
Abstract
Background
Ventriculoperitoneal shunt (VPS) is the mainstay of therapy for hydrocephalus. The aim of this study is to compare outcomes of laparoscopic (LVPS) versus open (OVPS) techniques for placement of distal VPS catheters.
Methods
All patients undergoing new VPS placement at a tertiary care center between January 2004 and August 2007 were included. Univariate analysis was performed. Wilcoxon rank-sum, chi-square, and Fisher’s exact tests were used to make comparisons between LVPS and OVPS groups. Stepwise backward logistic regression was performed to predict complications requiring operative intervention. A Kaplan–Meier estimate of the survival function was calculated for shunt survival. All data is presented as median and range unless otherwise specified.
Results
Five hundred thirty-five consecutive patients underwent 579 VPS (258 LVPS, 321 OVPS). Median age (52.0 years) and American Society of Anesthesiologists (ASA) score (3) were similar in LVPS and OVPS groups. Body mass index (BMI) [27.8 (17.0–64.9) kg/m2 versus 25.9 (12.3–44.4) kg/m2, p = 0.007], previous operations [0.8 ± 0.9 versus 0.6 ± 0.7, p = 0.004 (mean ± standard deviation)], estimated blood loss (EBL) [20 (0–175) ml versus 25 (0–500) ml, p < 0.001], operating room (OR) time [37.5 (17.0–152.0) min versus 52.0 (20.0–197.0) min, p < 0.001], and length of stay (LOS) [11 (1–77) days versus 14 (1–225) days, p = 0.016] were statistically different between the LVPS and OVPS groups, respectively. LVPS abdominal complication rate of 5.8% and OVPS rate of 6.9% were similar (p = 0.611). Previous abdominal operation [odds ratio (OR) 1.673, 95% confidence interval (CI) 1.100–2.543, p = 0.016] and previous VPS (OR 1.929, 95% CI 1.147–3.243, p = 0.016) were significant predictors of complications requiring operative intervention. Kaplan–Meier analysis demonstrated no difference in survival between LVPS and OVPS groups (p = 0.538), with overall shunt survival of 86.4% at 6 months and 83.0% at 1 year.
Conclusions
LVPS is associated with decreased OR time, less blood loss, and shorter LOS with no difference in complication rate when compared OVPS. The laparoscopic approach for VPS is a safe, effective, and readily reproducible alternative to the traditional open approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Hydrocephalus is a common and debilitating neurological disorder that is treated primarily with cerebrospinal fluid diversion by ventricular shunt placement. The economic impact of ventricular shunts in the USA has been estimated to be greater than US $1.1 billion per year [1] with a prevalence of more than 125,000 shunts in place [2]. Complications including infection and shunt malfunction are common, with a 1-year failure rate up to 40% [3]. Ventriculoperitoneal shunt placement is the most commonly performed diversion procedure, followed by ventriculopleural and ventriculoatrial shunts.
The placement of the abdominal catheter of a ventriculoperitoneal shunt has traditionally been performed using an open approach via a minilaparotomy of variable length or by blind trocar insertion [4]. In the late 1970s and 1980s, laparoscopy was introduced for retrieval of “lost” distal catheters [5, 6], and has primarily been utilized for shunt revision. Laparoscopy for distal catheter placement in new shunts was described in 1993 [7–9], but has not been used extensively for this purpose.
When compared with the open approach, laparoscopy offers several benefits including direct visualization of distal catheter placement, verification of cerebrospinal fluid (CSF) flow, and the ability to perform lysis of adhesions or retrieve nonfunctioning catheters if necessary. In addition, cosmesis and postoperative pain are improved, formation of peritoneal adhesions is decreased, and risk of incisional hernia is reduced [10–12]. The goal of this study is to compare outcomes of the laparoscopic and open techniques for placement of the abdominal portion of ventriculoperitoneal shunt catheters.
Materials and methods
This is an institutional review board (IRB)-approved (X060331022), retrospective cohort study of consecutive patients undergoing new ventriculoperitoneal shunt placement at the University of Alabama at Birmingham (UAB) Hospital between January 2004 and August 2007. New ventriculoperitoneal shunt placement was defined as placement of a proximal cerebral catheter, new valve, and distal peritoneal catheter. Shunt procedures not meeting these criteria were considered revisions and excluded from this study. A complication was categorized as perioperative if it occurred within 30 days of operation and long term if it occurred more than 30 days postoperatively. The most recent patient encounter (e.g., clinic visit or hospital discharge), shunt removal, and patient death were defined as endpoints for follow-up. In all cases, a laparoscopic or open technique was used for placement of the peritoneal catheter.
Demographic, clinical, and operative data were collected by manual chart review, examination of operative notes, and extraction of records from hospital databases. Independent variables including age, gender, race, previous abdominal operations, previous ventriculoperitoneal shunt placement, indication for operation, ASA score, body mass index, operative technique (laparoscopic or open), operative time, estimated blood loss, and length of stay were collected. Dependent variables including complications requiring shunt revision or removal were obtained.
Univariate statistics were computed for all demographics and variables of interest. Bivariate analyses were performed to examine associations between independent variables and the primary dependent variable, complication requiring operative intervention. Associations of all covariates with the primary independent variable of interest, operative technique, were examined.
Wilcoxon rank-sum tests were used for comparisons of continuous variables by both complication and technique because all distributions violated the assumption of normality. Results are reported as median and range unless otherwise specified. Chi-square tests of proportion were used to examine associations between categorical variables of interest. Fisher’s exact test was used when cell sizes were too small to produce reliable chi-square results. Possible predictors of complications requiring operative intervention were examined using best-fit stepwise manual backward logistic regression analyses, with model fit assessed by Pearson and deviance criteria. Kaplan–Meier survival analysis was performed and Wilcoxon test was used to compare survival of shunts placed using a laparoscopic versus open technique. All statistical analyses were performed using SAS v9.1.3.
Surgical technique
The patient is placed in a supine position and the head, neck, chest, and abdomen are prepped and draped in the usual sterile fashion. During both open and laparoscopic cases, the cranial and abdominal procedures are usually performed concurrently. The neurosurgical team optimally places the ventricular catheter and shunt valve. The tubing is then brought out through a retroauricular incision. A 65-cm malleable tunneling device is used to create a subcutaneous tract from the abdominal incision to the retroauricular incision. The catheter is then connected to the tunneling device and brought through the subcutaneous tract to the abdominal incision in preparation for abdominal placement by either open or laparoscopic approach.
Open abdominal catheter placement is typically performed by a member of the neurosurgical team while another member completes the cranial part of the procedure. A 4–5-cm incision is made in the midline approximately 10 cm inferior to the xyphoid process (a longer incision is made in obese patients). The underlying fascia is exposed and a small incision is made with a scalpel. The fascial incision is extended with Metzenbaum scissors and the preperitoneal fat is moved aside to expose the parietal peritoneum. The peritoneum is grasped with two hemostats and carefully inspected to ensure that no bowel loops are adherent. A small incision is made in the peritoneum with Metzenbaum scissors and extended with a hemostat. The peritoneal cavity is carefully inspected to confirm entry into the abdomen and verify that no visceral injury had occurred. The distal shunt tubing is then placed into the peritoneal cavity under direct visualization. The abdominal incision is then closed in layers with absorbable suture.
The gastrointestinal surgery team performs laparoscopic abdominal catheter placement while the neurosurgery team is placing the cerebral catheter and shunt valve. A 2–3-mm midline epigastric incision is made to facilitate tunneling and catheter placement, and a 5-mm paramedian incision is made approximately 10 cm from the site of the epigastric incision and remote from any previous abdominal incisions. A Veress needle is used to establish pneumoperitoneum to 15 mmHg. An Endopath Xcel trocar (Ethicon Endosurgery, Cincinnati OH, USA) is utilized to gain access to the peritoneum under direct vision. A 5-mm, 30° laparoscope (Endo-Eye, Olympus America Inc., Center Valley, PA, USA) is inserted and the abdomen is explored, noting any pathology or adhesions. If adhesions preventing catheter placement are present or a previous shunt catheter has migrated, a second 5-mm port is placed to lyse adhesions and/or remove the old catheter. The positioning of ports and the incision for catheter tunneling can vary depending on previous abdominal operations and body habitus.
Under direct visualization, an 18-gauge needle is placed through the epigastric incision used for tunneling the shunt onto the abdomen. A guide wire is then placed through the needle and the needle is removed. Using the Seldinger technique, a 10-French peel-away sheath is placed over the guidewire into the peritoneal cavity. The distal part of the catheter is placed through the sheath into the abdomen under direct visualization and shunt function is verified by observing CSF flow from the catheter. The sheath is then peeled away. The incisions are closed using a 4–0 absorbable subcuticular suture and a sterile adhesive is applied for skin closure.
Results
During the study period, 579 consecutive new ventriculoperitoneal shunts were performed. Of these, the distal catheter was placed by open technique in 321 cases and by laparoscopic approach in 258 cases (Table 1). Of ventriculoperitoneal shunt cases, median age was 52.0 (15.7–90.4) years, and 60.3% of cases were performed on White patients. Median BMI was 27.1 (13.3–64.9) kg/m2, and 57.9% of cases were performed on females. Median estimated blood loss was 25.0 (0.0–500.0) ml and median operative time was 45.0 (17.0–197.0) min. Mean follow-up was 13.5 (0.0–48.7) months. In 202 cases (34.9%), previous abdominal operations had been performed, with hysterectomy being the most common procedure. When comparing open and laparoscopic techniques, open procedures were more likely to be performed on White versus non-White patients (66.7% versus 52.3%, p < 0.001). The laparoscopic group had undergone a higher proportion of previous abdominal operations when compared with the open group (29.9% versus 41.1%, p = 0.005).
The most common indications for ventriculoperitoneal shunt were subarachnoid hemorrhage, normal pressure hydrocephalus, tumor, and trauma, and were similar in the open and laparoscopic groups. The majority of cases had an American Society of Anesthesiologists (ASA) score of 3 (74.6%) and there was no significant difference in ASA score between the groups (p = 0.184). The laparoscopic group had higher median BMI (27.7 versus 25.9 kg/m2, p = 0.007) and lower estimated blood loss (20.0 versus 25.0 ml, p < 0.001) when compared with the open group. Median operative time (37.5 versus 52.0 min, p < 0.001) and length of stay (11.0 versus 13.0 days, p = 0.016) were significantly shorter in the laparoscopic group versus open group, respectively. Median follow-up was shorter for the laparoscopic group (10.5 versus 17.0 months, p < 0.001) (Table 2).
The most common complications reported were shunt infection, obstruction, and unspecified malfunctions. There was no significant difference in complications between laparoscopic and open procedures (Table 3). Analysis was performed based on the location where complications occurred, and no difference was noted between groups for any abdominal or cerebral complication (data not presented). Malpositioning of the abdominal catheter, which did not occur in the laparoscopic group, complicated two open cases. Abdominal pain requiring shunt removal occurred in 1.6% of open and 1.3% of laparoscopic cases (p = 1.000).
Operative intervention for complications was necessary in 21.8% of ventriculoperitoneal shunt placement procedures, and was similar between the laparoscopic and open group. Perioperative and long-term complication rates were also similar, as were the rates of abdominal and cerebral complications (Table 4).
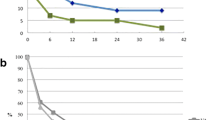
Analysis of data using a best fit stepwise backward logistic regression model suggests that use of a laparoscopic versus open technique for peritoneal catheter placement is not a significant predictor for complications requiring operative intervention. History of abdominal operation (OR 1.673, 95% CI 1.100–2.542, p = 0.016) and previous ventriculoperitoneal shunt placement (OR 1.929, 95% CI 1.147–3.243, p = 0.013) were predictors of complications requiring operative intervention, while age was protective (OR 0.981, 95% CI 0.969–0.992, p = 0.001) (Table 5). Kaplan–Meier survival analysis demonstrated no significant difference in survival between shunts placed using laparoscopic versus open technique (p = 0.538). Overall shunt survival was estimated to be 86.4% at 6 months and 83.0% at 1 year (Fig. 1).

Kaplan–Meier plot of overall ventriculoperitoneal shunt survival
Two intraoperative complications occurred during this series. The first complication occurred during an open procedure when an enterotomy was made upon entering the peritoneal cavity. An intraoperative general surgery consult was obtained and the enterotomy was closed and abdomen thoroughly irrigated. A subdural peritoneal catheter that had been previously placed for a subdural hygroma became infected and was removed 4 days later. After 10 days from the initial bowel injury, a ventriculoatrial shunt was placed and was functioning well 2 years later. The second intraoperative complication occurred during a laparoscopic procedure when the capsule of the liver was punctured by the Veress needle. The wound was hemostatic on initial inspection and prior to closing the abdomen. There were no perioperative complications resulting from this injury. The shunt was removed after 4 months for an abdominal shunt infection. There was no mortality resulting from ventriculoperitoneal shunt placement in this series.
Discussion
This study compares laparoscopic and open approaches to distal catheter placement during ventriculoperitoneal shunt procedures. We found that there was no statistical difference in complication rates between groups. This is consistent with a previous report of 139 open and 38 laparoscopic shunt placements by Roth et al. [13]. Schubert et al. reported a significantly higher rate of abdominal complications in the open group in their series of 50 open and 50 laparoscopic shunt placements [14]. In our study, predictors of complications requiring operative shunt revision or removal are history of previous operation and previous ventriculoperitoneal shunt placement, while increasing age appears to be protective. In addition to similar complication rates, we found that ventriculoperitoneal shunt survival was similar between groups undergoing laparoscopic versus open placement of the abdominal catheter.
Our mean operative time was 25% shorter (41 versus 55 min) and median operative time was 28% shorter (37.5 versus 52 min) in the laparoscopic versus open group, respectively. In other series, mean operative times for shunt placement ranging from 42 to 81 min with laparoscopy [14–20] and 49 to 116 min with an open approach [14, 15] have been reported. Two studies note longer operative times in laparoscopic versus open cases: 59 versus 49 min in one [14] and a range of 35–130 min versus 30–120 min in the other [21]. Interestingly, in a series of 13 complicated laparoscopic abdominal cases, Khosrovi et al. use patients as their own controls by comparing the index laparoscopic procedure (81 min) with a prior open case (116 min) performed by the same surgeon [15].
Duration of ventriculoperitoneal shunt procedures depends on both patient and surgeon factors. Patients who have had previous open abdominal surgery or multiple shunt procedures often require extra time to both lyse adhesions and prevent inadvertent bowel injury. During open abdominal catheter placement, obese patients usually require longer incisions and more involved abdominal closure. Operation time decreases with surgeon experience, which is especially pertinent to laparoscopy as it requires development of a unique skill set.
In most series, as in ours, a general surgeon performs laparoscopic abdominal catheter placement while a neurosurgeon completes the cranial portion of the procedure [14–18, 21]. Operative time can be increased if the schedules of the neurosurgery and general surgery teams are not well coordinated. For uncomplicated cases, the cranial part of the procedure can be done in 10–15 min while the abdominal part can be done in less than 10 min, suggesting that the entire procedure can be completed in 25 min or less [16]. Our mean operative time of 41 min with 15% of cases taking less than 25 min is less than that of other series in the literature [14–19]. This is likely due to efforts to improve efficiency by coordinating surgeon schedules and ensuring that appropriate supplies are readily available when needed.
In addition to decreased operative time, less blood loss, and shorter length of stay, laparoscopy allows the surgeon to explore the abdominal cavity, lyse adhesions if necessary, and note any incidental abdominal pathology. This technique allows the surgeon to verify optimal peritoneal catheter placement and observe cerebrospinal fluid exiting the catheter, confirming functionality. Less inflammation occurs with laparoscopy, which leads to decreased formation of adhesions [12], and may be especially important in younger patients in whom multiple future shunt placements are likely. Compared with minilaparotomy, laparoscopic incisions are usually only 5 mm, leading to improved cosmesis and reduced risk of developing incisional hernias. Postoperative pain is improved and risk of postoperative ileus is decreased with the laparoscopic approach [11], resulting in shorter length of stay when compared with minilaparotomy.
Our study has several limitations. First, laparoscopic placement of the distal ventriculoperitoneal shunt catheter is thought to be beneficial for complicated patients who are obese or have dense intra-abdominal adhesions [11, 15]. In our series, the group undergoing laparoscopy had significantly higher median BMI and increased proportion of previous abdominal procedures, which may represent selection bias. Regardless, there was no difference in complications between laparoscopic and open procedures, while operative time, blood loss, and length of stay were less in the laparoscopic group. Second, this is a retrospective study conducted at a tertiary care academic medical center with both general surgery and neurosurgery residents and a laparoscopic fellowship program. Our results, therefore, may not be easily reproduced by other surgeons or institutions where these resources are not available. Third, because patients were identified through querying hospital databases, there is the possibility of misclassification bias. Finally, financial data is not analyzed. Reimbursement is obtained by using a billing code for a second surgeon, so financial arrangements must be negotiated between surgeons who perform this procedure. Cost–benefit analysis on laparoscopic versus open ventriculoperitoneal distal catheter placement represents an avenue for further exploration.
Conclusions
Laparoscopic technique for distal catheter placement during ventriculoperitoneal shunt procedures is associated with decreased operative time, less blood loss, and shorter length of stay with no difference in complication profile or shunt survival when compared with traditional minilaparotomy. Furthermore, the use of laparoscopy allows verification of catheter placement and function while resulting in better aesthetic results, decreased postoperative pain, and virtually no risk of incisional hernia development. Laparoscopic placement of the distal catheter during ventriculoperitoneal shunt placement is a safe, effective, and reproducible procedure, and represents a viable alternative to open catheter placement. Close communication and coordination between the general surgeon and neurosurgeon is crucial when using laparoscopy to place the abdominal portion of ventriculoperitoneal shunt catheters.
References
Patwardhan RV, Nanda A (2005) Implanted ventricular shunts in the United States: the billion-dollar-a-year cost of hydrocephalus treatment. Neurosurgery 56:139–144
Bondurant CP, Jimenez DF (1995) Epidemiology of cerebrospinal fluid shunting. Pediatr Neurosurg 23:254–258
Kestle J, Drake J, Milner R, Sainte-Rose C, Cinalli G, Boop F, Piatt J, Haines S, Schiff S, Cochrane D, Steinbok P, MacNeil N (2000) Long-term follow-up from the shunt design trial. Pediatr Neurosurg 33:230–236
Lockhart C, Selman W, Rodziewicz G, Spetzler RF (1984) Percutaneous insertion of peritoneal shunt catheters with use of the Veress needle. Technical note. J Neurosurg 60:444–446
Lemay JL, Dupas JL, Capron JP, Robine D (1979) Laparoscopic removal of the distal catheter of ventriculoperitoneal shunt (Ames valve). Gastrointest Endosc 25:162–163
Guzinski GM, Meyer WJ, Loeser JD (1982) Laparoscopic retrieval of disconnected ventriculoperitoneal shunt catheters. Report of four cases. J Neurosurg 56:587–589
Armbruster C, Blauensteiner J, Ammerer HP, Kriwanek S (1993) Laparoscopically assisted implantation of ventriculoperitoneal shunts. J Laparoendosc Surg 3:191–192
Basauri L, Selman JM, Lizana C (1993) Peritoneal catheter insertion using laparoscopic guidance. Pediatr Neurosurg 19:109–110
Schievink WI, Wharen RE Jr, Reimer R, Pettit PD, Seiler JC, Shine TS (1993) Laparoscopic placement of ventriculoperitoneal shunts: preliminary report. Mayo Clin Proc 68:1064–1066
Jea A, Merdas A, Bonnard A (2007) Laparoscopy-assisted ventriculoperitoneal shunt surgery in children: a series of 11 cases. J Neurosurg (6 Suppl Pediatrics):421–425
Kirshtein F, Benifla M, Roy-Shapira A, Merkin V, Melamed I, Cohen Z, Cohen A (2004) Laparoscopically guided distal ventriculoperitoneal shunt placement. Surg Laparosc Endosc Percutan Tech 14:276–278
Szabo G, Miko I, Nagy P, Braith E, Peto K, Furka I, Gamal E (2007) Adhesion formation with open versus laparoscopic cholecystectomy: an immunologic and histologic study. Surg Endosc 21:253–257
Roth J, Boaz S, Amir S, Hanoch E (2007) Laparoscopic versus non-laparoscopic-assisted ventriculoperitoneal shunt placement in adults. A retrospective analysis. Surg Neurol 68:177–184
Schubert F, Fijen B, Krauss J (2005) Laparoscopically assisted peritoneal shunt insertion in hydrocephalus: a prospective controlled study. Surg Endosc 19:1588–1591
Khosrovi H, Kaufman H, Hrabovsky E, Bloomfield S, Prabhu V, El-Kadi H (1998) Laparoscopic-assisted distal ventriculoperitoneal shunt placement. Surg Neurol 49:127–135
Turner R, Rosenblatt S, Chand B, Luciano M (2007) Laparoscopic peritoneal catheter placement: results of a new method in 111 patients. Neurosurgery 61:167–172
Reimer R, Wharen R, Pettit P (1998) Ventriculoperitoneal shunt placement with video-laparoscopic guidance. J Am Coll Surg 187:637–639
Roth J, Park A, Gewirtz R (2000) Minilaparoscopically assisted placement of ventriculoperitoneal shunts. Surg Endosc 14:461–463
Reardon P, Scarborough T, Matthews B, Marti J, Preciado A (2000) Laparoscopically assisted ventriculoperitoneal shunt placement using 2-mm instrumentation. Surg Endosc 14:585–586
Khaitan L, Brennan E (1999) A laparoscopic approach to ventriculoperitoneal shunt placement in adults. Surg Endosc 13:1007–1009
Bani A, Telker D, Hassler W, Grundlach M (2006) Minimally invasive implantation of the peritoneal catheter in ventriculoperitoneal shunt placement for hydrocephalus: analysis of data in 151 consecutive adult patients. J Neurosurg 105:869–872
Acknowledgement
This project was supported in part by Grant Number T32HS013852 from the Agency for Healthcare Research and Quality.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Argo, J.L., Yellumahanthi, D.K., Ballem, N. et al. Laparoscopic versus open approach for implantation of the peritoneal catheter during ventriculoperitoneal shunt placement. Surg Endosc 23, 1449–1455 (2009). https://doi.org/10.1007/s00464-008-0245-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0245-x