
Abstract
Background
A thoracoabdominal esophagectomy for esophageal cancer is a severely invasive procedure. A thoracoscopic esophagectomy may minimize injury to the chest wall and reduce surgical invasiveness. Conventional thoracoscopic procedures are performed in the left lateral-decubitus position. Recently, procedures performed in the prone position have received more attention because of improvements in operative exposure or surgeon ergonomics. However, the efficacy of the prone position in an aggressive thoracoscopic esophagectomy with an extensive lymphadenectomy has not been fully documented.
Methods
We successfully performed a thoracoscopic esophagectomy with a three-field extensive lymphadenectomy in 43 esophageal carcinoma patients in the prone position from December 2007 to December 2009. We describe our procedures with the patients in the prone position, focusing especially on a lymphadenectomy along the left recurrent laryngeal nerve where the nodes are frequently involved and precise dissection is technically challenging. To determine further the advantages of this position, we retrospectively compared surgical outcomes in 43 patients to those of 34 patients who underwent a thoracoscopic esophagectomy in the left lateral decubitus position as a historical control from January 2006 to November 2007.
Results
It was easier to explore the operative field around the left recurrent laryngeal nerve during a thoracoscopic esophagectomy in the prone position. The mean duration of the aggressive thoracoscopic procedure in the prone position was 307 min, which was significantly longer than in the left lateral decubitus position, but the total estimated blood loss in the prone position was significantly lower. There was no difference in the incidence of postoperative complications between the two procedures.
Conclusions
A thoracoscopic esophagectomy in the prone position is technically safe and feasible and provides better surgeon ergonomics and better operative exposure around the left recurrent laryngeal nerve during an aggressive esophagectomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
A standard procedure for surgically curable thoracic esophageal cancer has high operative morbidity and mortality rates because of extreme invasiveness involving extensive dissection of lymph nodes [1–3]. A thoracoscopic esophagectomy may minimize injury to the chest wall and reduce the surgical invasiveness, and there have been several reports of its feasibility and curability [4–12]. This procedure is traditionally performed in the left lateral decubitus position, but recently the advantages of a thoracoscopic esophagectomy in the prone position have been reported [13–15]. Compared to the left lateral decubitus position, better operative exposure, improved surgeon ergonomics, shorter operative time, and less blood loss have been demonstrated in the prone position [16]. However, the potential benefits of the prone position during minimally invasive but aggressive esophagectomy accompanied with extensive lymphadenectomy are not fully documented.
We introduced a thoracoscopic esophagectomy in the left lateral decubitus position to reduce surgical invasiveness and accelerate early recovery [17] and have recently developed the procedure with the patient in the prone position to obtain better operative exposure and surgeon ergonomics. Lymph nodes along the recurrent laryngeal nerves are thought to be highly involved by carcinoma cells as well as a main lymphatic chain to the neck, and complete dissection of these nodes is recommended [1, 18–22]. However, a lymphadenectomy, especially along the left recurrent laryngeal nerve during a thoracoscopic esophagectomy, is thought to be a burdensome step because of difficult operative exploration at the left upper mediastinum. To achieve a meticulous dissection of this portion, stable operative views and technical feasibility are necessary. We herein present our procedure of a lymphadenectomy along the left laryngeal nerve by performing a thoracoscopic esophagectomy in the prone position, and retrospectively review the advantages of this procedure in the prone position compared with those of the left lateral decubitus position.
Methods
Patients
We reviewed the records of 95 consecutive patients with potentially curable thoracic esophageal cancer who were candidates for a thoracoscopic esophagectomy at our institute and an affiliated one from January 2006 to December 2009. From January 2006 to November 2007, 42 patients were treated in the left lateral decubitus position (LLDP group), and from December 2007 to December 2009, 53 patients were treated in the prone position (PP group). Distant metastasis, multiorgan involvement, enlarged and fixed cervical lymph nodes, and suggestive celiac lymph node metastasis on computed tomography or FDG-PET scan findings were considered indications of incurable disease. Contraindications for a thoracoscopic esophagectomy were tumor infiltration into other structures; impaired circulatory or pulmonary function prohibiting single-lung ventilation; a concomitant serious medical disorder such as severe diabetes mellitus, chronic renal failure, or liver cirrhosis; and patient refusal to undergo thoracoscopic surgery. Tumors were staged according to the TNM classification system of the American Joint Committee on Cancer and the Union Internationale Contre le Cancer. Twenty patients underwent chemoradiation therapy or chemotherapy before surgery for T3 and bulky N1 or T3 N2 tumors. The abdominal portion of the procedure was performed laparoscopically in all but five patients who had had previous serious abdominal surgery (i.e., 2 in the PP group and 3 in the LLDP group). An alimentary tract was reconstructed using a gastric conduit in all patients except two who had had a previous gastrectomy (i.e., one in each group who underwent a small or large intestinal reconstruction). All surgeries were performed or supervised by a single senior surgeon (NH). The patients were fully involved in the decision-making process, and informed consent was obtained from all patients. All patients who had undergone a thoracoscopic esophagectomy had a scheduled enhanced computer tomographic examination every 3 or 6 months after surgery to determine the prevalence and location of local-regional recurrence. This retrospective study was approved by the Institutional Review Board of Saga University Hospital.
Thoracoscopic procedures in a prone position
Under a combination of epidural and general anesthesia and using a double-lumen endotracheal tube for single-lung ventilation, the patient was initially placed in a prone position. The right arm only was raised cranially to expose the right axillar fossa. The face was placed toward the right to facilitate suction of the sputa by bronchial scope and to avoid increasing ophthalmic pressure. All surgeons stood on the right chest side of the patient, and a high-quality video monitor was set up on the opposite side (Fig. 1). A 12-mm blunt trocar was inserted into the fifth intercostal space (ICS) on the posterior axillary line, carefully confirming the absence of pleural adhesion. Another three trocars were inserted under thoracoscopic control: a 12-mm trocar in the third ICS behind the midaxillary line, a 5-mm trocar in the seventh ICS behind the posterior axillary line, a 12-mm trocar in the ninth ICS on the scapular angle line for the thoracoscope, and, if needed, a 5-mm trocar in the seventh ICS on the scapular angle line (Fig. 1). Carbon dioxide pneumothorax was achieved at a pressure of 6 mmHg to collapse the right lung and to expand the mediastinum. Procedures in the prone position were basically the same as those in thoracoscopic procedures in the left lateral decubitus position previously described [17]. The surgeon used a grasper in the left hand and a monopolar electrocautery, ultrasound-activated device (SonoSurg X, Olympus, Tokyo) or tissue-fusion system (Ligasure V, Covidien, Norwalk, CT, USA) in the right hand. The surgeon began by opening the mediastinal pleura overlying the anterior aspect of the esophagus. The arch of the azygos vein was then divided and the right bronchial artery was carefully preserved. The lymph nodes around the right recurrent laryngeal nerve could be dissected nearly below the thyroid gland. The thoracic duct was divided in preparation for attachment to the esophagus. The pulmonary branches of the vagus nerves were preserved and the esophagocardial branches were divided. The upper esophagus was mobilized circumferentially, and the esophagus was divided at the level of the aortic arch by linear stapling (ETS flex 45–4.8, Ethicon, Somerville, NJ, USA) to facilitate lymph node dissection on the left aspect of the esophagus.

Position of the patient, surgeons, and video monitors, and sites of the four trocars. Roman numerals show the rib number. MA midaxillary line, PA posterior axillary line
Dissection along the left recurrent laryngeal nerve
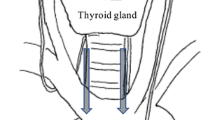
Before dissection along the left recurrent laryngeal nerve, subcarinal nodes and nodes below the right bronchus were dissected, and the preserved right bronchial artery was extended by the division of the branch of the third intercostal artery to a point that allowed good visualization of the left aspect of the trachea and the area below the aortic arch. During the procedure, a main cuff of a double-lumen endotracheal tube was deflated temporarily and the trachea was rolled back carefully and strongly to the right and ventrally by a grasper holding small gauze to explore the left aspect of the trachea and the left bronchus (Fig. 2). First, the divided esophagus on the oral side was released from the trachea toward the neck to allow for a sufficient number of lymph nodes up to the thoracic inlet to be dissected. Next, the tissue, including the left recurrent laryngeal nerve and lymph nodes, was dissected sharply just along the trachea and the left bronchus to make the ventral border of dissection. The posterior aspect, which was the left border of dissection, was dissected on a vascular sheath of the dense connective tissue covering the aortic arch and the left subclavicular artery. This vascular sheath is supposed to be developed to the pericardium around the heart. This dense connective tissue includes a couple of superior cardiac branches of the sympathetic nerve system that arise at the neck and run down along the left subclavicular artery (Fig. 3). Some esophageal or tracheal branches of the identified left recurrent laryngeal nerve were divided, and the thoracic duct was also divided at the thoracic inlet. Finally, the left recurrent laryngeal nerve was sharply isolated from the explored tissue without using an electric device to avoid injury by electricity or heat, and lymph nodes were consequently dissected in an en-bloc fashion accompanied with the divided thoracic duct. At the vertebral side of the posterior aspect of this dissection, the vascular sheath covering the aortic arch and the left subclavicular artery was prepared with the divided esophagus on the descending aorta at the posterior face (Fig. 3). During dissection below the aortic arch, the recurrent portion of the left recurrent laryngeal nerve, left vagus nerve, and one or two left bronchial arteries were identified and preserved on the face of the trunk of the pulmonary artery.

A schematic drawing of the exploration around the left recurrent laryngeal nerve and dissection along the left recurrent laryngeal nerve preserving the cardiac branches within the vascular sheath of the left subclavicular artery and the aortic arch. The curved arrow shows the trachea rolled back by a grasper with small gauze. The straight arrows show the dissected borders around the left recurrent laryngeal nerve. CB cardiac branches, LNs lymph nodes, LRLN left recurrent laryngeal nerve, LSA left subclavicular artery, T trachea, VS vascular sheath

The superb visualization and a magnified view provided by the thoracoscope in the prone position around the left aspect of the trachea and the area below the aortic arch. LRLN left recurrent laryngeal nerve, T trachea, LSA left subclavicular artery, CB cardiac branches, AA aortic arch
By dissecting the esophagus below the main bronchi, a proper dissecting plane was created; the pericardium, left pleura, descending aorta, and diaphragm were maintained to perform sufficient paraesophageal, middle, and lower posterior mediastinal and supradiaphragmatic lymph node dissection.
After the thoracoscopic procedures were completed, a single 28Fr chest tube or a 19Fr Blake drain (Ethicon) was inserted. The patient was placed in the supine position and then underwent the laparoscopic abdominal procedure. The double-lumen endotracheal tube was changed to a standard single-lumen endotracheal tube. The stomach was mobilized accompanied by dissection of abdominal lymph nodes; a gastric conduit was then created extracorporeally through the small laparotomy incision. The reconstruction of an alimentary tract was done at the neck between the cervical esophagus and a gastric conduit pulled up through the posterior mediastinum. A pyloroplasty was not performed and no feeding jejunostomy tube was placed.
Statistical analysis
We determined the advantages of thoracoscopic esophagectomy in the prone position compared to those of the left lateral decubitus position. To determine whether an adequate operative exposure around the left recurrent laryngeal nerve was obtained, we confirmed that there was adequate identification and exploration of the left subclavicular artery from the aortic arch to the thoracic inlet, which overlies the posterior aspect of the dissection, by reviewing the medical charts and the video recordings of all thoracoscopic procedures. As clinical data, we obtained the following information from medical charts: age; sex; concurrent illness; tumor characteristics; total and thoracic operation times; total estimated blood loss; number of retrieved total nodes, mediastinal nodes, and nodes along the left recurrent laryngeal nerve; and incidence of recurrent nerve palsy and respiratory complications. If a patient had hoarseness, then otolaryngologists were consulted to determine whether recurrent laryngeal nerve palsy was present. Respiratory complications were defined in this study as a fever over 38°C, with radiographic evidence of pulmonary infiltration, prolonged ventilation over 5 days, or new use of a bronchodilator. The values are expressed as the mean ± standard deviation (SD). Differences between the groups were analyzed by Student’s t test or the χ2 test using Fisher’s exact probability [23]. A two-sided p value of less than 0.05 was considered to be statistically significant.
Results
During the study period, there was no patient who initially was proposed to be a candidate for an open thoracotomic esophagectomy. The thoracoscopic procedure in the prone position was completed in all 53 patients with no conversions to a conventional thoracotomy or thoracoscopic surgery by the left lateral decubitus position. Ten patients who underwent a thoracoscopic esophagectomy in the prone position were excluded from this study for the following the reasons: Eight patients of the original 53 had a limited two-field lymph node dissection due to the superficial spread of carcinoma that was preoperatively diagnosed as a T1a tumor located in the lower third of the esophagus. Another patient had an incurable T4 tumor that had been diagnosed preoperatively as a resectable T3 tumor and consequently underwent a palliative resection. One patient had concomitant pharyngeal cancer and underwent a pharyngolaryngectomy in addition to a radical esophagectomy for esophageal cancer.
From January 2006 to November 2007, 42 patients underwent a thoracoscopic esophagectomy in the left lateral decubitus position for preoperatively curable esophageal cancer. Eight of these patients were excluded from the present study. In 2 of 42 patients, the thoracoscopic procedure was converted to a conventional open thoracotomy: one because of dense pleural adhesion derived from previous surgery for lung cancer and the other because of intraoperative bleeding from the left inferior pulmonary vein. In this group, there was one patient with an incurable T4 tumor and one patient with concomitant pharyngeal cancer. Four patients had a two-field lymph node dissection because of the superficial carcinoma preoperatively diagnosed as T1a tumor in the lower esophagus.
Consequently, 43 patients enrolled in this study underwent a thoracoscopic esophagectomy in the prone position (PP group) and 34 underwent a thoracoscopic esophagectomy in the left lateral decubitus position (the LLDP group). Patient and tumor characteristics are listed in Table 1. There was no significant difference between the two groups in age, gender, location of tumor, or staging. All 43 patients in the PP group had a preoperative histological diagnosis of esophageal squamous cell carcinoma, but there were 3 patients with adenocarcinoma in the LLDP group. Twelve patients (28%) in the PP group and 7 patients (16%) in the LLDP group underwent preoperative chemotherapy using a combination of cisplatin and 5-fluorouracil, and 1 patient in the PP group had preoperative radiation therapy of 34 Gy in addition to chemotherapy. Proximal and distal surgical margins were free from carcinoma cells in all patients in both groups, according to macroscopic and microscopic examinations. Lymph node metastasis was identified in 26 (60%) of the 43 patients in the PP group and in 18 (53%) of the 34 patients in the LLPG group. The duration of the thoracoscopic procedure was significantly longer in the PP group than in the LLDP group (307 ± 66 min vs. 272 ± 58 min, p = 0.01 respectively), as shown in Table 2. Estimated blood loss in the PP group was 142 ± 87 g, which was significantly lower than that in the LLDP group (295 ± 416 g, p = 0.045). The number of dissected and retrieved lymph nodes in the thoracoscopic procedure was 27.0 ± 9.1 in the PP group and 26.8 ± 11.0 in the LLDP group (p = 0.439). The operative field around the left recurrent laryngeal nerve was carefully explored in the PP group (Fig. 3). Identification of the left subclavicular artery was achieved in all of 43 patients (100%) in the PP group and in 28 of 34 patients (82%) in the LLDP group (p < 0.0001). Further adequate identification and exploration of the left subclavicular artery to allow sufficient lymph node dissection around the left recurrent laryngeal nerve was obtained in 41 of 43 patients (95%) in the PP group compared to only 22 of 34 patients (65%) in the LLDP group (p = 0.007). The number of lymph nodes along the left recurrent laryngeal nerve was counted in the en-bloc excised specimen from the tracheobronchial node below the aortic arch to the nodes at the cervical side attached to the left recurrent laryngeal nerve as long as it could be dissected thoracoscopically. The number of dissected and retrieved lymph nodes along the left recurrent nerve was 6.1 ± 3.9 in the PP group and 5.4 ± 5.0 in the LLDP group (p = 0.556) (Table 2).
Intraoperative complications, other than conversion of the thoracoscopic procedure to conventional open thoracotomy in two patients in the LLDP group, were observed in one patient in the PP group who had an injury to the right inferior pulmonary vein. We were able to grasp the bleeding point just before a massive hemorrhage and the injury was closed successfully by suturing. Operative mortality was observed in one patient in the PP group; the patient died suddenly on postoperative day 8 from a serious hemorrhaging into the thorax and gastric conduit from the esophagogastrostomy. Postoperative complications developed in 15 of the 43 patients in the PP group (35%) and in 12 of the 34 patients of the LLDP group (35%) (Table 3). Respiratory complications were observed in 5 (12%) of the 43 patients of the PP group and in 5 (15%) of the 34 patients of the LLDP group; there was no significant difference in the incidence of respiratory complications between the two groups. Postoperative hoarseness and palsy of the left recurrent laryngeal nerve was observed in 6 patients (14%) in the PP group and in 6 patients (18%) in the LLDP group; there was no significant difference in postoperative hoarseness or left recurrent nerve palsy between the two groups. There were two patients with right recurrent laryngeal nerve palsy in the LLDP group. One also had left nerve palsy and underwent a temporary tracheotomy. All 12 patients, except for one in the LLDP group, recovered from hoarseness and recurrent laryngeal nerve palsy within 6 months. During a median follow-up period of 22 months after surgery, primary local recurrence along the left recurrent laryngeal nerve has not been observed.
Discussion
To minimize morbidity and mortality after an esophagectomy, a thoracoscopic esophagectomy was introduced as a minimally invasive option [4, 5], with the same survival benefit as conventional open esophagectomy [6–12]. The thoracoscopic procedure is most commonly performed with the patient in the left lateral decubitus position. Cuschieri et al. [24] demonstrated the thoracic portion of this procedure performed in the prone position in six patients in 1994. However, their procedure was not widely adopted until 2006. Recently, Palanivelu [13] reported his experience with 130 patients treated by thoracoscopic esophagectomy in the prone position and stimulated new interest in this approach. Fabian et al. [16] suggested potential benefits compared to those of the procedure in the left lateral-decubitus position. The authors reported increased operative exposure, improved surgeon ergonomics, and less operative time. Conversely, an aggressive esophagectomy with an extended three-field rather than two-field lymphadenectomy for thoracic esophageal cancer is thought to be beneficial for survival after surgery, mainly among Eastern surgeons [1, 25, 26], even though the efficacy of a three-field lymphadenectomy has not been proven by well-designed, prospective, randomized control trials [18, 19]. Akiyama et al. [1] emphasized that the recurrent laryngeal nerve lymphatic chains were of utmost importance for possible nodal metastases because of a high frequency of tumor spread of over 30% wherever the primary cancer was located in the mediastinum. The rationale of the aggressive procedure is based on the high involvement of upper mediastinal lymph nodes, especially along the recurrent laryngeal nerves in thoracic esophageal cancer, and improved survival benefits by radical dissection of these nodes [1, 2, 25, 26]. However, both postoperative morbidity and mortality are closely associated with the extensiveness of the lymphadenectomy [3]. Otherwise, chemoradiation should be adopted as an alternative adjuvant therapy to improve the surgical outcomes in advanced thoracic esophageal carcinoma with extensive nodal involvement.
Reduced invasiveness with a thoracoscopic procedure is documented in a radical esophagectomy with extensive lymphadenectomy, which itself is an inherently invasive procedure [5, 7, 8]. Less operative blood loss, fewer respiratory complications, and preserved respiratory vital capacity after thoracoscopic surgery were reported [5–12]. In addition, a magnified operative view may enhance meticulous dissection of lymph nodes, thereby preserving mediastinal structures. Despite these potential merits, it is difficult to achieve better operative exposure during a thoracoscopic esophagectomy in the left lateral decubitus position because the positioning of the patient causes mediastinal organs and structures to shift greatly to the left, the right lung is collapsed by univentilation anesthesia and overlies the esophagus, and exudates collect in the posterior mediastinum of the operative field. A technically skillful assistant must expose the operative views quickly and gently using the forceps and suction. The surgeon’s view of the monitor must be turned upside down to avoid the counterimage when two monitors are set on each side. In this situation, hand-eye coordination cannot be obtained smoothly if a scope-holding assistant does not work correctly. The prone position could improve some of these disadvantages. We were first struck by the superior operative exposure obtained when the patient was placed in the prone position. Mediastinal organs and structures were exposed spontaneously by both gravity and artificial pneumothorax without any help from an assistant. The lung fell away with or without minimal handling. As exudates accumulated in the right anterior thorax, not in the posterior mediastinum of the operative field, intermittent suction of accumulated fluids were usually unnecessary during surgery. In addition, the surgeon’s wrists and shoulder joints were in a neutral position in relation to the forearms and upper arms, minimizing fatigue and maximizing ergonomic function. The view of one monitor standing in a single line to the operative field and the improved surgeon ergonomics contributed to better hand-eye coordination. Therefore, the prone position in minimally invasive esophagectomy may provide many advantages [13, 16] but its efficacy is not fully documented. In this study we described our aggressive procedure and determined the advantages of thoracoscopic esophagectomy in the prone position compared to the left lateral decubitus position, focusing on a lymphadenectomy along the left recurrent laryngeal nerve where lymph node dissection is thought to be important but difficult.
Increased operative exposure with the prone position was greatly improved, even around the left recurrent laryngeal nerve. Our hypothesis was that we could perform a precise and accurate lymph node dissection in this area if the operative field was sufficiently exposed because the dissected area could be strictly defined and traced as described above. In this study we confirmed the hypothesis that adequate identification and exploration of the left subclavicular artery in the posterior aspect of the dissected area could be achieved. We found that the prone position was superior to the left lateral decubitus position in this respect. We also determined the number of thoracoscopically harvested lymph nodes along the left recurrent laryngeal nerve below the aortic arch to the thoracic inlet with an en-bloc excised specimen. We found that the number of the harvested lymph nodes in the prone position was slightly higher, but the difference was not significant. A possible plateau in the skill of dissecting sufficient lymph nodes along the left recurrent laryngeal nerve using thoracoscopy in the left lateral decubitus position may limit the number of dissected lymph nodes despite increased quality of dissection in this area. Nevertheless, we could expect that the dissection of lymph nodes of this area by the prone approach might be much more extensive due to improved operative exposure. We demonstrated that the left paratracheal nodes along the left recurrent laryngeal nerve and infra-aortic nodes, which are considered to be particularly difficult to dissect [27], were visualized and dissected sufficiently with the use of the proper techniques of a thoracoscopy in the prone position. Exposure around the thoracic inlet and of the ventral side of the posterior aspect of the left recurrent laryngeal nerve within this area was accelerated by rolling back the trachea using a forceps that grasped a small piece of gauze rather than retracting the trachea or pressing the forceps as in the left lateral-decubitus position. As a result we could expect lymph nodes along the left recurrent laryngeal nerve to be dissected and the nerve isolated in a more precise way by thoracoscopic esophagectomy in the prone position. We were concerned that the incidence of recurrent nerve palsy would be increased by extensive manipulation of the nerve, but this was not the case. We speculate that precision that was thus achieved by the improved ergonomics of the surgeon and operative exposure also minimized damage to the left recurrent laryngeal nerve.
A mediastinal lymph node dissection is considered to be critically important in ensuring patient survival after a radical esophagectomy [1, 2, 18–21]. The average number of retrieved nodes in the current series was 27, which was nearly identical to that retrieved by open thoracotomic esophagectomy, thus suggesting that thoracoscopic esophagectomy in the prone position is oncologically equivalent to open surgery and the left lateral-decubitus position. Previous studies of thoracoscopic esophagectomy reported mean numbers of dissected and retrieved intrathoracic lymph nodes ranging from 11 [6] to 34 [8]. The numbers of retrieved lymph nodes reported in Japanese studies seem to be larger than those in Western studies [5, 11, 27]. The difference in postoperative survival, especially in cases with nodal involvement, may reflect this difference.
Better operative exposure was not associated with shortened operative time in this series. It does not appear that the operative time depended on the initial learning curve of thoracoscopic esophagectomy in the prone position. The chief surgeon in this study had the experience of over 150 cases of thoracoscopic esophagectomy in the left lateral decubitus position before introduction to the prone position and had been trained in the prone technique at another institute. Fabian et al. [16] also suggested that the learning curve for the prone technique appeared to be relatively short, within the first five cases. It took more time to dissect lymph nodes extensively in the fields requiring sufficient exploration in the prone position. In other reports, the operative times for a thoracoscopic esophagectomy in the prone position were much shorter than those in the present series [13, 16]. However, the number of dissected lymph nodes in those reports was also fewer than that in the present series. The strategy of a lymphadenectomy during an esophagectomy might be quite different. Paraesophageal nodes might be dissected in most cases [16], and the procedure might be determined on a case-by-case basis with or without subcarinal nodes and nodes along the recurrent laryngeal nerves [13]. We took more time to preserve mediastinal organs and structures; i.e., recurrent nerves, bronchial arteries, cardiac branches of the sympathetic nerves, a sheath of trachea, and pulmonary branches of the vagus nerves. Therefore, we must try to reduce the operative time by selecting the dissected portions in each case or by achieving technical advances in dissection. Furthermore, we should assess specific measurements of task performance or surgeon fatigue in future studies to advocate improved surgeon ergonomics.
Despite the prolonged operative time for thoracoscopic esophagectomy in the prone position, the estimated blood loss was lower. The blood loss occurs with either a technical event during mediastinal dissection or injury of intercostal sites. Thoracoscopic surgery itself, by using four or five surgical ports, can minimize damage to the chest wall. Furthermore, a magnified view and superb visualization provided by thoracoscopic surgery allow better identification of mediastinal structures and more meticulous dissection, and consequently an injury to serious vessels can be avoided despite extensive dissection. In addition to these advantages of thoracoscopic surgery, we could expect that increased operative exposure and improved surgeon ergonomics with the prone position may allow precision for both dissection and hemostasis, resulting in less blood loss than in the left lateral decubitus position. Even when there is accidental injury to a serious vessel, as in our experience with the right inferior pulmonary vein, immediate and successful hemostasis could be achieved with the patient in the prone position.
Mortality and morbidity rates were low and acceptable compared to the rates in recent reports on open surgery [28–30] and even in reports on thoracoscopic procedures in the left lateral decubitus position [6–12, 27]. The incidence of respiratory complications in the prone position was 15%. This is equivalent to that of the left lateral decubitus position and is much lower than that reported for open surgery [31, 32]. Minimal manipulation of the right lung as well as early recovery after thoracoscopic surgery prevented pulmonary complications. Because respiratory complications are the most common problem leading to prolonged hospital stay or postoperative mortality after a thoracoabdominal esophagectomy, we expected that performance of a thoracoscopic procedure in the prone position would have a positive effect on the incidence of respiratory complications. In the present series, differences in respiratory complications in the prone position compared to the lateral decubitus position were not apparent. A minimally invasive esophagectomy by means of thoracoscopy in the left lateral decubitus position and laparoscopy already facilitates early recovery from postoperative damage enough to minimize postoperative respiratory complications. Therefore, we failed to demonstrate striking efficacy with the prone position compared to the combined thoracoscopic and laparoscopic procedure. Careful selection of patients without preoperative impaired respiratory function or anticancer therapy might make the clinical efficacy of a minimally invasive esophagectomy more apparent by limiting the surgical invasiveness of a radical esophagectomy.
Obvious disadvantages of the prone position include emergent or elective conversion to open surgery and the need for an assistant to expose the operative field or retract the organs. However, no such conversions were required in this series. In one patient, there was an injury to the right inferior pulmonary vein, but we were able to immediately grasp the bleeding point just before a massive hemorrhage and close a hole in the pulmonary vein by suturing. Improved handling and better operative exposure with the prone position permitted the critical situation to be resolved. Emergent conversion to a posterior thoracotomy could be performed in this position but would not be a familiar surgical approach. If it was an elective conversion, not due to an emergency, it might be better for the patient to be placed in the left lateral decubitus position. A thoracoscopic esophagectomy in the prone position is carried out almost in a solo-surgery fashion with minimal help from an attending assistant. Technically skillful help from an assistant would allow the surgeon to dissect more precisely and quickly. However, our current prone procedures permit an assistant to use only a single port which is difficult to handle.
We conclude that a thoracoscopic esophagectomy in the prone position is technically safe and feasible and provides good surgeon ergonomics and excellent operative exposure around the left recurrent laryngeal nerve. By meticulous dissection with the patient in the prone position, the blood loss or the incidence of recurrent nerve palsy is not increased despite extensive manipulation of the nerve. Except for the operative time, the present results do not show disadvantages with thoracoscopic esophagectomy in the prone position. We believe that improved visualization and a magnified view provided by thoracoscopy in the prone position would possibly prove more advantageous during an aggressive esophagectomy with extensive dissection of lymph nodes in a long-term result.
References
Akiyama H, Tsurumaru M, Udagawa H, Kajiyama Y (1994) Radical lymph node dissection for cancer of the thoracic esophagus. Ann Surg 220(3):364–372
Fujita H, Kakegawa T, Yamana H, Shima I, Toh Y, Tomita Y, Fujii T, Yamasaki K, Higaki K, Noake T et al (1995) Mortality and morbidity rates, postoperative course, quality of life, and prognosis after extended radical lymphadenectomy for esophageal cancer. Comparison of three-field lymphadenectomy with two-field lymphadenectomy. Ann Surg 222(5):654–662
Watson A (1994) Operable esophageal cancer: current results from the West. World J Surg 18(3):361–366
Cuschieri A, Shimi S, Banting S (1992) Endoscopic oesophagectomy through a right thoracoscopic approach. J R Coll Surg Edinb 37(2):7–11
Akaishi T, Kaneda I, Higuchi N, Kuriya Y, Kuramoto J, Toyoda T, Wakabayashi A (1996) Thoracoscopic en bloc total esophagectomy with radical mediastinal lymphadenectomy. J Thorac Cardiovasc Surg 112(12):1533–1540
Smithers BM, Gotley DC, McEwan D, Martin I, Bessell J, Doyle L (2001) Thoracoscopic mobilization of the esophagus. A 6 year experience. Surg Endosc 15(2):176–182
Taguchi S, Osugi H, Higashino M, Tokuhara T, Takada N, Takemura M, Lee S, Kinoshita H (2003) Comparison of three-field esophagectomy for esophageal cancer incorporating open or thoracoscopic thoracotomy. Surg Endosc 17(9):1445–1450
Osugi H, Takemura M, Higashino M, Takada N, Lee S, Kinoshita H (2003) A comparison of video-assisted thoracoscopic oesophagectomy and radical lymph node dissection for squamous cell cancer of the oesophagus with open operation. Br J Surg 90(1):108–113
Luketich JD, Alvelo-Rivera M, Buenaventura PO, Christie NA, McCaughan JS, Litle VR, Schauer PR, Close JM, Fernando HC (2003) Minimally invasive esophagectomy. Outcomes in 222 patients. Ann Surg 238(4):486–495
Braghetto I, Csendes A, Cardemil G, Burdiles P, Korn O, Valladares V (2006) Open transthoracic or transhiatal esophagectomy versus minimally invasive esophagectomy in terms of morbidity, mortality and survival. Surg Endosc 20(11):1681–1686
Smithers BM, Gotley DC, Martin I, Thomas JM (2007) Comparison of the outcomes between open and minimally invasive esophagectomy. Ann Surg 245(2):232–240
Berrisford RG, Wajed SA, Sanders D, Rucklidge MWM (2008) Short-term outcomes following total minimally invasive oesophagectomy. Br J Surg 95(5):602–610
Palanivelu C, Prakash A, Senthikumar R, Senthilnathan P, Parthasarathi R, Rajan PS, Venkatachlam S (2006) Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position - experience of 130 patients. J Am Coll Surg 203(1):7–16
Fabian T, McKelvey AA, Kent MS, Federico JA (2007) Prone thoracoscopic esophageal mobilization for minimally invasive esophagectomy. Surg Endosc 21(9):1667–1670
Cadière GB, Torres R, Dapri G, Capelluto E, Hainaux B, Himpens J (2006) Thoracoscopic and laparoscopic oesophagectomy improves the quality of extended lymphadenectomy. Surg Endosc 20(8):1308–1309
Fabian T, Martin J, Katigbak M, McKelvey AA, Federico JA (2008) Thoracoscopic esophageal mobilization during minimally invasive esophagectomy: a head-to-head comparison of prone versus decubitus positions. Surg Endosc 22(11):2485–2491
Noshiro H, Nagai E, Shimizu S, Uchiyama A, Kojima M, Tanaka M (2007) Minimally invasive radical esophagectomy for esophageal cancer. Esophagus 4(1):59–65
Watanabe H, Kato H, Tachimori Y (2000) Significance of extended systemic lymph node dissection for thoracic esophageal carcinoma in Japan. Recent Results Cancer Res 155:123–133
Shiozaki H, Yano M, Tsujinaka T, Inoue M, Tamura S, Doki Y, Yasuda T, Fujiwara Y, Monden M (2001) Lymph node metastasis along the recurrent nerve chain is an indication for cervical lymph node dissection in thoracic esophageal cancer. Dis Esophagus 14(3–4):191–196
Tsurumaru M, Kajiyama Y, Udagawa H, Akiyama H (2001) Outcomes of extensive lymph node dissection for squamous cell carcinoma of the thoracic esophagus. Ann Thoracic Cardiovasc Surg 7(6):325–329
Nishimaki T, Suzuki T, Tanaka Y, Nakagawa S, Aizawa K, Hatakeyama K (1997) Evaluating the rational extent of dissection in radical esophagectomy for invasive carcinoma of the thoracic esophagus. Surg Today 27(1):3–8
Lerut T, Nafteux P, Moons J, Coosemans W, Decker G, De Leyn P, Van Raemdonck D, Ectors N (2004) Three-field lymphadenectomy for carcinoma of the esophagus and gastroesophageal junction in 174 R0 resections: impact on staging, disease-free survival, and outcome: a plea for adaptation of TNM classification in upper-half esophageal carcinoma. Ann Surg 240(6):962–974
Snedecor GW, Cochran WG (1980) Statistical methods. Iowa State University Press, Ames
Cuschieri A (1994) Thoracoscopic subtotal oesophagectomy. Endosc Surg Allied Technol 2(1):21–25
Isono K, Sato H, Nakayama K (1991) Results of nationwide study on the three-field lymph node dissection of esophageal cancer. Oncology 48(5):411–420
Igaki H, Tachimori Y, Kato H (2004) Improved survival for patients with upper and/or middle mediastinal lymph node metastasis of squamous cell carcinoma of the lower thoracic esophagus treated with 3-field dissection. Ann Surg 239(4):483–490
Peracchia A, Rosati R, Fumagalli U, Bona S, Chella B (1997) Thoracoscopic dissection of the esophagus for cancer. Int Surg 82(1):1–4
Swanson SJ, Batirel HF, Bueno R, Jaklitsch MT, Lukanich JM, Allred E, Mentzer SJ, Sugarbaker DJ (2001) Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg 72(6):1918–1924
Gluch L, Smith RC, Bambach CP, Brown AR (1999) Comparison of outcomes following transhiatal or Ivor Lewis esophagectomy for esophageal carcinoma. World J Surg 23(3):271–275
Orringer MB, Marshall B, Iannettoni MD (1999) Transhiatal esophagectomy: clinical experience and refinements. Ann Surg 230(3):392–400
Crozier TA, Sydow M, Siewert JR, Braun U (1992) Postoperative pulmonary complication rate and long-term changes in respiratory function following esophagectomy with esophagogastrostomy. Acta Anaesthesiol Scand 36(1):10–15
Ferguson MK, Martin TR, Reeder LB, Olak J (1997) Mortality after esophagectomy: risk factor analysis. World J Surg 21(6):599–603
Acknowledgment
The authors are grateful for the technical training and ongoing advice on the prone procedures by Professors Ichiro Uyama and Seiichiro Kanaya in the Department of Surgery of Fujita Health University School of Medicine.
Disclosures
Drs. Hirokazu Noshiro, Tomonori Iwasaki, Kiitiro Kobayashi, Akihiko Uchiyama, Yoshihiro Miyasaka, Toshihiro Masatsugu, Kenta Koike, and Koji Miyazaki have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Noshiro, H., Iwasaki, H., Kobayashi, K. et al. Lymphadenectomy along the left recurrent laryngeal nerve by a minimally invasive esophagectomy in the prone position for thoracic esophageal cancer. Surg Endosc 24, 2965–2973 (2010). https://doi.org/10.1007/s00464-010-1072-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1072-4