
Abstract
Background
This study was designed to evaluate the feasibility and safety of total laparoscopic sigmoid and rectal surgery without abdominal incision in combination with transanal endoscopic microsurgery (TEM).
Methods
From May 2010 to October 2011, 34 patients with colon and rectal tumors were treated by total laparoscopic surgery without abdominal incision, and the clinical data of these patients were reviewed.
Results
All operations could be successfully accomplished without conversion to open surgery. No diverting ileostomy was created. The average operative time was 151.60 (range, 125–185) minutes. The average blood loss was 200.20 (range, 55–450) ml. All resection margins were negative. Six patients developed postoperative anastomotic leakage. There were no reports of other complications in all patients.
Conclusions
This preliminary study indicated that total laparoscopic sigmoid and rectal surgery in combination with TEM was a safe, feasible, and minimally invasive technique. This advanced surgical technique was developed by combining laparoscopy with the concept of natural orifice transluminal endoscopic surgery.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Laparoscopic procedures have developed increasingly during the past 20 years. Compared with open surgery, minimally invasive colorectal procedures, such as laparoscopic-assisted colectomy, have been shown to have better outcomes, such as faster recovery, improved cosmetic results, and less postoperative pain, and can simultaneously offer safe and proper tumor resection in cases of colon and rectal cancer [1–7]. However, during the conventional laparoscopic-assisted colectomy, an additional abdominal incision needs to be made for specimen retrieval and anastomosis, which negates some of the advantages offered by laparoscopy and increases the possibility of incision- and implantation-related complications. In sphincter-preserving surgery for low rectal cancer, it is difficult to assess the adequate surgical margins and perform ultra-low rectal cross-clamping using conventional laparoscopy.
Since the concept of natural orifice transluminal endoscopic surgery (NOTES) was first presented, transanal removal of the specimen during laparoscopic colorectal procedures is an appealing concept in terms of its minimally invasive nature and its similarity to the concept of NOTES. Cheung et al. [8] have reported laparoscopic colectomy without minilaparotomy for left-sided colonic tumors by extracting the specimen via the anus, Leroy et al. [9] have evaluated a prospective study for 16 laparoscopic resections with transanal specimen extraction for sigmoid diverticulitis, and Lacy et al. [10] have completed a transvaginal minilaparoscopic-assisted natural orifice surgery (MA-NOS) for radical sigmoidectomy. Recently, we performed total laparoscopic sigmoid and rectal resection in combination with transanal endoscopic microsurgery (TEM). Using this procedure, we could determine the distal resection margin and perform resection under direct visualization by TEM; the resected specimen was extracted via the natural orifice, which helped us avoid an abdominal incision.
Materials and methods
Inclusion and exclusion criteria
The inclusion criteria for this study were: (1) Tumor location in the rectum and sigmoid colon with diameter >1 cm, but <4 cm; (2) Local spread restricted to the sigmoid/rectal wall (T1–T3) as determined by preoperative CT, MRI, or endorectal ultrasonography for the cancer in sigmoid and upper rectum, local spread restricted to internal sphincter (T1/T2) for lower rectal cancer; (3) Absence of synchronous distant metastasis.
The exclusion criteria were: (1) Patients with history of pelvic operation; (2) Patients with synchronous distant metastasis; (3) Tumor diameter >4 cm, which is the diameter of TEM resectoscope shaft; (4) Tumors located >30 cm from the anal verge, which are difficult for transanal end-to-end anastomosis by circular stapler; (5) Tumors located <4 cm from the anal verge, which require abdominoperineal resection.
Patients
From May 2010 to October 2011, we performed total laparoscopic sigmoid and rectal resection in combination with TEM (Richard Wolf TEM Instrument System, Shanghai, China) in 34 patients (19 men, 15 women; average age, 56.5 (range, 41–78) years) with colorectal tumors. The data of these patients are reviewed in Table 1. The study had been approved by the ethics committee of our institution. The main symptoms at the time of diagnosis were hematochezia (25 patients), altered bowel habits (5 patients), and abdominal pain (1 patient). Colorectal tumor was identified during physical examination in one patient, tumor recurrence after endoscopic polypectomy was observed in one patient, and a salvage operation had to be performed in one patient after pathological diagnosis confirmed the adenocarcinoma after local excision. The average BMI of the patients was 24.6 (range, 19.8–30.3). The average distance of the tumors from the anal verge was 11.5 (range, 4–30) cm. The tumors were located in the upper rectum in 15 patients, the sigmoid colon in 6 patients, and the mid or lower rectum in 13 patients. (The upper rectum is regarded as rectum above the peritoneal reflection, above 8 cm from the anal verge; and the mid or lower rectum is below the peritoneal reflection, within 8 cm from the anal verge.) The preoperative clinical staging was T1-2N0M0 in nine patients, T1-2N1M0 in three patients, T3N0M0 in ten patients, T3N1M0 in six patients, and adenoma in five patients.
Preoperative preparation
Before performing the operation, the patients’ complete medical records and history were reviewed. All patients were subjected to digital rectal examination, colonoscopy, which was important for tumor biopsy, chest radiograph, and abdominal and pelvic computed tomography (CT) scan. Patients with tumors in the lower rectum underwent additional examination by endorectal ultrasonography or magnetic resonance imaging to determine the possibility of anal sphincter-preserving operation. Polyethylene glycol electrolyte solution was administered 1 day before operation for bowel preparation. Prophylactic antibiotics (cefuroxime, 2.25 g; metronidazole, 200 mg) were intravenously administered before the operation.
Details of the technique
Operative posture and location of trocar
Patients were placed in a modified lithotomy position with the head tilted downward and general anesthesia was administered, after which a pneumoperitoneum was created. Five-port technique is the standard approach for laparoscopic LAR/sigmoid resection in our institute. A 12-mm camera port was created in the supraumbilical region and the 10-mm laparoscope was inserted via this port; three 5-mm surgical ports were created on the upper right, upper left, and lower left abdominal quadrants; a 12-mm surgical port was created on the right lower quadrant. Under laparoscopic guidance, routine intra-abdominal exploration was performed.
Mobilization
Complete mobilization of the sigmoid and left colon and dissection of the inferior mesenteric artery close to its origin and the inferior mesenteric vein at the inferior border of the pancreas were performed. Subsequently, partial or total mesorectal excision (TME) was performed according to the tumor location. The resectoscope shaft (diameter, 40 mm) for TEM was inserted into the rectum through the anus after gentle dilatation, and the intestine was maintained in an extended state by insufflation (carbon dioxide; pressure, 12–15 mmHg). The distal resection margin was endoscopically confirmed. After trimming the proximal and distal mesocolon, a circumferential incision of the rectum at least 2 cm below the tumor was made by using a harmonic scalpel (Johnson & Johnson, Ethicon, Shanghai, China) laparoscopically and sometimes helped by using a monopolar cautery transanally. The end of the proximal bowel was ligated laparoscopically using hemp rope to occlude the bowel and prevent the outflow of intestinal contents and prevent contamination in the abdominal cavity.
Resection and anastomosis
On the basis of the tumor location, we used different methods to deliver mobilized rectum and sigmoid colon through the resectoscope and finish the anastomosis:
-
(1)
For tumors in the upper rectum, the mobilized colon and rectum were carefully packed into a specimen bag and exteriorized through the TEM resectoscope shaft (Fig. 1), and proximal colonic resection was performed transanally by first creating a pursestring suture and then inserting a circular stapling anvil into the proximal end of the bowel. The colon was then replaced in the abdominal cavity, after which we performed iodine solution lavage of the abdominal and pelvic cavity. The distal stump of the rectum was transversely clamped using a stapler (Covidien, AutoSuture, Endo GIA Roticulator™ 60–3.5 Sulu; Fig. 2). Then, a circular stapler (Covidien, AutoSuture, DST series™ EEA™ 31 mm or Johnson & Johnson, Ethicon, DST series™ EEA 33 mm) was inserted transanally, and an end-to-end anastomosis was laparoscopically created under direct visual control (Fig. 3).
Fig. 1 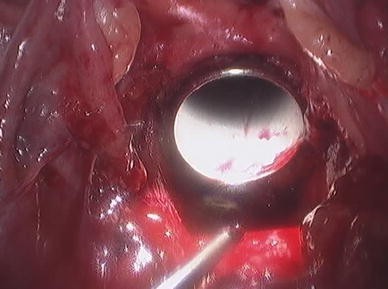
TEM resectoscope shaft for delivering mobilized rectum and sigmoid colon
Fig. 2 
Distal stump of the rectum was transversely clamped by using a Endo GIA stapler
Fig. 3 
Circular stapler was inserted transanally, the anvil was attached in position, and an end-to-end anastomosis was laparoscopically created
-
(2)
For tumors in the sigmoid colon, in case the colon could not be sufficiently mobilized to be pulled out through the anus, the proximal colon was resected transversely using a harmonic scalpel, and the specimen was exteriorized through the TEM resectoscope shaft in a specimen bag. The anvil of the circular stapler was then inserted into the abdominal cavity through the TEM resectoscope, and pursestring sutures were made circumferentially at the proximal end of the bowel and the anvil was inserted into it laparoscopically (Fig. 4). The distal stump of the rectum was clamped using an Endo GIA stapler, after which a circular stapler was inserted transanally and end-to-end anastomosis was created.
Fig. 4 
Purse-string sutures were made circumferentially at the proximal end of the bowel and the anvil was inserted into it laparoseopically
-
(3)
For tumors in the mid and lower rectum, the mobilized rectum, and sigmoid colon were carefully packed into a specimen bag and exteriorized through the TEM resectoscope shaft and the proximal colon was transected transanally. Pursestring sutures were made on the proximal end of the colon, and the anvil of the stapler was inserted into it. After replacing the colon into the abdominal cavity, the TEM resectoscope was removed and the anus was effaced using Lone-Star Retractor. We performed transanal pursestring suturing of the distal stump of the rectum using 2-0 monofilaments, because the sutured area was too short to be laparoscopically closed using an Endo GIA stapler. Then, a circular stapler was inserted transanally, and the pursestring sutures were tightened to secure the stapler in place. The anvil was attached in position and the end-to-end anastomosis was created.
-
(4)
For cases of ultra-low rectal cancer, which is approximately 2 cm within the dentate line, a circumferential, handsewn, end-to-end anastomosis was created after partial intersphincteric resection technique was performed.




Results
All 34 operations were successfully performed laparoscopically, and none of the cases required conversion to open surgery. No diverting ileostomy was created during the procedure. The average operative time was 151.6 (range, 125–185) minutes. The average blood loss was 200.2 (range, 55–450) ml. The final pathological diagnoses were carcinoma in 30 patients (pTis in 1 patients, stage I or II in 16 patients, and stage III in 13 patients), adenoma in 3 patients, and no residual tumor tissue in 1 patient, who was initially diagnosed as adenocarcinoma after local excision. All resection margins were negative (Table 2).
There was no operation-related mortality. Six patients developed postoperative anastomotic leakage; all of them had tumors in the mid or lower rectum. Among these 6 patients, 5 were among the first 17 patients on whom this surgery was performed. However, as we gained experience in performing the surgeries, the outcomes improved and among the next 17 patients who underwent surgery, only 1 patient showed postoperative anastomotic leakage. Among the patients who had anastomotic leakage, five were conservatively treated with pelvic lavage, fasting, and total parenteral nutrition for 2–6 weeks, only one patient underwent secondary ileostomy. There were no other complications in all patients. The median postoperative hospitalization was 9 (range, 7–66) days.
Discussion
Since the first laparoscopic-assisted colectomy reported by Jacobs in 1991, laparoscopic colorectal surgery has been adopted in a variety of surgical procedures, and its applications continue to develop. Several randomized, controlled trials [1–7] have shown that laparoscopic colectomy follows the same principles of radical treatment as laparotomy, namely, length of the specimen, number of lymph nodes harvested, and margins of resection. Furthermore, the long-term oncological outcome of this procedure is equivalent to that of open surgery. However, current techniques still require an additional abdominal incision to extract the specimen. This incision, although smaller than an open laparotomy incision, might reduce some advantages offered by a laparoscopic approach and increase the possibility of incision- and implantation-related complications. Creating total intracorporeal anastomosis is still a major challenge in laparoscopic colorectal surgery. The placement of the anvil of a circular stapler is particularly difficult, mainly because of the complicated procedures involved in fixing it to the proximal colonic stump [11].
Since the concept of natural orifice transluminal endoscopic surgery (NOTES) was first presented in 2004 [12], it has attracted a great deal of interest from surgeons and endoscopists [13–15] and has been anticipated to represent the next step in the evolution of minimally invasive surgery. The anus is a natural orifice that is anatomically in continuation with the colon and the rectum; thus, transanal removal of the specimen during laparoscopic colorectal procedures is an appealing concept in terms of its minimally invasive nature and its similarity to the concept of NOTES. Abdominal incision could be avoided by combining laparoscopy with transanal endoscopic microsurgery (TEM) [8, 16]. Modeled on the requirements for NOTES, the TEM device has many desirable features. It is a stable platform [17] that can help to maintain a continuous pressure-regulated pneumorectum and has a four-port multifunction back plate that allows the use of several instruments simultaneously to permit various surgical maneuvers, such as accurate dissecting and suturing in the rectal lumen up to 20 cm from the anal verge [18, 19]. Combining the laparoscopic procedure with TEM in colorectal surgery allows an optimum surgical view and a stable pneumorectum/peritoneum throughout the procedure. Above all, the operation can be performed simultaneously in the peritoneal cavity and transanally through the TEM resectoscope.
We have described a new surgical technique for total laparoscopic sigmoid and rectal surgery in combination with TEM for completion of the anastomosis created on the basis of the tumor location. After high ligation of the inferior mesenteric artery and vein, the sigmoid colon and left colon are completely mobilized for easy transanal exteriorization of the colon transanally for resection and insertion of the anvil of a circular stapler. For tumors in the sigmoid colon, if colon mobilization is not sufficient to allow transanal exteriorization, the proximal colon is transected laparoscopically and the specimen is exteriorized through the TEM resectoscope shaft. The anvil of the circular stapler is then inserted into the abdominal cavity to the proximal end of the bowel under laparoscopic guidance [10]. End-to-end anastomosis is created after closing the distal stump of the rectum. For tumors in the lower rectum, the distal stump of the rectum is too short to be closed using an Endo GIA stapler laparoscopically. In such cases, anastomosis is created first by transanal pursestring suturing of the distal stump of the rectum transanally, after which the circular stapler was inserted and held in position by tightening the pursestring sutures. We recommend creating circumferential, handsewn, end-to-end anastomosis in sphincter-preserving surgery for cases of ultra-low rectal cancer.
We encountered three main technical difficulties during the surgery: the first was with regard to complete mobilization of the sigmoid and descending colon, simultaneously ensuring adequate blood supply to the proximal colon, for easy exteriorizing of the colon for extracorporeal resection and insertion of the anvil of the circular stapler. In case of insufficient mobilization, we had to perform pursestring suturing and insert the anvil to the proximal end of the bowel under laparoscopic guidance, which increased the operation difficulty and time. The second was with regard to closure of the distal stump of the rectum and reliable completion of the anastomosis. To ensure these, we needed to set aside an adequate length of the stump of the distal rectum for closure using an Endo GIA stapler. If the closure of the distal stump of the rectum is not intact, postoperative anastomotic leakage is inevitable. According to our experience, for lower rectal tumors, it is better to pursestring sutures to the distal stump of the rectum transanally or to construct handsewn end-to-end anastomosis rather than mere stapling. The third was with regard to exteriorize the specimen through anus and avoid tumor cell seeding. To ensure these, we pack the specimen into a plastic bag and extract it through the TEM resectoscope shaft. Furthermore, in cases where specimen extraction is difficult because of large tumors, we suggest performing an additional abdominal incision to remove specimen, which can help to avoid injury by repeated extracting.
Bowel open is inevitable during this operation. Avoiding the outflow of intestinal contents and potential tumor spillage and decreasing the incidence of intraperitoneal infection are the key points for the successful completion of this procedure. To achieve these, first, adequate preoperative workup and bowel cleansing and administration of prophylactic antibiotics need to be strictly implemented. Second, an economical method of ligation of the end of the proximal bowel should be performed using hemp rope to prevent the outflow of intestinal contents and subsequent contamination of the peritoneal cavity. Third, iodine solution lavage of the abdominal and pelvic cavity should be performed after specimen retrieval. In our study group, there were no reports of postoperative intraperitoneal infection after employing these measures.
Our technique has the following advantages over conventional laparoscopic-assisted colorectal resection: (1) The specimen is exteriorized through a natural orifice. Besides the trocar sites, the patients have no additional abdominal incisions (Fig. 5), which considerably reduces surgical trauma, provides better cosmetic outcomes, and reduces incision-related complications; (2) Our surgical approach is a totally laparoscopy-guided procedure that requires no-touch probing. The specimen is extracted transanally in a specimen bag through the TEM resectoscope shaft, which ensures no tumor cell seeding on the abdominal wall and anus; (3) The distal resection margin for mid and lower rectal tumors are identified under direct visualization by using TEM, which may reduce the incidence of positive distal resection margin.

No abdominal incision after surgery
The main complication of this procedure is the high incidence of anastomotic leakage. As we gained experience in the surgical technique, we encountered only one case of anastomotic leakage in the second batch of 17 patients, which was much better than the results in the first batch of 17 patients, of which 5 showed anastomotic leakage. In addition, we observed that all anastomotic leakages developed in patients with mid or lower rectal cancer. Thus, we assume that if the stump of the distal rectum is not adequately long, it is not safe to clamp it using only an Endo GIA stapler; if the closure is not intact, postoperative anastomotic leakage is inevitable. Our overall experience showed that using laparoscopic surgery in combination with TEM, removal of sigmoid and upper rectal tumors in patients have the best outcome. In addition, the tumor diameter should not exceed 4 cm, which is the diameter of the TEM resectoscope shaft. In case of patients whose sigmoid colon is longer, it is convenient to extract the specimen using our technique and then insert the anvil of a circular stapler. While performing sphincter-preserving surgery for lower rectal cancer, the distal resection margin can be identified more accurately under direct visualization using TEM. Furthermore, in cases where the stump of the distal rectum was not adequately long, we employed transanal pursestring suturing or constructed handsewn end-to-end anastomosis, rather than attempting closure using an Endo GIA stapler. Additionally, when the situation required it, we performed a diverting ileostomy via the port on the upper right abdomen as a means to offset the impact of anastomotic leakage.
Patient safety should be a prime focus in our endeavor to develop new surgical techniques for scarless colectomies by combining laparoscopy with TEM. The preliminary evaluation of the results of our study shows that our technique, which represents a surgical advancement by amalgamating the concept of NOTES with laparoscopic techniques, is safe and feasible with no notable increase in operative difficulty. However, we have not assessed the long-term oncologic implications and functional outcomes. Among the many advantages of this technique, improved cosmetic outcome is noteworthy. We believe that further advancements in this technique may enable more patients to benefit from this minimally invasive surgery.
References
Lacy AM, Delgado S, Castells A et al (2008) The long-term results of a randomized clinical trial of laparoscopy assisted versus open surgery for colon cancer. Ann Surg 248:1–7
Faiz O, Warusavitarne J, Bottle A et al (2009) Laparoscopically assisted vs open elective colonic and rectal resection: a comparison of outcomes in English National Health Service Trusts between 1996 and 2006. Dis Colon Rectum 52:1695–1704
Breukink SO, Grond AJ, Pierie JP et al (2005) Laparoscopic vs open total mesorectal excision for rectal cancer: an evaluation of the mesorectum’s macroscopic quality. Surg Endosc 19:307–310
Bonjer HJ, Hop WC, Nelson H et al (2007) Laparoscopically assisted vs. open colectomy for colon cancer: a meta-analysis. Arch Surg 142:298–303
Jayne DG, Guillou PJ, Thorpe H et al (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC trial group. J Clin Oncol 25:3061–3068
The Clinical Outcome of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Eng J Med 350:2050–2059
Guillou PJ, Quirke P, Thorpe H et al (2005) Short-term end points of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASSICC trial): multicentre randomized controlled trial. Lancet 356:1718–1726
Cheung HY, Leung AL, Chung CC et al (2009) Endo-laparoscopic colectomy without mini-laparotomy for left-sided colonic tumors. World J Surg 33:1287–1291
Leroy J, Costantino F, Cahill RA et al (2011) Laparoscopic resection with transanal specimen extraction for sigmoid diverticulitis. Br J Surg 98:1327–1334
Lacy AM, Delgado S, Rojas OA et al (2008) MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc 22:1717–1723
Akamatsu H, Omori T, Oyama T et al (2009) Totally laparoscopic low anterior resection for lower rectal cancer: combination of a new technique for intracorporeal anastomosis with prolapsing technique. Dig Surg 26:446–450
Kalloo AN, Singh VK, Jagannath SB et al (2004) Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc 60:114–117
Kantsevoy SV, Jagannath SB, Niiyama H et al (2005) Endoscopic gastrojejunostomy with survival in a porcine model. Gastrointest Endosc 62:287–292
Merrifield BF, Wagh MS, Thompson CC (2006) Peroral transgastric organ resection: a feasibility study in pigs. Gastrointest Endosc 63:693–697
Wagh MS, Merrifield BF, Thompson CC (2005) Endoscopic transgastric abdominal exploration and organ resection: initial experience in a porcine model. Clin Gastroenterol Hepatol 3:892–896
Sylla P, Sohn DK, Cizginer S et al (2010) Survival study of natural orifice translumenal endoscopic surgery for rectosigmoid resection using transanal endoscopic microsurgery with or without transgastric endoscopic assistance in a swine model. Surg Endosc 24:2022–2030
Whiteford MH, Denk PM, Swanstrom LL (2007) Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc 21:1870–1874
Papagrigoriadis S (2006) Transanal endoscopic micro-surgery (TEMS) for the management of large or sessile rectal adenomas: a review of the technique and indications. Int Semin Surg Oncol 3:13–16
Maslekar S, Beral DL, White TJ et al (2006) Transanal endoscopic microsurgery: where are we now? Dig Surg 223:12–22
Acknowledgments
The authors thank Dr. Xing-Sheng Lu, Dr. Li-Gong Tang, Dr. Nian Liu, Ms. Zhi-Li Hua, and Ms. Xue-Lei Wu for their participation in the operation.
Disclosures
The paper has not been published previously and all authors have nothing to disclose for corporate or commercial relationships. Drs. Yi Han, Yong-Gang He, Hao-Bo Zhang, Ke-Zhi Lv, Ya-Jie Zhang, Mou-Bin Lin, and Lu Yin have no conflict of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
All authors participate in drafting the article or revising it critically for important intellectual content and give final approval of the version to be published.
Rights and permissions
About this article
Cite this article
Han, Y., He, YG., Zhang, HB. et al. Total laparoscopic sigmoid and rectal surgery in combination with transanal endoscopic microsurgery: a preliminary evaluation in China. Surg Endosc 27, 518–524 (2013). https://doi.org/10.1007/s00464-012-2471-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2471-5