
Abstract
Background
Music and noise are frequent occurrences in the operating room. To date, the effects of these auditory conditions on the performance of laparoscopic surgery experts have not been evaluated.
Methods
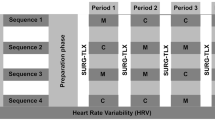
Eight internationally recognized experts were recruited for a crossover study. The experts were randomized to perform three simple tasks on a laparoscopic simulator, SurgicalSIM VR. The tasks were equal in difficulty and performed under the following conditions: silence, dichaotic music (auditory stress), classical music (auditory relaxation), and mental loading (mental arithmetic tasks). Permutations of the conditions were created to account for a learning effect. The tasks were performed twice to test for memory consolidation and to accommodate baseline variability. Time until task completion and task accuracy via instrument tip trajectory (path of the tip through space) were recorded. Performance was correlated with responses on the Brief Musical Experience Questionnaire (MEQ).
Results
The study demonstrated that dichaotic music has a negative impact on time until task completion but not on task accuracy. In addition, memory consolidation of accuracy is negatively influenced. Classical music has a variable effect on experts’ time until task completion, yet all the experts performed the tasks more accurately. Classical music had no effect on recall of a procedure. Mental loading increased time until completion, but did not affect accuracy or recall. The experience of music varied among experts and influenced how each of the conditions affected their performance.
Conclusion
The study demonstrated that, contrary to common belief, proficiency in surgery does not protect against stressful auditory influences or the influence of mental preoccupation. Interestingly, relaxing auditory influences such as classical music can even have a positive impact on the accuracy of experts. Previous musical experience could help to identify surgeons whose performance may be specifically affected by music or noise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Although both soothing and stressful auditory conditions commonly exist in the operating room, their influence on laparoscopic motor skill performance and memory consolidation remains poorly understood. Furthermore, it remains unclear whether the impact of stressful auditory stimuli is similar or different from that of mental loading (i.e., mental preoccupation with something other than the current surgical task). Although stress, in general, is recognized as a significant factor affecting performance in aviation and in the military, the influence of auditory stress on surgical performance remains poorly understood [1–5].
Noise pollution in the operating room has been identified as a cause of stress [6–8]. The noise levels as high as 80 to 85 dB have been measured in the operating room, which is twice the recommended standard of 45 dB for a working environment. Especially during neurosurgical and orthopedic procedures, peak levels of noise can be as high as 100 to 120 dB, which has been demonstrated to affect necessary communication in the operating room. For theater staff, this noise can lead to impaired concentration and performance, interference with communication, and increased levels of stress. Additionally, patients who are conscious for part or all of their time in the operating theater may become more anxious because of the noise [9]. Noise in the operating room environment also could have a negative impact on surgeons’ performance of surgical procedures [10, 11].
The effect of noise on laparoscopic performance has been controversial. One study showed that background noise at 113 dB had a negative impact on surgical laparoscopic performance [11], whereas another study on the effect of noise and background music showed no difference in task performance in terms of the time taken to complete a task [10] In other studies, music has had a positive impact on surgeons and their performance. Surgeon-selected music has been associated with reduced autonomic reactivity and improved performance of a stressful nonsurgical laboratory task [12].
Large animal studies also have yielded conflicting evidence regarding the value of classical music and enhancement of performance. With monkeys, for example, Mozart’s piano music led to worse performance in a delayed response task, whereas white noise led to improvement [13].
In this study, we examined the effect of external auditory stimuli, namely, auditory stress (dichaotic music) and auditory relaxation (classical music), on the laparoscopic motor skill performance of experts and compared the results with the effects of internal stresses on mental loading via arithmetic tasks. Furthermore, we related the degree of effect that the experimental conditions had on the performance of these laparoscopic experts to their reports of how they experience music in their lives. This correlation was established using the Music Experience Questionnaire (MEQ), a self-report measure of individual differences in reactions to music. This questionnaire has been used in a number of studies to assess the place of music in the lives of people in the United States, Australia, Greece, Israel, Hungary, and Lithuania.
The MEQ consists of 53 items (questions) that test for following six scales: Commitment to Music (the centrality of pursuit of musical experiences in the person’s life), Innovative Musical Aptitude (self-reports of musical performance ability as well as the ability to generate musical themes and works), Social Uplift (the experience of being stirred and uplifted in a group-oriented manner by music), Affective Reactions (affective and spiritual reactions to music), Positive Psychotropic Effects (calming, energizing, integrating reactions), and Reactive Musical Behavior (motile reactions including humming and swaying along with music). Replicated results using the principal factors method have identified two factors that underlie the questionnaire: subjective and physical reaction to music and active involvement. We tested for these factors independently from the six MEQ scales.
Materials and methods
Eight internationally renowned experts of laparoscopy were asked to complete four simple tasks on the surgical computerized laparoscopy simulator, SurgicalSIM VR (Medical Education Technologies, Inc., Sarasota, Fl, USA). For each task, the simulator recorded time until task completion as well as accuracy, measured as the instrument tip trajectory. The simulator measured the distance the instrument tip traveled through space, which was reduced with increased accuracy. The tasks were equal in difficulty, and permutations of task order were performed to avoid the systematic error of a learning effect. Each task was repeated after a 10-min interval to allow testing for memory consolidation of the motor performance. During the 10-min interval, each expert was engaged in an “everyday” conversation or in simple manual tasks to distract his or her mind from the task.
The tasks were completed under the following four conditions:
-
1.
Silence.
-
2.
Dichaotic music, in which a different type of music was heard through each ear (“death metal” style music was heard in one ear and German vocal folk music in the other ear). The stress level of the dichaotic music was heightened by having inverse dynamic lines, for example, melodic lines in the left ear complementing those in the right ear during short breaks.
-
3.
Mental loading, which required the expert to solve simple math problems read to him or her in a standardized fashion. Answers had to be given as rapidly as possible. If there were more than 3 s of silence or the answer was incorrect, the question was repeated.
-
4.
Classical music by Mozart. We chose slow movements of the piano sonatas, which we have been previously shown to have relaxing compositional elements [14].
The expert was exposed to each condition both the first time the task was performed and during the repeat performance. The auditory stimuli were applied in a standardized fashion via headphones at equal noise pressure levels. Aspects of the musical experience were quantified via the reliable Brief Music Experience Questionnaire (MEQ), which has been researched in six countries [15]. Briefly, this questionnaire assesses six aspects of music experience summarized by two dimensions: Subjective/Physical Reactions to music (e.g., emotional reactions) and Active Involvement in music (cognitive/behavioral involvement). Descriptive statistical analysis was performed using SPSS Inc 16.0 (SPSS, Chicago, IL, USA).
Results
Speed
Time until task completion was increased for most of the experts when listening to dichaotic music or being mentally loaded (Fig. 1). However, listening to classical music led to improved performance. This was most evident for expert 6, who had an overall longer time until task completion but a reduction in time until completion while listening to classical music. Interestingly, the results for memory consolidation demonstrated a pattern quite different from the first time the task was completed. Most of the experts showed decreased improvement in task completion time when performing the task the second time under dichaotic music in comparison with a repeat performance in silence.

Results of the laparoscopic performance under the test conditions. The data describe motor skill performance under the conditions of (a) silence, (b) dichaotic music, (c) mental loading, and (d) Mozart music. A Baseline time until completion. B Time until task completion after a 10-min break. C Trajectory (directly correlated with accuracy) at baseline and D after a 10-min interval. E Data for relative improvement with respect to time and F with respect to accuracy
Mental loading led to worse task performance: Four experts had even longer task completion time in their second session of mental loading although they had completed the task in only 10 min previously. There was great diversity with respect to memory consolidation of experts listening to classical music. Whereas one expert improved his time until completion by 50%, another expert’s time became 30% worse.
Accuracy also was influenced by the various auditory conditions. There was a difference exceeding 200% in accuracy among the experts when the task was performed in silence. During silence, two of six experts did not improve, whereas the remainder of the experts improved 10 to 50%. When exposed to dichaotic music, six of the eight experts showed improved accuracy. In repeat task performance, the accuracy of two experts worsened with dichaotic music compared with silence, and the overall improvement secondary to repetition was less than during silence. Again, six of the eight experts (different experts than those under dichaotic music) showed worse performance during mental loading. Five of the eight experts were able to improve their performance relative to silence. All except one expert was able to improve their trajectory from the first to the second session of mental loading.
Interestingly, the accuracy exhibited by seven of the eight experts was better during classical music than during all the other conditions. Although the experts had the most accurate performance while listening to classical music, five experts improved and three experts worsened their performance during task repetition. A comparison of relative improvement between the test conditions of silence and dichaotic music showed that the expert who improved the most during silence (60%) had the worst recall during dichaotic music (−50%).
Response to music in general
The study findings showed both similarities and differences among the experts in their reports of music experience in general on the six scales of the MEQ (Fig. 2A) and on the MEQ’s summary factors (Fig. 2B). To show these experts’ standing on the music variables relative to the set of all experts, the results shown in Fig. 2B, D are standardized so that 1 unit is a standard deviation. Although commitment to music was generally low in the cohort of experts, all of them showed strong affective reactions to music. Two experts showed distinct patterns of performance both across conditions (Fig. 2C) and across the dimensions of music experience measured by the MEQ (Fig. 2D). A look at relative performance under the two auditory conditions (dichaotic music and Mozart) shows that expert 7 was more negatively affected by dichaotic music and improved the most while listening to Mozart. Expert 2 was relatively less negatively affected by dichaotic music but had worsened recall while listening to Mozart music.

Aspects of all experts’ responses to music (A and B), and of two experts differing in their laparoscopic performance across conditions (C and D). Comparison of the data on the Music Experience Questionnaire representing aspects of the response to music in general and of all the experts as well as experts 2 and 7 in standardized form. (A and C) Results for six scales (Commitment to Music, Innovative Musical Aptitude, Social Uplift, Affective Reactions, Positive Psychotropic Effects, Reactive Musical Behavior) and (B and D) two factors (Subjective/Physical Reactions to Music and Active Involvement in Music). A higher score indicates greater endorsement of an aspect of response to music. The y-axis of A represents scores computed as the mean response across a scale’s items using the MEQ’s 5-point response scale ranging from 1 (very untrue) to 5 (very true). Scores on the y-axis of C are factor scores (with mean equaling 0 in a reference sample). The y-axis in B and D depicts standard deviations on the scales (B) and factors relative to group performance (D)
Expert 2, with an interestingly low social uplift value on the MEQ, and expert 7 show a contrast in their different MEQ values. From the perspective of scores on the MEQ’s six scales, expert 2 reported relative noninvolvement in group-oriented or social aspects of musical activities, whereas expert 7 highlighted his or her musical abilities as well as music’s effects on activation (e.g., calming or energizing effects) and motile reactions to music. From the perspective of scores on the MEQ’s summary factors, expert 2 had a distinctively low score for the factor representing subjective and emotional reactions, whereas expert 7 had a distinctively high score for the factor representing cognitive, social, intellectualized, and instrumental aspects of music experience. Expert 2, who reported a low emotional reaction to music, was the least affected by dichaotic music in terms of speed and accuracy. Expert 7, on the other hand, with very high scores for cognitive, social, intellectualized, and instrumental aspects of prior music experience, had the second greatest improvement in time until completion of all the experts during classical music.
Discussion
Contrary to common belief, extremely high proficiency in performing laparoscopic surgery does not lead to immunity against the impact of common auditory stimuli in the operating room. We have shown that dichaotic music can lead to worse performance with respect to time until task completion, task accuracy, and recall of a performed task. Mental loading had a greater effect on time until task completion than on accuracy but did not appear to affect recall as much. We believe that the performance under these two adverse conditions, dichaotic music and mental loading, was somewhat confounded by the fact that the experts perceived these conditions as a challenge. Therefore, the improved performance of some experts with dichaotic music versus silence might be explained by their greater effort under the adverse condition. A comparison of the two stressors, dichaotic music and mental loading, seemed to suggest that mental loading uniformly leads to prolonged time until completion, whereas accuracy seems to be affected in a variable degree, with some experts performing more accurately when mentally loaded than when exposed to dichaotic music. These interesting findings warrant further investigation with a larger cohort.
Previous findings have shown that music by Mozart leads to relaxation, and relaxation can lead to improved performance [10, 12]. We found this effect to be more pronounced for time until task completion. Why there was less effect on accuracy than on time could be studied in further research. Aspects of the role that music plays in the experts’ lives and of their reactions to music appear related to their patterns of performance under the auditory conditions in this research. This finding suggests that if the study is replicated with a larger sample, self-reports of music experience may form a basis for identifying surgeons whose laparoscopic performance is particularly affected by conditions of auditory stress in the operating room, and for whom special training in working under auditory stress could be provided.
Although this case–control study begins to elucidate some of the effects auditory influences have on laparoscopic performance, it seems to have raised more questions than it has answered. What are the effects of the auditory conditions on laparoscopic surgery beginners and on performance of other forms of surgery? Would music by composers other than Mozart or music chosen by the experts as being relaxing work better at inducing relaxation and lead to better performance? How are these effects mediated? By what mechanism do responses to music in general relate to performance under various auditory conditions and how can this mechanism be taken into account to improve performance? These questions warrant more follow-up studies using larger cohorts.
Although auditory stressors and the use of music are common environmental factors in the operating room, little understanding exists with regard to their effects on surgical performance. Understanding and recognizing these effects could be a powerful tool for creating an operative environment that is safer and geared toward the best possible patient outcome.
References
Sexton JB, Helmreich RL (2000) Analyzing cockpit communications: the links between language, performance, error, and workload. Hum Perform Extrem Environ 5:63–68
Sexton JB, Thomas EJ, Helmreich RL (2000) Error, stress, and teamwork in medicine and aviation: cross-sectional surveys (clinical research editorial). BMJ 320:745–749
Wallenius C, Larsson G, Johansson CR (2004) Military observers’ reactions and performance when facing danger. Military Psychol 16:211–229
Goodell KH, Cao CG, Schwaitzberg SD (2006) Effects of cognitive distraction on performance of laparoscopic surgical tasks. J Laparoendosc Adv Surg Tech 16:94–98
Bell AK, Zhou M, Schwaitzberg SD, Cao CG (2009) Using a dynamic training environment to acquire laparoscopic surgery skill. Surg Endosc 23(10):2356–2363
Shankar N, Malhotra KL, Ahuja S, Tandon OP (2001) Noise pollution: a study of noise levels in the operation theatres of a general hospital during various surgical procedures. J Indian Med Assoc 99:246–247
Hodge B, Thompson JF (1990) Noise pollution in the operating theatre. Lancet 335:891–894
Ray CD, Levinson R (1992) Noise pollution in the operating room: a hazard to surgeons, personnel, and patients. J Spinal Disord 5:485–488
Falk SA, Woods NF (1973) Hospital noise levels and potential health hazards. N Engl J Med 289:774–781
Moorthy K, Munz Y, Undre S, Darzi A (2004) Objective evaluation of the effect of noise on the performance of a complex laparoscopic task. Surgery 136:25–30 discussion 31
Moorthy K, Munz Y, Dosis A, Bann S, Darzi A (2003) The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg Endosc 17:1481–1484
Allen K, Blascovich J (1994) Effects of music on cardiovascular reactivity among surgeons. JAMA 272:882–884
Carlson S, Rama P, Artchakov D, Linnankoski I (1997) Effects of music and white noise on working memory performance in monkeys. Neuroreport 8:2853–2856
Conrad C, Niess H, Jauch KW, Bruns CJ, Hartl WH, Welker L (2007) Overture for growth hormone: requiem for interleukin-6? Crit Care Med 35(12):2709–2713
Werner PD, Swope AJ, Heide FJ (2006) The music experience questionnaire: development and correlates. J Psychol 140:329–345
Disclosures
Claudius Conrad, Yusuf Konuk, Paul Werner, Caroline G. Cao, Andrew Warshaw, David Rattner, Daniel B. Jones, and Denise Gee have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Conrad, C., Konuk, Y., Werner, P. et al. The effect of defined auditory conditions versus mental loading on the laparoscopic motor skill performance of experts. Surg Endosc 24, 1347–1352 (2010). https://doi.org/10.1007/s00464-009-0772-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0772-0