each had previously performed 42 LESS surgical procedures and 49 multiport robotic operations. All had been previously introduced to the robotic single-site platform at the Intuitive Surgical, Inc., training laboratory (Sunnyvale, CA), but none had personal experience with purely single-site robotic surgery in clinical practice.
In the first attempt using the LESS approach, only one surgeon of five (20 %) was able to complete enterotomy suture closure before the 20-min time limit. The number improved to 3–5 (60 %) successful surgeons in the second attempt (Table 2). The average amount of time required to complete the task, among those who were able to do it in <20 min, was 17 min, 34 s. In comparison, all participants completed the same task using the robotic system. In the first attempt, the task was completed with an average time of 15 min, 2 s, and an average time of 16 min, 11 s, in the second attempt. The time to completion using the robotic single-site system was significantly shorter than the time required using the standard LESS system (p < 0.0001). When surgeons were stratified on the basis of the level of prior experience with multiport robotic surgery, there was no difference in the ability to complete the tasks between novice, intermediate, and expert surgeons. All surgeons expressed subjectively more fatigue after using the LESS system compared to the robot.
All enterotomy suture closures were tested for leak, whether or not all steps were completely done, as a clinically meaningful measure of a truly completed task. Using the LESS surgery system, 9 of 10 total attempts to close the enterotomy resulted in leaks, with a total leak rate of 90 % (Table 3). Using the robotic single-site system, none of the enterotomy closures resulted in a saline leak in either the first or second attempt (leak rate of 0 %).
Discussion
Initially described as an evolution of the laparoscopic cholecystectomy, LESS surgery has now been performed in general, urologic, and gynecologic surgery. Single-site laparoscopic general surgery has been performed in all quadrants of the abdomen, involving the gastrointestinal tract, hernia repair, and solid organ resections, seeking to demonstrate feasibility and an improvement on multisite laparoscopic surgery [10, 11]. Studies have shown the procedures to be safe and without increased morbidity, and the main arguments supporting the single-site approach have been improved cosmesis and decreased postoperative pain compared to multiport laparoscopic surgery [12–14]. Published articles over the past decade suggest that more than 4,500 single-site laparoscopic operations were performed, reflecting a progressively increasing interest and development of surgical techniques [15]. Cholecystectomy and appendectomy together comprise more than 60 % of the cases reported. Adoption of single-site laparoscopic techniques, however, has not been universal as a result of concerns about postoperative pain and wound complications, but also as a result of intraoperative technical concerns and a steep learning curve.
Despite the fact that proficient minimally invasive surgeons are typically the ones to adopt LESS surgery, there is still a steep learning curve. Although it varies with the procedure performed, it nonetheless commonly requires dozens of repetitions to attain proficiency [16–18]. The loss of triangulation, collisions of the instruments and laparoscope, and difficulty with tissue exposure often lead to awkward positioning and ergonomics [19]. In addition, with all of the instruments and camera working from a single fulcrum at the umbilicus, attempts to avoid clashing extracorporeally result in a sensation of working in mirror image, intracorporeally. This can be disorienting to the surgeon, and development of new technology, including flexible instruments and laparoscopes, has attempted to decrease this effect. Flexible instruments and those designed to curve are meant to compensate for the loss of triangulation. Despite this, however, complex laparoscopic tasks, such as suturing and knot tying, remain difficult and cumbersome.
There is new evidence that for basic laparoscopic cases, such as cholecystectomy, the robotic single-site system may allow the surgeon to more quickly overcome the typical single-site learning curve [20]. The robot removes the collisions from the procedure, as the machine takes over the movement of the instruments and camera. The flexible instruments and curved cannulae provide a consistent and predictable angle of approach to the operative target relative to the camera and reconstitutes triangulation. In addition, it is suggested that by swapping the instrument controls between the right and left hands at the console, the sensation of operating in mirror image is eliminated.
In this study, we chose to evaluate the ability of skilled surgeons to suture and tie knots, which are complex tasks fundamental to surgery, yet that are avoided in most LESS surgical procedures as a result of their technical difficulty. The difficulty of these tasks was redemonstrated in this study using common LESS surgical equipment. In this early experience with the robotic single-site system, we also found that the common difficulty experienced in single-site surgery can be overcome in a short time and with few repetitions using the robotic platform. Suturing and knot tying were accomplished by all study participants on the very first attempt, with high precision. An important note is that the robotic single-site surgery platform instruments are not “wristed” like regular robotic instruments. Thus, the ease of use of the robotic single-site platform was a function of the improved ergonomics, geometry, and visualization, not the wristed instruments.
Setup time for each of the systems (e.g., robotic docking, placement of the port) was not included in the time measurements in this study. The setup for the robot is often considered time-consuming, in which the docking of the robot itself has a learning curve. Including setup time in this study is confounding, and although it is relevant to an actual operation, is less relevant in this study, which focuses on the ability of two techniques to perform a specific task.
A significant limitation of this study is the small number of participants. Although multisite approaches remain the gold standard for laparoscopic surgery, there is continued interest in single-site techniques. Here we compare two different single-site platforms in the ability of skilled surgeons to complete a predefined task using each platform. The number of surgeons was small, but nonetheless, the differences that were identified between the two techniques were immediately apparent and statistically significant. The introduction of new technology into surgical practice has become a frequent occurrence in clinical practice, and its adoption often precedes published data. As in this study, it is important to scrutinize new technologies and share significant data. To further compare the learning curves for performing complex laparoscopic tasks, future studies will need to be designed comparing robotic to LESS surgery with a larger cohort and using in vivo models.
Conclusion
Suturing and knot-tying tasks were performed with significantly greater ease and higher precision using the robotic single-site platform than the LESS platform. This system may expand the utility and implementation of single-site surgery in general practice. Further studies are needed to test single-site platforms in other surgical tasks and in vivo models.
References
NIH Consensus Conference (1993) Gallstones and laparoscopic cholecystectomy. JAMA 269:1018–1024
Allen JW, Rivas H, Cocchione RN, Ferzli GS (2003) Intracorporeal suturing and knot tying broadens the clinical applicability of laparoscopy. JSLS 7:137–140
Stefanidis D, Hope WW, Korndorffer JR Jr, Markley S, Scott DJ (2010) Initial laparoscopic basic skills training shortens the learning curve of laparoscopic suturing and is cost-effective. J Am Coll Surg 210:436–440
Ross S, Rosemurgy A, Albrink M, Choung E, Dapri G, Gallagher S, Hernandez J, Horgan S, Kelley W, Kia M, Marks J, Martinez J, Mintz Y, Oleynikov D, Pryor A, Rattner D, Rivas H, Roberts K, Rubach E, Schwaitzberg S, Swanstrom L, Sweeney J, Wilson E, Zemon H, Zundel N (2012) Consensus statement of the consortium for LESS cholecystectomy. Surg Endosc 26:2711–2716
Rao PP, Rao PP, Bhagwat S (2011) Single-incision laparoscopic surgery—current status and controversies. J Minim Access Surg 7:6–16
Schill MR, Varela JE, Frisella MM, Brunt LM (2012) Comparison of laparoscopic skills performance between single-site access (SSA) devices and an independent-port SSA approach. Surg Endosc 26:714–721
Endo T, Nagasawa K, Umemura K, Baba T, Henmi H, Saito T (2011) A remarkably easy knot-tying technique for single-incision laparoscopic surgery with the SILS port for gynecologic diseases. J Minim Invasive Gynecol 18:500–502
Wren SM, Curet MJ (2011) Single-port robotic cholecystectomy; results from a first human use clinical study of the new da Vinci single-site surgical platform. Arch Surg 146:1122–1127
Escobar PF, Knight J, Rao S, Weinberg L (2012) da Vinci single-site platform: anthropometrical, docking and suturing considerations for hysterectomy in the cadaver model. Int J Med Robot 8:191–195
Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I (1997) One-wound laparoscopic cholecystectomy. Br J Surg 84:695
Gill IS, Advincula AP, Aron M, Caddedu J, Canes D, Curcillo PG 2nd, Desai MM, Evanko JC, Falcone T, Fazio V, Gettman M, Gumbs AA, Haber GP, Kaouk JH, Kim F, King SA, Ponsky J, Remzi F, Rivas H, Rosemurgy A, Ross S, Schauer P, Sotelo R, Speranza J, Sweeney J, Teixeira J (2010) Consensus statement of the consortium for laparoscopic single-site surgery. Surg Endosc 24:762–768
Curcillo PG 2nd, Wu AS, Podolsky ER, Graybeal C, Katkhouda N, Saenz A, Dunham R, Fendley S, Neff M, Copper C, Bessler M, Gumbs AA, Norton M, Iannelli A, Mason R, Moazzez A, Cohen L, Mouhlas A, Poor A (2010) Single-port access (SPA) cholecystectomy: a multi-institutional report of the first 297 cases. Surg Endosc 24:1854–1860
Teoh AY, Chiu PW, Wong TC, Poon MC, Wong SK, Leong HT, Lai PB, Ng EK (2012) A double-blinded randomized controlled trial of laparoendoscopic single-site access versus conventional 3-port appendectomy. Ann Surg 256:909–914
Phillips MS, Marks JM, Roberts K, Tacchino R, Onders R, DeNoto G, Rivas H, Islam A, Soper N, Gecelter G, Rubach E, Paraskeva P, Shah S (2012) Intermediate results of a prospective randomized controlled trial of traditional four-port laparoscopic cholecystectomy versus single-incision laparoscopic cholecystectomy. Surg Endosc 26:1296–1303
Pfluke JM, Parker M, Stauffer JA, Paetau AA, Bowers SP, Asbun HJ, Smith CD (2011) Laparoscopic surgery performed through a single incision: systematic review of current literature. J Am Coll Surg 212:113–118
Song T, Kim TJ, Lee YY, Choi CH, Lee JW, Kim BG, Bae DS (2012) Learning curves for single-site laparoscopic ovarian surgery. J Minim Invasive Gynecol 19:344–349
Park YH, Balk KD, Lee YJ, Kim KT, Kim HH (2012) Learning curve analysis for laparoendoscopic single-site radical nephrectomy. J Endourol 26:494–498
Gawart M, Dupitron S, Lutfi R (2012) Laparoendoscopic single-site gastric bands versus standard multiport gastric bands: a comparison of technical learning curve measured by surgical time. Am J Surg 203:327–329
Merchant AM, Cook MW, White BC, Davis SS, Sweeney JF, Lin E (2009) Trans-umbilical gelport access technique for performing single incision laparoscopic surgery (SILS). J Gastrointest Surg 13:159–162
Pietrabissa A, Sbrana F, Morelli L, Badessi F, Pugliese L, Vinci A, Klersy C, Spinoglio G (2012) Overcoming the challenges of single-incision cholecystectomy with robotic single-site technology. Arch Surg 147:709–714
Disclosures
Dr. Lau is on the medical advisory board for Miret Surgical. Dr. Rivas is a consultant for Covidien. Drs. Eisenberg, Vidovszky, Lau, Guiroy, and Rivas received an honorarium for participation in this study from Intuitive Surgical, Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eisenberg, D., Vidovszky, T.J., Lau, J. et al. Comparison of robotic and laparoendoscopic single-site surgery systems in a suturing and knot tying task. Surg Endosc 27, 3182–3186 (2013). https://doi.org/10.1007/s00464-013-2874-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-2874-y