
Abstract
Background
Obesity, steroid-induced diabetes, hypercholesterolemia, and steatohepatitis can occur after liver transplantation and may respond to bariatric surgery. The safety and feasibility of bariatric surgery after liver transplantation is unknown.
Methods
Nine morbidly obese patients with prior liver transplants underwent sleeve gastrectomy in a pilot program. Sleeve gastrectomy was chosen over gastric banding to avoid foreign body implantation, and over gastric bypass to maintain endoscopic access to the biliary system and reduce surgical complexity. We reviewed patient demographics, operative details, 30-day complications, weight loss, postoperative hepatic and renal functions, and resolution of comorbidities.
Results
Sleeve gastrectomy was performed laparoscopically in eight patients and as an open procedure in one patient. The mean operative time was 165 min and mean postoperative length of stay was 5 days. Follow-up ranged from 3 to 36 months. In the first 30 days, there were three complications in three patients: mesh dehiscence after a synchronous incisional hernia repair, bile leak from the liver surface requiring laparoscopic drainage, and postoperative dysphagia that required reoperation. Calcineurin inhibitor levels and hepatic and renal functions remained stable. There were no episodes of graft rejection. At 3 months liver function tests remained stable. Excess weight loss averaged 55.5 % at 6 months.
Conclusion
Sleeve gastrectomy is technically feasible after liver transplantation and resulted in weight loss without adversely affecting graft function and immunosuppression. Early complications may be more frequent as a result of adhesions of the left upper quadrant. Late complications were rare.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Morbid obesity is an epidemic plaguing the United States, in which nearly one third of the population meets the criteria for obesity [1]. The liver transplant population is not exempt from this problem. In one study, 54 % of patients undergoing orthotopic liver transplant were either overweight or obese [body mass index (BMI) >25 kg/m2] [2]. Seven percent of patients who received liver transplant are considered to be severely or morbidly obese (BMI >35 kg/m2). Weight gain after solid organ trasnplantation occurs because of steroid-containing immunosuppression and physical inactivity from decreased exercise tolerance [3].
Data regarding obesity and its impact on liver transplant outcomes is limited. Recent studies suggest that obesity does not affect patient and graft survival after liver transplantation [4]. However, obesity has been shown to increase the surgical morbidity, including wound infections, wound dehiscence, and hernias after transplantation [5]. More significantly, excess pretransplant body weight hinders the rate of improvement in health-related quality of life after liver transplantation [6].
One possible approach for treating obesity after a liver transplant is to use bariatric surgery. Currently, bariatric surgery is established as the most effective means for both weight loss and resolution of metabolic disease in the morbidly obese. However, its applicability to liver transplant recipients has not been established; only sporadic case reports have been published [7]. Risks of bariatric surgery in this population include (1) adhesions in the left upper quadrant as a result of previous surgery, (2) concern for infection and poor healing as a result of immunosuppression, and (3) potential for graft rejection or loss as a result of unpredictable immunosuppression pharmacokinetics and absorption. We sought to determine the feasibility and outcome of sleeve gastrectomy in patients who have undergone a liver transplant.
Methods
We conducted a pilot trial of nine liver transplant patients who underwent sleeve gastrectomy between August 2007 and August 2011 and reviewed outcomes. All patients were referred by their hepatologists or primary-care physicians to the UCSF Bariatric Surgery Program for management of morbid obesity after conservative management failed. Morbid obesity was defined as having grade III obesity (BMI > 40 kg/m2) or grade II obesity with comorbidities (BMI > 35 kg/m2). All patients met the 1991 National Institutes of Health (NIH) Consensus Development Conference Guidelines for weight loss surgery. During this period, one attending surgeon (AMP) performed eight laparoscopic sleeve gastrectomies and one open sleeve gastrectomy in morbidly obese liver transplant recipients.
Sleeve gastrectomy was performed by mobilizing the greater gastric curvature starting 5 cm proximal to the pylorus and continuing to the left crus using a LigaSure™ device (Covidien, Mansfield, MA) to divide the gastroepiploic branches and short gastric vessels. A bougie (size range = 36–44 Fr) was inserted and the stomach was sleeved using 4.8-mm Duet staple cartridges (Covidien) along the bougie. The separated stomach along the greater curvature was extracted and the remnant stomach was anchored to the greater omentum with interrupted sutures to prevent stomach torsion. Orogastric methylene blue was used to test for gastric leaks and a drain was placed near the staple line. All patients were extubated in the operating room and underwent an upper gastrointestinal series on postoperative day 1. Afterward, a bariatric clear liquid diet was started. All patients had follow-up in the bariatric clinic at 2 weeks, 4 weeks, every 3 months for the first 2 years, and every 6 months thereafter. Each patient had separate transplant clinic appointments for continuous surveillance of their liver.
We reviewed patient demographics, preoperative and surveillance laboratory data, operative details, percentage of excess weight loss (% EWL), morbidity, and mortality. Laboratory data included measurements of serum levels of tacrolimus since the absorption of this drug can potentially be affected by gastrointestinal surgery, and maintenance of stable levels is important in preventing rejection and avoiding tacrolimus-related nephrotoxicity. In addition, liver function tests were measured on a regular basis to monitor graft function and detect possible graft rejection. Paired t tests were calculated for preoperative and postoperative laboratory values.
Results
Clinical characteristics of patients
Of the nine patients studied (Table 1), eight underwent laparoscopic sleeve gastrectomy and one had an open procedure. The mean pretransplant BMI was 29 kg/m2. Eight patients had prior liver transplants and one had a liver and a kidney transplant. Before transplantation, four of the nine patients (44 %) were either overweight or morbidly obese class I based on NIH criteria. The mean time between liver transplantation to sleeve gastrectomy was 5.9 ± 2.4 years. The mean BMI prior to sleeve gastrectomy was 41 ± 3 kg/m2 and six patients were morbidly obese (BMI > 40 kg/m2). All patients underwent intraoperative lysis of adhesions, five had concurrent liver biopsies, and two also had incisional hernia repairs with mesh. All patients had at least two or more obesity-related comorbidities (Table 1). The mean operative time was 165 ± 68 min and the length of stay in the hospital averaged 5.3 ± 3.8 days.
Complications
There were three complications in three different patients within the first 30 days and all required reoperation. One patient had developed an incisional hernia after his liver transplant and underwent an open sleeve gastrectomy together with a hernia repair using mesh. An open approach was used because of the large size of the hernia (20 × 30 cm). On postoperative day 2, the hernia recurred and the patient underwent a revisional repair and replacement of the mesh. The patient subsequently did well.
Another patient had two prior liver transplants and developed a bile leak on postoperative day 1. Diagnostic laparoscopy showed an injury to the medial edge of the left lateral segment causing a biliary leak from the liver surface. This was treated with argon beam coagulation and drainage. The patient recovered uneventfully.
The third patient developed dysphagia to both solid and liquids postoperatively. An upper gastrointestinal series demonstrated delayed esophageal emptying. An upper endoscopy demonstrated no anatomical deformities and two attempts at dilation of the lower esophageal sphincter (LES) and sleeve failed. Manometry demonstrated aperistalsis. The patient required parenteral nutrition, and 6 weeks after her sleeve gastrectomy she underwent conversion to laparoscopic Roux-en-Y esophagojejunostomy. She has done well since her corrective surgery.
Weight loss and laboratory findings
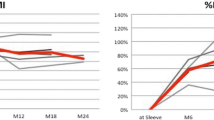
The mean excess body weight loss (EWL) was 38 % for all nine patients at 3 months. There was a trend toward continued weight loss 1 year after sleeve gastrectomy (Fig. 1). Calcineurin inhibitor levels and drug dosages remained stable, as did hepatic and renal functions for the duration of the study (Table 2).

Graph depicting mean percentage of excess body weight loss in liver transplant patients who underwent sleeve gastrectomy
Discussion
The obesity epidemic has already had an impact on liver transplantation. The proportion of liver transplant recipients classified as obese increased from 15 % in the early 1990s to just over 25 % since 2002 [8]. Although the increase in general perioperative morbidity and mortality among obese patients due to its adverse effects on all organ systems is well documented [9], data regarding obesity and its impact on liver transplant outcomes is limited. Recent studies suggest that obesity does not affect patient and graft survival after liver transplantation [4]. However, obesity does have a detrimental effect on the health-related quality of life and exacerbates obesity-related comorbidities after liver transplantation.
After solid organ transplantation, patients tend to gain weight because of immunosuppressant drugs and physical inactivity from a decrease in exercise tolerance [3]. Immunosuppressants like calcineurin inhibitors (such as cyclosporine and tacrolimus) and steroids can exacerbate obesity-related comorbidities such as hypertension, diabetes, and dyslipidemia. Metabolic syndrome occurs in 59 % of patients after liver transplantation and can decrease graft function [3]. It also costs more to take care of morbidly obese patients after transplant and their long-term survival is decreased [9].
Bariatric surgery is a potential option for losing weight and decreasing the effects of metabolic syndrome and thereby increasing the durability of transplanted organs. Recently, sleeve gastrectomy has been shown to be safe and effective for morbidly obese patients who seek an alternative to gastric bypass or gastric banding. In recent studies, sleeve gastrectomy was shown to improve metabolic syndrome and result in a >70 % excess body weight loss at 2 years after the procedure [10].
We previously showed that laparoscopic gastric bypass in patients with end-stage renal disease and laparoscopic sleeve gastrectomy in patients with cirrhosis or end-stage renal disease are safe and well-tolerated and improve the patient’s candidacy for transplantation [11]. The data regarding safety and feasibility of bariatric surgery after liver transplantation is scarce. Both gastric bypass and gastric banding have been described as technically feasible [12, 13]. Several challenges exist for considering bariatric surgery in this population. First, bariatric surgery requires mobilization of the left lobe of the liver, and adhesions from the previous transplant can be tenacious. Second, postoperative complications may have more severe sequelae due to prolonged wound healing and risk of infections associated with immunosuppression. Finally, there is concern about changes in the absorption of immunosuppressive medications and the resultant impact on graft function.
Our study showed that laparoscopic sleeve gastrectomy was feasible and resulted in weight loss and metabolic benefits. Patients lost nearly 40 % of their excess body weight by 3 months. The three patients who reached 1 year of follow-up lost 65 % of their excess body weight, which is comparable to that of bariatric patients without prior solid organ transplant [10]. There was resolution of diabetes despite steroid-based immunosuppression. There was no difficulty in maintaining immunosuppression, no need for dose escalation of calcineurin inhibitors, and no episodes of acute rejection. However, three patients had early complications after sleeve gastrectomy and all three required reoperation. Complications may have been more frequent because of the patients’ underlying disease and previous surgical procedures.
Limitations of this pilot study are its small size and short follow-up, and more patients with longer follow-up are needed to determine the safety and efficacy of bariatric surgery in this population. Yet, given the recent widespread interest in bariatric surgery for morbidly obese patients after solid organ transplantation, we wanted to report our early experience in order to help guide others interested in this approach.
Sleeve gastrectomy is an attractive option for liver transplant recipients because it preserves endoscopic access to the biliary tree and duodenum, an important consideration because an estimated 12–30 % liver transplant patients will require future endoscopic intervention related to their transplanted organ [14]. Sleeve gastrectomy is less technically challenging and takes less time than gastric bypass because there is no need to create a Roux limb or build a second Roux if one was already created for the liver transplant. Finally, sleeve gastrectomy may be less likely than gastric bypass to cause malabsorption of nutrients and immunosuppressive medications. Although laparoscopic gastric banding is technically easier than a sleeve gastrectomy, we were concerned about placing a foreign body and the frequent adjustments in this immunosuppressed population.
We conclude that laparoscopic sleeve gastrectomy after liver transplantation can provide weight loss and metabolic benefit without adversely affecting graft function or immunosuppression. While early technical complications were more common, late complications were rare, and weight loss was similar to that seen in nontransplant patients. Based upon this pilot study, laparoscopic bariatric surgery after solid organ transplant is feasible and warrants further investigation. Larger series of patients and long-term follow-up are needed to determine if weight loss is sustainable and offers long-term benefit.
References
Youfa W, Beydoun M (2007) The obesity epidemic in the United States––gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev 29(1):6–28
2010 Annual Report of the US Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1994–2009. Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Rockville, MD; United Network for Organ Sharing, Richmond, VA; University Renal Research and Education Association, Ann Arbor, MI
Laish I, Braun M, Mor E, Sulkes J, Harif Y, Ben AZ (2011) Metabolic syndrome in liver transplant recipients: prevalence, risk factors, and association with cardiovascular events. Liver Transpl 17:15–22
Leonard J, Heimbach JK, Mlinchoc M, Watt K, Charlton M (2008) The impact of obesity on long-term outcomes in liver transplant recipients––results of the NIDDK liver transplant database. Am J Transplant 8(3):667–672
Schaeffer DF, Yoshida EM, Buczkowski AK, Chung SW, Steinbrech UP, Erb SE, Scudamore CH (2009) Surgical morbidity in severely obese liver transplant recipients––a single Canadian centre experience. Ann Hepatol 8(1):38–40
Zaydfudim V, Feurer I, Moore D, Wisawatapnimit P, Wright JK, Pinson CW (2009) The negative effect of pretransplant overweight and obesity on the rate of improvement in physical quality of life after liver transplantation. Surgery 146(2):174–180
Butte JM, Devaud N, Jarufe N, Boza C, Perez G, Torres J, Perez-Ayuso RM, Arrese M, Martinez J (2007) Sleeve gastrectomy as treatment for severe obesity after orthotopic liver transplantation. Obes Surg 17(11):1517–1519
Charlton M (2009) Obesity, hyperlipidemia, and metabolic syndrome. Liver Transpl 15(Suppl 2):S83–S89
Choban P, Flancbaum L (1997) The impact of obesity on surgical outcomes: a review. J Am Coll Surg 185:593–603
Himpens J, Dapri G, Cadiere GB (2006) A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg 16:1430–1436
Takata MC, Campos GM, Ciovica R, Rabl C, Rogers SJ, Cello JP, Ascher NL, Posselt AM (2008) Laparoscopic bariatric surgery improves candidacy in morbidly obese patients awaiting transplantation. Surg Obes Relat Dis 4(2):159–164; discussion 164–165
Chopra A, Chao E, Etkin Y, Merklinger L, Lieb J, Delany H (2012) Laparoscopic sleeve gastrectomy for obesity: can it be considered a definitive procedure? Surg Endosc 26(3):831–837
Tichansky D, Madan A (2005) Laparoscopic Roux-en-Y gastric bypass is safe and feasible after orthotopic liver transplantation. Obes Surg 15:1481–1486
Sherman S, Shaked A, Cryer HM, Goldstein LI, Busuttil RW (1993) Endoscopic management of biliary fistulas complicating liver transplantation and other hepatobiliary operations. Ann Surg 218(2):167–175
Acknowledgments
The authors thank Pamela Derish for her editing.
Disclosures
Matthew Y. C. Lin, Ankit Sarin, M. Mehdi Tavakol, Shadee M. Amirikiai, Stanley J. Rogers, Jonathan T. Carter, and Andrew M. Posselt have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the SAGES 2012 Annual Meeting, March 7–March 10, 2012, San Diego, CA.
Rights and permissions
About this article
Cite this article
Lin, M.Y.C., Tavakol, M.M., Sarin, A. et al. Safety and feasibility of sleeve gastrectomy in morbidly obese patients following liver transplantation. Surg Endosc 27, 81–85 (2013). https://doi.org/10.1007/s00464-012-2410-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2410-5